Diagnosing Listeria: Blood Cultures, CSF, and Food Testing
- Blood Cultures: The Gold Standard
- CSF Culture for Meningitis
- Gram Stain Appearances
- The Cephalosporin Trap
- NAAT and PCR for Listeria
- Food Testing by Regulatory Agencies
- Whole-Genome Sequencing in Outbreak Investigation
- Stool Culture: Limitations
- When to Test Versus Empirically Treat
- Connections
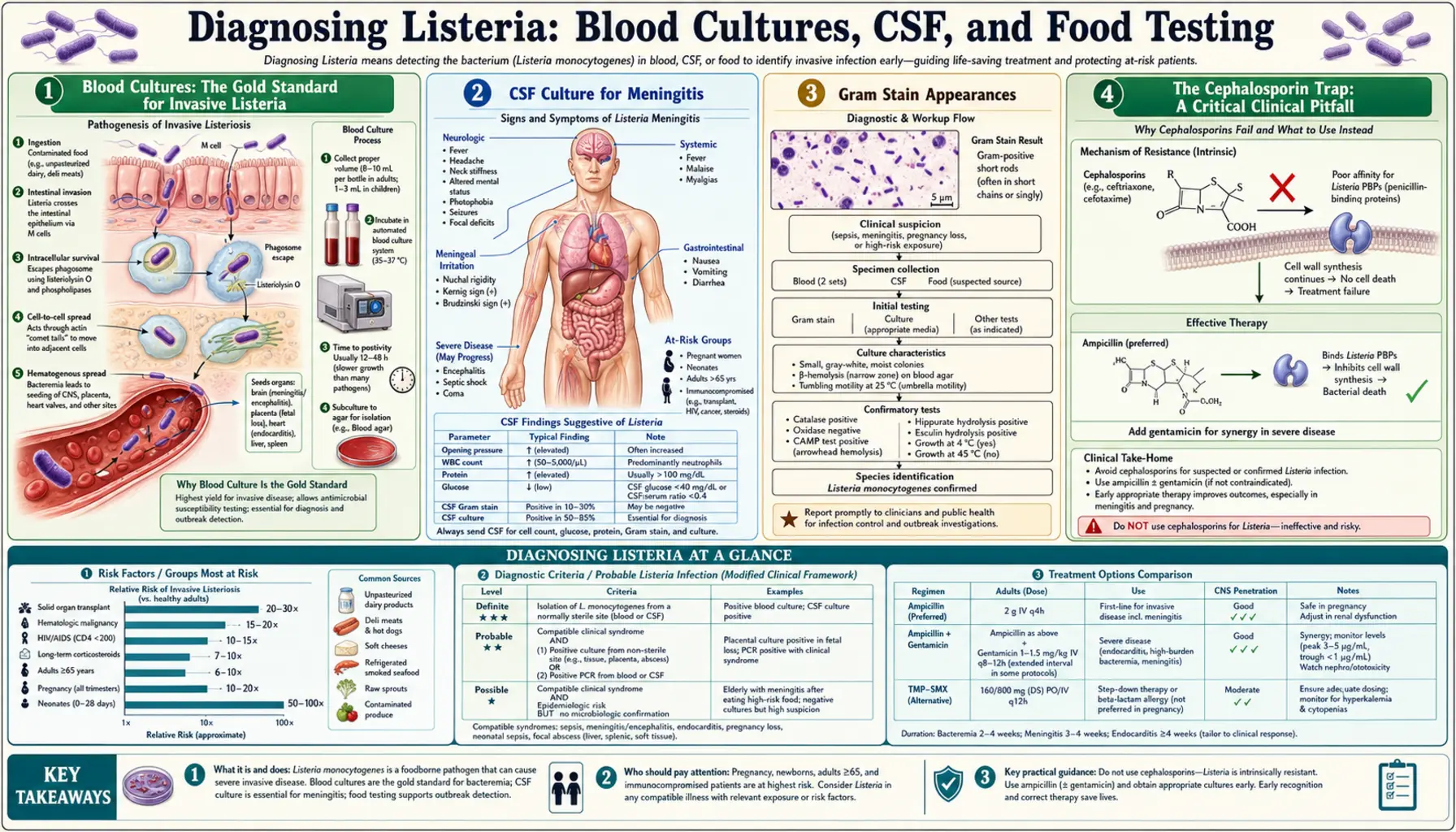
Blood Cultures: The Gold Standard for Invasive Listeria
Blood culture is the cornerstone of diagnosing invasive listeriosis. When Listeria monocytogenes is circulating in the bloodstream (bacteremia), blood culture bottles will become positive in typically 24–48 hours, making it one of the faster-growing bacteria in standard clinical microbiology.
