Listeria Treatment: Ampicillin, Gentamicin, and Alternatives
- Ampicillin Mechanism Against Listeria
- Ampicillin IV Dosing
- Gentamicin Synergy
- The Cephalosporin Failure
- TMP-SMX for Penicillin Allergy
- Meropenem as Alternative
- Treatment Duration by Infection Site
- Neonatal Dosing
- Monitoring Treatment Response
- Key Research Papers
- Connections
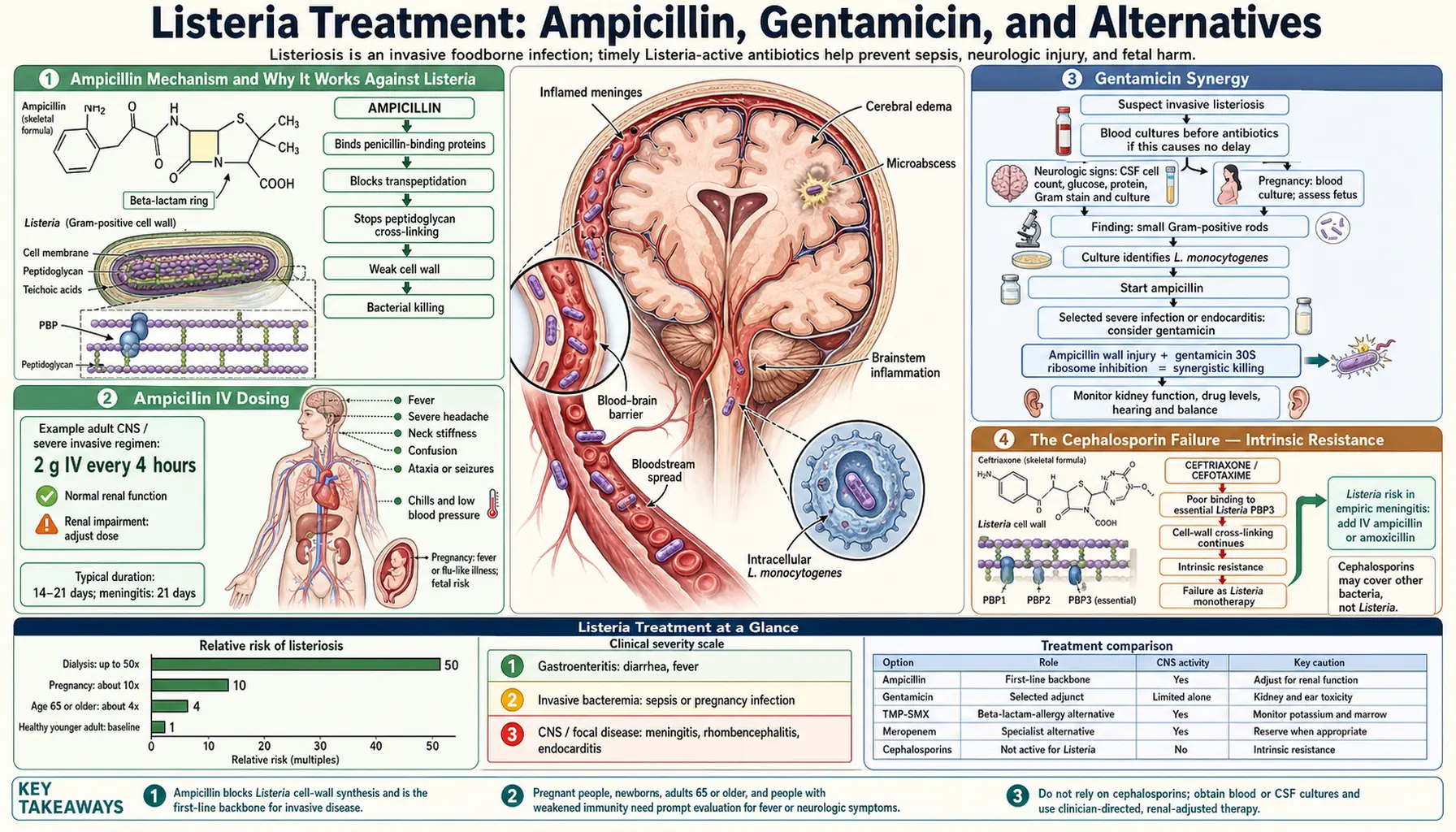
Ampicillin Mechanism and Why It Works Against Listeria
Ampicillin belongs to the aminopenicillin class of beta-lactam antibiotics. It kills bacteria by binding to penicillin-binding proteins (PBPs) — enzymes that bacteria use to build and cross-link their cell wall. Specifically, ampicillin has strong affinity for PBP3 in Listeria monocytogenes, the key enzyme responsible for forming the bacterial cell wall's structural peptidoglycan mesh.
