Invasive Listeriosis: Bacteremia, Meningitis, and Encephalitis
- Bacteremia: Bacteria in the Bloodstream
- Listeria Meningitis
- CSF Findings in Listeria Meningitis
- Rhombencephalitis: Brainstem Infection
- Brain Abscess from Listeria
- Mortality from CNS Listeriosis
- Transplant and Cancer Patients at Extreme Risk
- Recovery and Neurological Sequelae
- Connections
Bacteremia: Bacteria in the Bloodstream
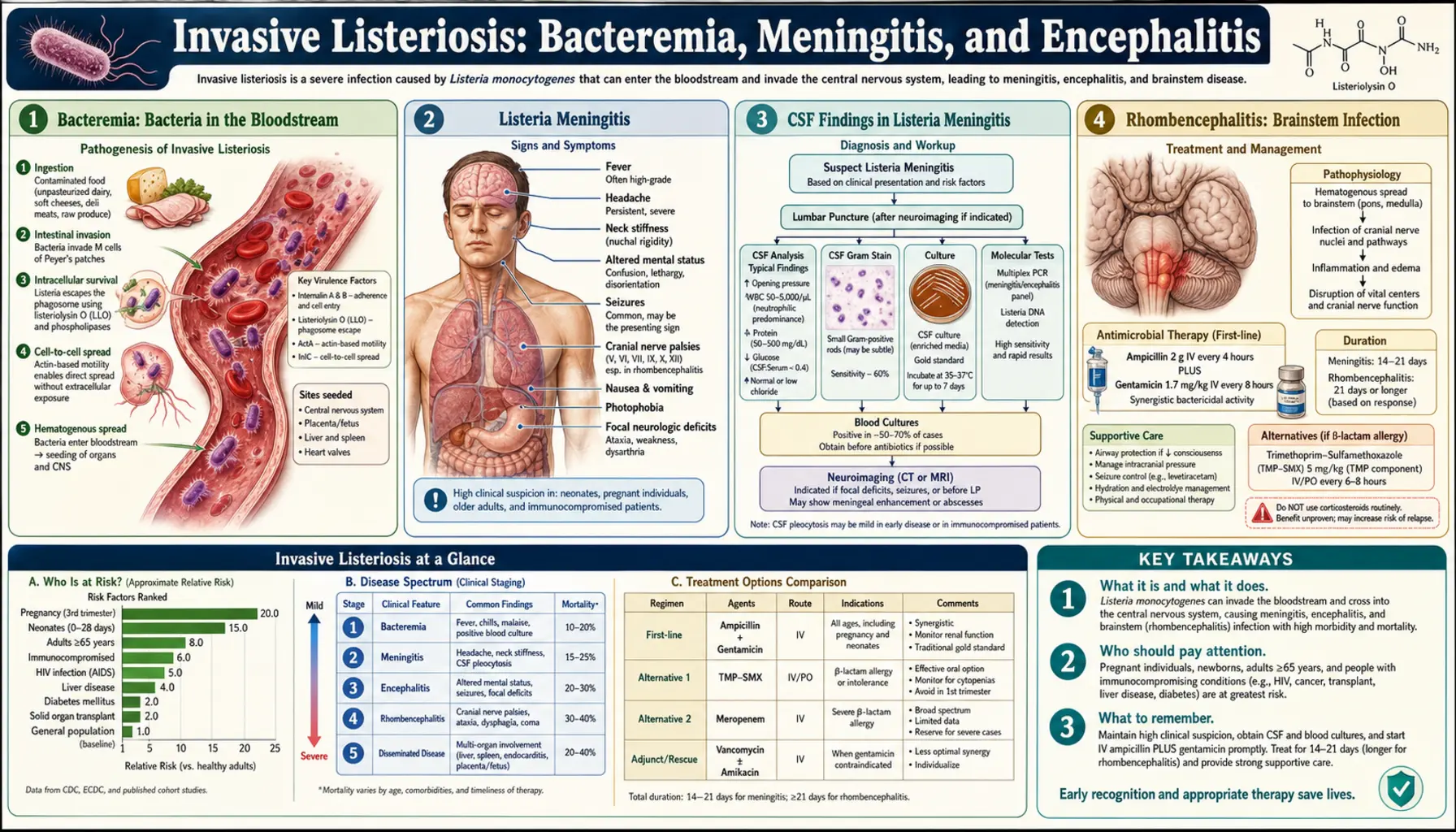
Bacteremia — bacteria circulating freely in the blood — is the most common form of invasive listeriosis in non-pregnant adults. It accounts for roughly 70% of all invasive cases. The path from gut to bloodstream follows a specific biological route that distinguishes Listeria from most other foodborne pathogens.