How blood cultures work: Blood is drawn from a peripheral vein (not from an existing intravenous line, which can be colonised with other organisms) and injected into two types of culture bottles: an aerobic bottle (for oxygen-preferring organisms) and an anaerobic bottle (for oxygen-sensitive organisms). Listeria grows best in the aerobic bottle but will also grow in anaerobic conditions. Most modern automated blood culture systems (such as BACTEC and BacT/ALERT) monitor bottles continuously for CO2 production — a sign of bacterial metabolism — and alert the laboratory when a bottle flags positive.
Practical points for patients and families:
- Blood cultures should be drawn before any antibiotics are given. Antibiotics can suppress bacterial growth in culture bottles and delay or prevent a positive result — making diagnosis harder.
- Typically two to three sets of blood cultures are drawn from different sites within a short time window (30–60 minutes). Drawing multiple sets increases sensitivity; a single set may miss bacteremia if the bacterial count in blood is low.
- A positive blood culture does not require a very high bacterial load — modern automated systems can detect as few as 1–10 bacteria per millilitre of blood.
- If blood cultures are drawn after antibiotics have already been started (because the patient deteriorated quickly), they may still become positive — especially if antibiotics were started only recently — but sensitivity is reduced.
Once a blood culture bottle flags positive, the laboratory performs a Gram stain on the broth directly, which gives a preliminary result (gram-positive rods in the case of listeria) within an hour. Definitive species identification follows over the next 12–24 hours by subculture, biochemical testing, or mass spectrometry (MALDI-TOF). Antimicrobial susceptibility testing adds a further 18–24 hours.
CSF Culture for Meningitis
When a patient presents with signs of meningitis — severe headache, stiff neck, fever, and photophobia — the definitive diagnostic test is lumbar puncture (LP, also called a spinal tap), performed to collect cerebrospinal fluid (CSF) for culture, cell count, chemistry, and Gram stain.
The timing of LP matters clinically. Current infectious disease guidelines recommend that LP should not be delayed if meningitis is clinically suspected — it should be performed immediately, before antibiotics, if there are no contraindications (severe coagulopathy, signs of raised intracranial pressure with herniation risk). If a CT scan is required first (e.g., for papilledema, focal neurological signs, or immunosuppression), antibiotics should be started immediately while awaiting CT, because delaying antibiotics to wait for LP results significantly worsens outcomes in bacterial meningitis.
Typical CSF findings in listeria meningitis (see also the Invasive Listeriosis page for detail):
- Opening pressure: elevated, 20–40 cm H2O
- White blood cells: 100–1,000/µL — often with a mixed lymphocyte/neutrophil pattern that may initially suggest viral meningitis
- Protein: elevated, typically 100–500 mg/dL
- Glucose: low (<60% of simultaneous blood glucose)
- Gram stain: positive in only 30–40% of cases — a negative stain does not exclude listeria
CSF culture for Listeria typically turns positive within 24–48 hours on standard sheep blood agar. Because Listeria is an intracellular pathogen, it may be present in relatively low numbers in the CSF, which is why repeat LP is sometimes necessary if the first culture is negative but clinical suspicion remains high.
Gram Stain Appearances
On Gram stain, Listeria monocytogenes appears as gram-positive rods — short, slightly curved or cocco-bacillary rods (part-rod, part-coccoid shape) that stain blue-purple. They are often described as resembling streptococci in short chains or pairs, which sometimes leads to confusion.
The most dangerous and common misidentification is calling Listeria "diphtheroids" or "Corynebacterium species" — skin contaminants that are gram-positive rods and look microscopically similar. Laboratory staff who see gram-positive rods on a blood culture Gram stain from an elderly or immunocompromised patient sometimes dismiss the organism as a contaminant before the culture subculture grows. This is a potentially fatal error.
Clinical laboratories should flag any gram-positive rod grown from a blood culture of a high-risk patient as potentially listeria until proven otherwise, rather than assuming contamination. Several features help distinguish Listeria from diphtheroids in culture:
- Beta-haemolysis: Listeria produces narrow zones of beta-haemolysis on sheep blood agar (clearing around colonies from red blood cell lysis), whereas diphtheroids do not
- Tumbling motility: At room temperature, Listeria shows characteristic end-over-end tumbling motility on wet mount — a distinctive feature no Corynebacterium species displays
- Growth at 4°C: Listeria grows readily at refrigerator temperature — a selective culture step used for environmental food testing, though not routine for clinical specimens
- CAMP test: Listeria produces enhanced haemolysis when grown adjacent to Staphylococcus aureus (a positive CAMP reaction), helping differentiate it from other gram-positive rods
- MALDI-TOF mass spectrometry: Modern mass spectrometry systems (now standard in most clinical labs) identify Listeria from a colony within minutes with very high accuracy, resolving ambiguity rapidly
The critical action: when ordering a blood culture from a pregnant woman, elderly person, or immunocompromised patient, it is reasonable to add a note on the requisition: "Patient is immunocompromised — please ensure gram-positive rods are not dismissed as contaminants without speciation." This simple communication can accelerate correct identification.