When ampicillin binds PBP3, the cell wall develops defects. The bacterium continues to grow but cannot maintain wall integrity, eventually rupturing from its own internal pressure. This makes ampicillin bactericidal — it does not merely inhibit Listeria but actively kills it, which is essential for clearing infection from immune-privileged sites like the brain and placenta.
Two additional properties make ampicillin ideal for Listeria treatment: it penetrates the blood-brain barrier when the meninges are inflamed (achieving bactericidal concentrations in cerebrospinal fluid), and it crosses the placenta, reaching the fetus and directly treating infection in the amniotic fluid and fetal tissues. No other first-line Listeria antibiotic matches this combination of properties.
Ampicillin IV Dosing
Ampicillin for listeriosis is always given intravenously — oral absorption is insufficient for blood and brain infections. The dose depends on which part of the body is infected:
- Meningitis and CNS infection: 2 g IV every 4 hours (total daily dose: 12 g/day). The higher frequency and dose is needed because the blood-brain barrier limits how much drug penetrates, even when inflamed. Brain tissue requires higher serum levels to drive enough drug across.
- Bacteremia without CNS involvement: 2 g IV every 6 hours (total daily dose: 8 g/day). Lower dose is effective when the drug does not need to penetrate a biological barrier.
- Endocarditis: 2 g IV every 4–6 hours for 4–6 weeks, combined with gentamicin throughout.
- Pregnancy-associated bacteremia: 2 g IV every 6 hours; if CNS or fetal involvement is suspected, the 4-hour dosing interval is preferred.
Ampicillin is generally well-tolerated. Side effects include rash (common, usually not allergic), diarrhea, and rarely hypersensitivity reactions including anaphylaxis. Patients with a history of severe penicillin reactions require an alternative — see TMP-SMX below.
Gentamicin Synergy
Gentamicin is an aminoglycoside antibiotic that kills bacteria by penetrating the cell and binding the 30S ribosomal subunit, causing misreading of messenger RNA and production of faulty, toxic proteins. On its own against Listeria, gentamicin is not highly effective because the bacteria's intact cell wall limits aminoglycoside entry. But when combined with ampicillin — which disrupts that cell wall — gentamicin gains much better access to the bacterial interior.
This synergy is not just theoretical. In vitro studies and clinical series show that ampicillin plus gentamicin kills Listeria faster and more completely than ampicillin alone. The combination is considered standard of care for severe disease: meningitis, endocarditis, neonatal listeriosis, and bacteremia in highly immunocompromised patients.
Gentamicin dosing: Traditional dosing is 1.5 mg/kg IV every 8 hours. Extended-interval (once-daily) dosing at 5–7 mg/kg/day is used in some centers based on PK/PD data, though traditional dosing remains more common for CNS infections. Regardless of schedule, renal monitoring is mandatory — aminoglycosides accumulate in kidney tubule cells and can cause permanent hearing loss (ototoxicity) and kidney injury, especially with prolonged use. Serum creatinine and drug trough levels are checked regularly throughout the course.
Gentamicin is typically continued for the first 7–14 days of therapy, then discontinued while ampicillin continues for the full treatment duration.
The Cephalosporin Failure — Intrinsic Resistance
This is the most dangerous gap in standard infectious disease management: Listeria monocytogenes is intrinsically resistant to all cephalosporin antibiotics, including the most potent third-generation agents like ceftriaxone, cefotaxime, and ceftazidime, as well as fourth-generation cefepime and fifth-generation ceftaroline.
The reason is PBP selectivity. Listeria's penicillin-binding proteins have very low affinity for cephalosporins — the drugs simply do not bind well enough to inhibit cell wall synthesis at achievable clinical concentrations. Unlike resistance acquired through genetic mutations (as with MRSA), this resistance is built into Listeria's molecular machinery and is universal across all strains ever tested.
The clinical problem: Ceftriaxone is the standard empiric antibiotic for bacterial meningitis in adults — it covers pneumococcus and meningococcus extremely well. If a clinician treats suspected meningitis with ceftriaxone alone and the patient turns out to have Listeria, the bacteria experience essentially zero antibiotic pressure. By the time the error is recognized (when cultures grow at 24–48 hours and show an organism resistant to what was given), the patient has lost critical hours.