After being ingested, Listeria monocytogenes survives stomach acid and reaches the small intestine, where it invades enterocytes (gut lining cells) and dendritic cells using surface proteins called internalins — particularly InlA and InlB. Once inside a cell, the bacterium escapes from the phagosome (the vesicle meant to destroy it) using a toxin called listeriolysin O (LLO). It then hijacks the host cell's actin filaments to propel itself through the cytoplasm and into adjacent cells, spreading without ever being exposed to antibodies or complement in the bloodstream. This actin rocket mechanism is one of the most elegant and dangerous bacterial strategies in infectious disease.
In a healthy person, intestinal macrophages and dendritic cells capture and destroy the bacteria. In immunocompromised people, the bacteria spread to regional lymph nodes and then reach the liver and spleen via portal circulation. From there, they spill into the systemic bloodstream.
Symptoms of listeria bacteremia are non-specific: high fever (often 38.5–40°C), chills, severe muscle aches, headache, and fatigue. Nausea, vomiting, or mild diarrhoea may be present but are not always. Many patients describe it as "the worst flu of my life." Without blood cultures, listeria bacteremia is indistinguishable from dozens of other infections or even from drug reactions in immunocompromised patients on complex medication regimens.
Listeria Meningitis
Listeria monocytogenes is the third most common cause of bacterial meningitis in adults (after Streptococcus pneumoniae and Neisseria meningitidis) and the most common cause in adults over 50, people receiving immunosuppressive therapy, and transplant recipients. Among all cases of adult bacterial meningitis requiring intensive care, listeria accounts for approximately 10–15%.
The bacteria reach the meninges (the membranes covering the brain and spinal cord) via the bloodstream after bacteremia. The choroid plexus — the structure inside the brain that produces cerebrospinal fluid (CSF) — appears to be a key entry point. Listerial meningitis causes inflammation of the meninges with the same cardinal signs as any bacterial meningitis.
Classic symptoms include:
- Severe headache — typically described as the worst headache of the patient's life, often bifrontal or generalised
- Neck stiffness (meningismus) — inability to flex the neck forward to the chest, caused by inflammation of the meningeal membranes
- Photophobia — severe sensitivity to light; even ordinary indoor light is painful
- High fever — usually above 38.5°C, often with rigors
- Altered mental status — confusion, lethargy, or agitation in more severe cases
- Nausea and vomiting
One important difference from meningococcal meningitis: the rash (petechiae, purpura) that is a hallmark of meningococcal disease does not occur in listeria meningitis. The absence of rash in a person with meningismus does not rule out bacterial meningitis — listeria meningitis presents without rash in virtually all cases.
CSF Findings in Listeria Meningitis
When a lumbar puncture (spinal tap) is performed in suspected bacterial meningitis, the cerebrospinal fluid findings can sometimes suggest Listeria as the causative organism — though the definitive answer always comes from culture.
Typical CSF findings in listeria meningitis:
- Opening pressure: Elevated, usually 20–40 cm H2O (normal is under 20)
- White blood cell (WBC) count: Often surprisingly modest — 100–1,000 cells/µL — lower than many other causes of bacterial meningitis, which typically show 1,000–10,000+ cells. This is the most distinctive feature.