The Cephalosporin Trap: A Critical Clinical Pitfall
This section addresses what is arguably the most important clinical fact about listeria diagnosis and treatment: the most commonly used empirical antibiotic regimen for bacterial meningitis in adults does not cover Listeria monocytogenes.
Standard empirical treatment for community-acquired bacterial meningitis in adults between ages 18 and 49 is typically ceftriaxone 2 g IV every 12 hours plus dexamethasone. Ceftriaxone is a third-generation cephalosporin with excellent activity against Streptococcus pneumoniae, Neisseria meningitidis, and many gram-negative organisms. However, Listeria monocytogenes is intrinsically resistant to all cephalosporins — every generation, from first-generation cefalexin through fourth-generation cefepime.
The mechanism of this intrinsic resistance is that Listeria possesses penicillin-binding proteins (PBPs) that have very low affinity for cephalosporins. The standard beta-lactam cell wall synthesis inhibition mediated by cephalosporins does not work against Listeria's PBP variants. There are no dosing tricks or concentration thresholds that make cephalosporins effective — they simply do not work.
This means:
- An elderly patient treated with ceftriaxone alone for bacterial meningitis is receiving no antibiotic coverage for listeria
- An immunocompromised patient treated with cefepime for febrile neutropenia with gram-positive bacteremia is not covered for listeria
- A pregnant woman given ceftriaxone for bacteremia is not covered for listeria
The solution is ampicillin. Listeria is highly susceptible to ampicillin (and to its oral form, amoxicillin). For meningitis, ampicillin 2 g IV every 4 hours is added to the ceftriaxone regimen whenever listeria is in the differential — which means any adult over 50, any immunocompromised patient, and any pregnant woman with suspected bacterial meningitis. Gentamicin is frequently added for synergy (ampicillin plus gentamicin kills listeria faster than either drug alone in vitro and in animal models).
The practical message: if you or a family member is immunocompromised and is being treated for meningitis or sepsis, it is entirely appropriate to ask the treating physician: "Does the antibiotic regimen cover Listeria? Is ampicillin included?"
NAAT and PCR for Listeria
Nucleic acid amplification tests (NAATs) — including conventional PCR and real-time PCR — can detect Listeria monocytogenes DNA in clinical specimens faster than culture. Where available, PCR for Listeria offers results in 2–4 hours versus 24–48 hours for culture.
Current applications and limitations:
- Blood PCR: Several commercial multiplex PCR panels for bloodstream infections (such as the BioFire FilmArray BCID2 panel) include Listeria monocytogenes. These can be run directly from a positive blood culture bottle within 1–2 hours, accelerating species identification compared to overnight subculture. However, they require a positive blood culture bottle to run — they do not replace the initial culture step.
- CSF PCR: The BioFire FilmArray Meningitis/Encephalitis (ME) panel includes Listeria monocytogenes and can detect it in CSF within about 1 hour. This is a significant advance — in a patient with meningitis, a positive CSF PCR for listeria can confirm the diagnosis within hours of LP, allowing rapid targeted therapy. The test is particularly valuable in patients who received antibiotics before LP (which may sterilise the culture but leaves DNA detectable).
- Sensitivity and specificity: The FilmArray ME panel has high sensitivity (approximately 92–100%) and specificity (approximately 99%) for Listeria in CSF, though listeria is rare enough that false positives, though uncommon, occur. Culture remains the reference standard for definitive confirmation and antimicrobial susceptibility testing.
- Availability: These panel tests are not universally available. Smaller hospitals and laboratories may not have access to rapid molecular testing. In those settings, empirical treatment decisions must be made on clinical grounds while cultures incubate.
PCR is also used in food testing (see below) and in environmental surveillance of food processing facilities, where it provides rapid screening for listeria contamination without the need to wait days for culture results.
Food Testing by Regulatory Agencies
When a foodborne listeria outbreak is suspected, regulatory agencies — primarily the FDA (for ready-to-eat foods, produce, and seafood) and the USDA Food Safety and Inspection Service (FSIS, for meat and poultry) — conduct environmental and product testing to confirm contamination and identify the source.