This is why every bacterial meningitis guideline specifies that patients over 50, pregnant women, and immunocompromised patients should receive ampicillin added to the ceftriaxone regimen empirically. The cost of the extra drug is trivial; the cost of missing Listeria is not.
TMP-SMX for Penicillin Allergy
Trimethoprim-sulfamethoxazole (TMP-SMX, brand name Bactrim or Septra) is the standard alternative when a patient cannot receive ampicillin due to confirmed penicillin allergy. It is the only alternative with robust clinical evidence showing outcomes comparable to ampicillin-based regimens.
Mechanism: TMP-SMX acts by sequential blockade of the folate synthesis pathway. Trimethoprim inhibits dihydrofolate reductase; sulfamethoxazole inhibits dihydropteroate synthase. Together they starve the bacteria of the folate required for DNA synthesis. This is a completely different mechanism from beta-lactams, with no cross-resistance.
Dosing for invasive listeriosis: 15–20 mg/kg/day of the TMP component, given IV in 3–4 divided doses. For a typical 70 kg adult, this is 280–400 mg of TMP per day (approximately 1600–2400 mg of the SMX component). The 1:5 TMP:SMX ratio means commonly used tablets (160/800 mg) are useful for step-down therapy when the patient can take oral medications and infection is controlled, though IV-only treatment is the norm for serious disease.
Side effects to monitor: Kidney injury (especially in patients already on other nephrotoxins), hyperkalemia (TMP blocks renal potassium excretion — dangerous in patients on ACE inhibitors or with kidney disease), bone marrow suppression (monitor CBC), and skin rashes including rare but severe Stevens-Johnson syndrome. Drug-drug interactions with warfarin (TMP-SMX dramatically raises INR) and methotrexate are important in immunocompromised patients who may be on these drugs.
Meropenem as Alternative
Meropenem, a carbapenem antibiotic, has activity against Listeria monocytogenes and is occasionally used as an alternative in patients who cannot receive either ampicillin or TMP-SMX. Like ampicillin, it targets penicillin-binding proteins, but its broader spectrum covers many other organisms simultaneously.
The evidence base for meropenem in listeriosis is much thinner than for ampicillin or TMP-SMX — it appears primarily in case reports and small series. The main clinical scenario where it is considered is the critically ill patient with multiple possible diagnoses being covered empirically (severe healthcare-associated infection or immunocompromised patient with an uncertain picture), where the broad-spectrum coverage of carbapenem makes sense for the overall picture rather than for Listeria specifically.
Standard dosing for CNS infection is 2 g IV every 8 hours, with extended infusion (over 3 hours) used in some centers to optimize pharmacodynamic target attainment. Meropenem penetrates the CSF reasonably well during meningitis. It is not recommended as first choice for Listeria because clinical experience is limited and ampicillin with its decades of proven efficacy remains clearly superior.
Treatment Duration by Infection Site
The duration of antibiotic treatment is determined by where the infection has established itself. The guiding principle is that immunologically privileged sites — the central nervous system, the heart valves, and the fetal compartment — are harder to clear and require longer treatment:
- Bacteremia (blood infection), no focal involvement: 14 days total. This is the minimum acceptable course. Even in patients who feel well after a week of treatment, stopping early risks relapse from bacteria that have not been fully cleared from the blood.
- Meningitis: 21 days minimum. The blood-brain barrier limits antibiotic penetration and allows bacterial sanctuaries. Three weeks of full-dose IV ampicillin is standard, with gentamicin typically for the first 7–14 days.
- Meningoencephalitis (brain tissue involvement beyond meninges): 21 days at minimum; some experts extend to 28 days or longer based on clinical response and repeat imaging.
- Brain abscess: 6 weeks or more, sometimes with neurosurgical drainage in addition to antibiotics. Abscesses are the most difficult to eradicate — bacteria in the abscess wall are metabolically less active and less susceptible to antibiotics.
- Endocarditis: 4–6 weeks with gentamicin synergy maintained throughout — not just the first 2 weeks as in meningitis. Listeria endocarditis carries mortality above 40% and may require surgery for valve replacement.
- Rhombencephalitis (brainstem involvement): Minimum 6 weeks given the high relapse risk and poor CSF penetration to the posterior fossa.
Neonatal Dosing
Newborns with listeriosis — whether acquired in utero (early-onset, presenting in the first 7 days of life) or through the birth canal or nursery (late-onset, presenting at 7–30 days) — require both ampicillin and gentamicin. The principle of synergy applies as strongly to neonates as adults, but dosing is based on weight and postnatal age, not fixed adult doses.