- Cell differential: Mixed — often 30–70% lymphocytes alongside neutrophils. Most bacterial meningitis is predominantly neutrophilic; listeria can look more like viral (aseptic) meningitis on initial differential, which can mislead clinicians away from empirical antibiotic coverage.
- Glucose: Low (less than 60% of simultaneous blood glucose), reflecting bacterial consumption — similar to other bacterial meningitis
- Protein: Elevated, typically 100–500 mg/dL
- Gram stain: Positive in only about 30–40% of listeria meningitis cases — far lower than pneumococcal (80%+) or meningococcal meningitis. This means a negative Gram stain does not rule out bacterial meningitis caused by listeria.
The relatively mild CSF pleocytosis and mixed cellular picture of listeria meningitis means it is sometimes initially treated as viral (aseptic) meningitis — a dangerous error. Clinicians must consider CSF culture mandatory and must ensure empirical antibiotic coverage includes ampicillin (which covers Listeria) in any adult over 50 or any immunocompromised patient with meningitis, even before CSF results return.
Rhombencephalitis: Brainstem Infection
Rhombencephalitis — inflammation of the rhombencephalon, which is the brainstem and cerebellum — is a distinctive and particularly dangerous form of listeria infection. It occurs in about 10–15% of CNS listeriosis cases and may occur even in otherwise healthy adults, without the typical high-risk group membership seen with other forms of invasive disease.
Unlike listerial meningitis, rhombencephalitis is a direct infection of the brainstem parenchyma (tissue). The bacterium appears to reach the brainstem via cranial nerve axons — travelling from the mouth or nasopharynx along the trigeminal or vagal nerves directly to the medulla and pons, bypassing the blood-brain barrier entirely. This neural route of spread is unusual and explains why some patients with rhombencephalitis have no bacteremia and normal or only mildly abnormal CSF.
The clinical presentation of rhombencephalitis is distinctive and should be recognised immediately:
- Prodrome: Fever, headache, nausea for 3–5 days before neurological signs appear
- Cranial nerve palsies: Facial palsy (CN VII), difficulty swallowing (CN IX, X), double vision (CN VI), asymmetric hearing loss (CN VIII)
- Cerebellar signs: Ataxia (unsteady gait), dysmetria (reaching past targets), nystagmus
- Respiratory failure: Occurs when infection spreads to the respiratory centres in the medulla — a catastrophic complication requiring mechanical ventilation
- Altered consciousness: Progressing to coma in severe cases
MRI of the brain is essential when rhombencephalitis is suspected. It typically shows T2 signal abnormality in the brainstem — pons, medulla, or cerebellum — with variable ring enhancement on gadolinium sequences. CSF may be normal or show only mild changes, which can falsely reassure physicians that bacterial meningitis is not present.
Mortality from rhombencephalitis is approximately 30–50%, and survivors often have significant residual neurological deficits including cranial nerve palsies, ataxia, and cognitive changes.
Brain Abscess from Listeria
Brain abscesses caused by Listeria monocytogenes are rare — accounting for about 10% of CNS listeriosis — but represent one of the most difficult management challenges in infectious disease. They occur almost exclusively in immunocompromised patients: solid organ transplant recipients, patients on prolonged corticosteroid therapy, and people with haematologic malignancies.
Listerial brain abscesses have a predilection for the brainstem (particularly the pons and medulla) and the thalamus, distinguishing them from most other bacterial brain abscesses which typically occur in the cerebral hemispheres. This distribution reflects the same neural route of spread seen in rhombencephalitis.
Symptoms develop subacutely over days to weeks: headache, fever, focal neurological signs corresponding to the abscess location (limb weakness, cranial nerve palsy, gait disturbance), and eventually altered consciousness. MRI reveals ring-enhancing lesions with surrounding oedema.