Standard culture method (BAM Method): The FDA Bacteriological Analytical Manual describes the standardised culture procedure for detecting Listeria in food. The method involves:
- A primary enrichment step: the food sample is mixed with enrichment broth (Listeria enrichment broth, LEB) and incubated at 30°C for 24–48 hours. Because Listeria is cold-tolerant, it can outcompete other organisms at temperatures that inhibit most competitors.
- A secondary selective enrichment: transfer to Fraser broth or PALCAM broth, which contain antibiotics that inhibit competing organisms while allowing Listeria to grow
- Selective agar plating: Oxford or PALCAM agar, which produces characteristic black halos around listeria colonies due to esculin hydrolysis
- Confirmation: biochemical testing, PCR, or MALDI-TOF of suspect colonies
Rapid screening methods including ELISA (enzyme-linked immunosorbent assay) for listeria antigens and real-time PCR are now routinely used for preliminary screening of large numbers of food and environmental samples. Positive screens are confirmed by culture. The PCR-based screening methods provide results in 24–48 hours versus the 5–7 days required for complete standard culture methods.
Environmental testing in food facilities focuses on "harborage sites" — cool, moist areas of food processing equipment where listeria can establish persistent biofilms: floor drains, condensation on cold surfaces, meat slicers, and packaging machines. Finding listeria in the environment does not automatically mean product is contaminated, but it triggers intensive cleaning, re-testing, and enhanced monitoring.
Whole-Genome Sequencing in Outbreak Investigation
Whole-genome sequencing (WGS) has transformed listeria outbreak investigation since its adoption by the CDC's PulseNet program in 2013. PulseNet is the national network that connects state and federal public health labs, allowing rapid sharing of bacterial genome sequences to identify clusters of related cases across the country.
Before WGS, outbreak investigation relied on pulsed-field gel electrophoresis (PFGE) — a DNA fingerprinting technique that could cluster listeria strains but lacked the resolution to distinguish closely related strains from unrelated ones. WGS provides a complete genetic "fingerprint" of each bacterial isolate, comparing thousands of genetic variants simultaneously.
How WGS identifies outbreak clusters:
- Every listeria isolate from a clinical case is sequenced by the state public health laboratory and uploaded to the National Center for Biotechnology Information (NCBI) database
- PulseNet algorithms compare all sequences in the database, flagging isolates that differ by only a few (typically 0–5) single nucleotide polymorphisms (SNPs) as potentially linked
- When multiple cases share nearly identical genome sequences, epidemiologists launch an investigation — interviewing patients, reviewing purchase records, and testing foods — to identify the shared source
- Environmental listeria isolates from food processing facilities are also sequenced and compared to clinical isolates, providing direct molecular evidence linking a food source to human illness
The power of WGS is in its precision. Before WGS, a 2011 outbreak traced to cantaloupe killed 33 people before the source was confirmed. Modern WGS-based surveillance can link cases within days, not weeks, and can also demonstrate that apparent "outbreaks" with genetically distinct strains represent multiple unrelated events rather than a single source — allowing public health resources to be correctly focused.
WGS has also revealed that some listeria strains persist in food processing environments for years, causing sporadic cases long after the initial environmental contamination was identified. The genetic stability of persistent strains means that a case in 2026 can sometimes be linked by WGS to a facility that had a positive environmental test in 2019.
Stool Culture: Limitations
Stool culture can detect Listeria monocytogenes, and the organism is found in the stool of both symptomatic and asymptomatic carriers — estimates suggest listeria is present in the stool of approximately 1–5% of healthy adults at any given time (asymptomatic carriage).
However, stool culture is not routinely used for the diagnosis of invasive listeriosis for several reasons:
- Asymptomatic carriage makes interpretation difficult: Finding listeria in stool does not confirm it is causing disease; many healthy people carry it intermittently
- Most clinical labs do not routinely culture for Listeria from stool: Standard stool culture panels in the US look for Salmonella, Shigella, Campylobacter, and E. coli O157:H7. Listeria must be specifically requested, and even then, the recovery techniques differ from blood and CSF (cold enrichment is used for food and environmental testing but not routine clinical stool culture)
- Invasive disease requires blood or CSF culture: In a patient with invasive listeriosis (bacteremia or meningitis), stool culture adds little — the diagnosis comes from blood or CSF. The stool result arrives days later and provides no additional management information.
- Outbreak use: Stool culture is useful in outbreak investigation when trying to identify cases of non-invasive febrile gastroenteritis — the mild form of listeriosis in healthy people. During an outbreak where multiple people ate the same food and developed diarrhoea/fever, stool culture from affected individuals can confirm listeria as the causative organism and help establish attack rates.