Ampicillin for neonates: 50 mg/kg per dose; frequency depends on age: every 12 hours in the first week of life (immature kidney clearance), every 8 hours from days 7–21, and every 6 hours after 3 weeks. For meningitis, doses are increased to 75–100 mg/kg per dose on the same schedules.
Gentamicin for neonates: Standard dosing is 2.5 mg/kg every 12–24 hours depending on gestational and postnatal age. Premature infants require longer dosing intervals due to immature renal function. Therapeutic drug monitoring (trough and peak levels) is essential to balance efficacy against nephrotoxicity and ototoxicity, which are particularly concerning in developing newborn organ systems.
Treatment duration for neonatal listeriosis: 10–14 days for bacteremia; 14–21 days for meningitis. Neonatal meningitis carries a significant risk of long-term neurological sequelae including hydrocephalus, hearing loss, and developmental delay — close follow-up after treatment completion is critical.
Monitoring Treatment Response
The first sign of improvement in listeriosis is usually fever resolution — typically within 48–72 hours of starting appropriate antibiotics. Persistent fever beyond 96 hours on ampicillin should prompt reassessment: Is the dose correct? Has the organism been confirmed susceptible? Is there a sequestered infection (abscess, endocarditis) that is not being controlled with antibiotics alone?
Follow-up blood cultures are standard 48–72 hours after starting treatment to confirm bacteremia has cleared. Persistent positive blood cultures indicate either antibiotic failure, undrained source (infected line, abscess), or inadequate dosing.
Repeat lumbar puncture is generally performed 48–72 hours into treatment for meningitis to confirm CSF is responding — decreasing white cell count, decreasing protein, and ideally sterile culture. Persistent growth on repeat CSF culture at 48–72 hours is a clinical emergency requiring neurosurgical consultation to rule out abscess.
Renal function and gentamicin levels are checked every 2–3 days throughout the course. Creatinine rising more than 0.3 mg/dL above baseline warrants dose interval extension or discontinuation of gentamicin with infectious disease guidance. In patients who have recovered to the point where oral step-down is being considered, TMP-SMX can be used for the remainder of the course, though most experts prefer to complete the full course IV for CNS disease.
Key Research Papers
- Tunkel AR, et al. Practice guidelines for the management of bacterial meningitis. Clin Infect Dis. 2004;39(9):1267–1284. PMID: 15494903
- Hof H. An update on the medical management of listeriosis. Expert Opin Pharmacother. 2004;5(8):1727–1735. PMID: 15264991
- Lorber B. Listeriosis. Clin Infect Dis. 1997;24(1):1–11 — Search PubMed
- Merle-Melet M, et al. Is amoxicillin-cotrimoxazole the most appropriate antibiotic regimen for listeria meningoencephalitis? Retrospective analysis of 22 cases and review of the literature. J Infect. 1996;33(2):79–85 — Search PubMed
- Clauss HE, Lorber B. Central nervous system infection with Listeria monocytogenes. Curr Infect Dis Rep. 2008;10(4):300–306 — Search PubMed
- Mylonakis E, et al. Listeria monocytogenes — an emerging food-borne pathogen. Eur J Clin Microbiol Infect Dis. 1998;17(7):462–468 — Search PubMed
- Wing EJ, Gregory SH. Listeria monocytogenes: clinical and experimental update. J Infect Dis. 2002;185(Suppl 1):S18–S24 — Search PubMed
- Thønnings S, et al. Antibiotic treatment and mortality in patients with Listeria monocytogenes meningitis or bacteraemia. Clin Microbiol Infect. 2016;22(8):725–730 — Search PubMed
- Lamont RF, et al. Listeriosis in human pregnancy: a systematic review. J Perinat Med. 2011;39(3):227–236 — Search PubMed
- Safdar A, et al. Listeria monocytogenes bacteremia in adults: analysis of 55 cases at the University of California, San Francisco, from 1990 to 1999. Clin Infect Dis. 2002;34(5):e25–e33 — Search PubMed
- Spitzer PG, Hammer SM, Karchmer AW. Treatment of Listeria monocytogenes infection with trimethoprim-sulfamethoxazole: case report and review of the literature. Rev Infect Dis. 1986;8(3):427–430 — Search PubMed
Connections
- All Bacteria
- Listeria Treatment and Prevention Hub
- Food Safety and Prevention
- Outbreak Investigation and Recalls
- Symptoms and Diagnosis Hub
- Invasive Listeriosis and Meningitis
- Listeria in Pregnancy and Newborns
- Listeria Monocytogenes Overview
- Meningitis
- Endocarditis