Treatment requires prolonged antibiotic therapy — typically 6–8 weeks of intravenous ampicillin, often combined with gentamicin for the first 2 weeks. Surgical drainage, which is standard for most brain abscesses, is technically difficult and often not feasible for brainstem abscesses. Prognosis is poor: mortality approaches 40–50%, and survivors almost uniformly have permanent neurological deficits.
One important practical note: the antifungal drug fluconazole, which transplant patients commonly receive for fungal prophylaxis, and the bacteriostatic antibiotic trimethoprim-sulfamethoxazole (co-trimoxazole), which provides incidental listeria prophylaxis in HIV patients, have dramatically different effects — co-trimoxazole prevents listeria infections in HIV patients effectively, while patients on fluconazole prophylaxis alone remain fully susceptible.
Mortality from CNS Listeriosis
The case fatality rate for CNS listeriosis (meningitis, encephalitis, rhombencephalitis, and brain abscess combined) is approximately 25–35%, even when patients receive appropriate intravenous antibiotics in intensive care. This is substantially higher than the mortality of CNS infection caused by Streptococcus pneumoniae (~20–25% in adults) and far higher than Neisseria meningitidis (~5–10%).
Several factors drive this high mortality:
- Patient vulnerability: Most patients with CNS listeriosis are already medically compromised. Their co-morbidities — transplant rejection risk, haematologic malignancies, end-stage renal disease — compound the mortality from the infection itself.
- Diagnostic delay: The atypical CSF picture (mixed pleocytosis, may look viral) frequently delays appropriate antibiotic coverage. Every additional hour before ampicillin is started increases mortality in bacterial meningitis.
- The cephalosporin gap: Cephalosporins — the most commonly used empirical treatment for community-acquired bacterial meningitis — have no activity against Listeria. Patients treated with ceftriaxone alone are inadequately covered.
- Location of infection: Brainstem involvement (rhombencephalitis, brainstem abscess) is inherently more deadly than cortical involvement because the brainstem controls breathing and cardiovascular function.
Survivors of CNS listeriosis have significant morbidity. Studies show approximately 30–40% of survivors have persistent neurological deficits at 1 year, including cognitive impairment, hearing loss, focal weakness, and movement disorders.
Transplant and Cancer Patients at Extreme Risk
Solid organ transplant recipients represent the highest-risk group for invasive listeriosis outside of pregnancy. Studies of transplant populations show listeriosis incidence 100–1,000 times higher than the general population.
The specific immunosuppressive agents used post-transplant explain the extreme susceptibility:
- Calcineurin inhibitors (tacrolimus, cyclosporine) block T-cell activation — the precise arm of immunity needed to control intracellular pathogens like Listeria. Tacrolimus in particular profoundly impairs cell-mediated immunity at the doses used for rejection prevention.
- High-dose corticosteroids used for rejection episodes further suppress macrophage function and neutrophil killing.
- Mycophenolate mofetil reduces lymphocyte proliferation, compounding the T-cell deficit.
Kidney transplant recipients on tacrolimus-based regimens have the highest risk among solid organ recipients — rates approximately 150 times the general population. Heart and liver transplant recipients are similarly vulnerable.
For haematology patients, the risk peaks during active chemotherapy for lymphoma, leukaemia, and myeloma — particularly during periods of profound lymphopenia. The combination of lymphopenia plus corticosteroids (used in many chemotherapy regimens like RCHOP, CHOP) creates ideal conditions for listeria dissemination.
Trimethoprim-sulfamethoxazole (TMP-SMX), which many transplant and haematology patients receive for Pneumocystis jirovecii prophylaxis, provides effective co-prophylaxis against listeria — but TMP-SMX-allergic patients or those on alternative prophylaxis are unprotected. This is why dietary counselling about listeria-risk foods is particularly important for transplant recipients.