In summary: for suspected invasive listeriosis (bacteremia, meningitis) → blood culture and/or lumbar puncture. For outbreak investigation of gastroenteritis → stool culture requested specifically for Listeria. Stool culture should not be ordered as a substitute for blood culture in a patient with fever and immunocompromise.
When to Test Versus Empirically Treat
One of the most practical questions for patients in high-risk groups: if I'm immunocompromised and I ate deli meat two weeks ago and now I have a fever, do I need tests, or should I just start antibiotics?
The answer is: draw blood cultures first, then start antibiotics immediately. Do not do one without the other. Here is why:
- Starting antibiotics without cultures: If you take antibiotics first and then have blood drawn later, the cultures may be negative even if listeria was present. You lose the diagnostic information needed to confirm the diagnosis, guide the duration of therapy, and allow the health department to report a case (which contributes to outbreak detection). In an outbreak, every reported case matters for finding the contaminated food source before more people are harmed.
- Drawing cultures and then waiting for results before starting antibiotics: This is equally wrong. In invasive listeriosis, every hour without appropriate antibiotics increases the risk of progression to meningitis, cerebral involvement, or fetal death in pregnant women. Blood cultures take minutes to draw. Antibiotics should start immediately after the cultures are collected.
Specific clinical triggers for blood cultures plus empirical ampicillin:
- Pregnant woman with fever (at or above 38°C) who ate high-risk foods in the past 70 days
- Immunocompromised adult (transplant, cancer, biologic therapy) with fever and no obvious source
- Elderly patient with fever, myalgia, and any suggestion of CNS symptoms (headache, confusion)
- Any adult with fever and neck stiffness: lumbar puncture plus blood cultures, start ampicillin immediately
- Anyone specifically notified of consuming a food subject to listeria recall who develops fever
For the immunocompromised patient who is afebrile but known to have eaten a recalled product: monitoring is appropriate (temperature twice daily, report any symptoms immediately), but prophylactic antibiotics in asymptomatic adults are not standard of care. The decision should be made case-by-case with a treating physician considering the degree of immunosuppression and the certainty of exposure.
Connections
- All Bacteria
- Listeria Symptoms Overview
- Invasive Listeriosis and Meningitis
- Listeria in Pregnancy and Newborns
- Listeria Treatment and Prevention
- Ampicillin and Antibiotic Treatment
- Outbreak Investigation
- Meningitis
- Lab Tests
- Blood Culture — the test that confirms invasive listeriosis, and how bottles, timing, and prior antibiotics change the result.
Key Research Papers
- Brouwer MC et al. Epidemiology, diagnosis, and antimicrobial treatment of acute bacterial meningitis. Clin Microbiol Rev. 2010;23(3):467–492. PMID 20610819
- Eckburg PB et al. Listeria monocytogenes meningitis: a clinical review. Clin Infect Dis. 1999;29(4):745–751. — Search PubMed
- Pohl AM et al. Evaluation of a multiplex PCR assay for the identification of Listeria species in clinical samples. J Clin Microbiol. 2013;51(3):921–924. — Search PubMed
- Leclercq A et al. Recognition of a commonly misidentified pathogen: Listeria monocytogenes. Clin Microbiol Infect. 2010;16(3):306–308. — Search PubMed
- Swaminathan B, Gerner-Smidt P. The epidemiology of human listeriosis. Microbes Infect. 2007;9(10):1236–1243. PMID 17720602
- Jackson BR et al. Implementation of nationwide real-time whole-genome sequencing to enhance listeriosis outbreak detection and investigation. Clin Infect Dis. 2016;63(3):380–386. PMID 27090985
- Doumith M et al. Differentiation of the major Listeria monocytogenes serovars by multiplex PCR. J Clin Microbiol. 2004;42(8):3819–3822. PMID 15297538
- Erickson MC, Doyle MP. The challenges of eliminating or substituting antimicrobial compounds in food preservation. Annu Rev Food Sci Technol. 2012;3:387–415. — Search PubMed
- Farber JM, Peterkin PI. Listeria monocytogenes, a food-borne pathogen. Microbiol Rev. 1991;55(3):476–511. PMID 1943998
- Vallejo AN et al. Listeria monocytogenes detection in clinical specimens: a comparison of culture and real-time PCR methods. J Med Microbiol. 2012;61(Pt 12):1752–1756. — Search PubMed
- Chen Y et al. Whole-genome sequencing for investigations of Listeria monocytogenes outbreaks in the United States. J Clin Microbiol. 2016;54(4):863–873. — Search PubMed