Recovery and Neurological Sequelae
For patients who survive CNS listeriosis, the recovery trajectory depends heavily on the form of infection and the extent of neurological injury at the time treatment began.
After listeria meningitis (without brainstem or parenchymal involvement), recovery can be relatively good if treatment was started early. However, significant sequelae occur in 30–50% of survivors:
- Sensorineural hearing loss: The most common sequela, occurring in approximately 25% of adult listeria meningitis survivors. It results from cochlear hair cell damage during the inflammatory phase. Hearing should be formally tested after discharge from all meningitis survivors.
- Cognitive impairment: Difficulties with memory, concentration, and processing speed are common and may not be apparent until the patient returns to work or school months later.
- Vestibular dysfunction: Balance problems, dizziness, and difficulty walking on uneven surfaces — related to both inner ear damage and cerebellar injury.
- Focal neurological deficits: Weakness, sensory loss, or visual field cuts in cases where cortical infarction occurred during the infectious phase.
After rhombencephalitis or brainstem abscess, residual deficits are present in the majority of survivors: cranial nerve palsies (facial droop, swallowing difficulty, hoarseness), cerebellar signs (ataxia, dysmetria), and cognitive changes. Some patients require percutaneous feeding tubes long-term due to dysphagia.
Rehabilitation after CNS listeriosis typically involves multidisciplinary input: speech and language therapy (swallowing), physiotherapy (gait and balance), occupational therapy (activities of daily living), and audiological assessment. Full recovery to pre-illness neurological function occurs in perhaps 30–40% of non-brainstem meningitis survivors but is rare after brainstem involvement.
Connections
- Listeria Symptoms Overview
- Listeria in Pregnancy and Newborns
- Diagnosis: Blood, CSF, and Testing
- Listeria Treatment and Prevention
- Ampicillin and Antibiotic Treatment
- All Bacteria
- Meningitis
- Encephalitis
Key Research Papers
- Brouwer MC et al. Epidemiology, diagnosis, and antimicrobial treatment of acute bacterial meningitis. Clin Microbiol Rev. 2010;23(3):467–492. PMID 20610819
- Thigpen MC et al. Bacterial meningitis in the United States, 1998–2007. N Engl J Med. 2011;364(21):2016–2025. PMID 21612470
- Bortolussi R. Listeriosis: a primer. CMAJ. 2008;179(8):795–797. — Search PubMed
- Antal EA et al. Listeria monocytogenes and the central nervous system. J Infect. 2005;50(2):120–126. — Search PubMed
- Mylonakis E et al. Central nervous system infection with Listeria monocytogenes. Medicine (Baltimore). 1998;77(5):313–336. PMID 9772921
- Arslan F et al. Risk and outcome of listeriosis in patients with underlying immunosuppressive conditions in a tertiary hospital. Neth J Med. 2015;73(5):233–239. — Search PubMed
- Disson O, Lecuit M. Targeting of the central nervous system by Listeria monocytogenes. Virulence. 2012;3(2):213–221. — Search PubMed
- Pamer EG. Immune responses to Listeria monocytogenes. Nat Rev Immunol. 2004;4(10):812–823. PMID 15459672
- Schuchat A et al. Listeriosis in humans. In: Ryser ET, Marth EH, eds. Listeria, Listeriosis and Food Safety. New York: Marcel Dekker; 1999. — comprehensive clinical review.
- Cabellos C et al. Listeria monocytogenes meningitis and encephalitis. Medicine (Baltimore). 2015;94(42):e1743. — Search PubMed
- Claes N et al. Organ transplantation and the risk of listeriosis: a systematic review. Transplant Infect Dis. 2018;20(3):e12906. — Search PubMed
- van de Beek D et al. Adjunctive dexamethasone in bacterial meningitis: a meta-analysis of individual patient data. Lancet Neurol. 2010;9(3):254–263. — Search PubMed