Listeria monocytogenes: Listeriosis, Food Safety, and Pregnancy Risks
Symptoms & Diagnosis
A food poisoning bug that kills — listeria is rare but targets the most vulnerable.
Invasive Listeriosis
Bacteremia, meningitis, and encephalitis in immunocompromised patients and the elderly.
Pregnancy & Newborns
Why pregnant women must avoid deli meats — miscarriage, stillbirth, and neonatal sepsis.
Diagnosis Tests
Blood cultures, CSF cultures, food testing, and the long incubation that delays diagnosis.
Treatment & Prevention
Ampicillin IV and the food safety measures that prevent listeria infection.
Antibiotic Treatment
Ampicillin + gentamicin for invasive listeria — and why cephalosporins don't work.
Food Safety
The high-risk foods — deli meats, soft cheeses, smoked salmon — and refrigerator safety.
Outbreak Investigation
How listeria outbreaks are traced back to single food facilities, and how recalls work.
Listeria is a foodborne bacterium remarkable for thriving in refrigerated food and posing catastrophic risk to pregnant women — causing miscarriage, stillbirth, and newborn meningitis — as well as to the elderly and immunocompromised. With a case-fatality rate of 20–30%, Listeria monocytogenes is the deadliest common foodborne pathogen in the United States, even though it causes far fewer total illnesses each year than Salmonella or Campylobacter. Understanding which foods carry it, who must avoid them, and when to seek care can be life-saving.
Table of Contents
- What Listeria Is
- Why It Is Uniquely Dangerous
- Who Is at High Risk
- How Listeria Gets Into Food
- Symptoms
- Diagnosis and Treatment
- Food Safety and Prevention
- Research Papers
- Connections
- Featured Videos
What Listeria Is
Listeria monocytogenes is a small, rod-shaped, Gram-positive bacterium found widely in the environment — in soil, water, decaying plant material, and the intestines of many animals. Unlike most foodborne pathogens, it does not need warmth to multiply. It grows at temperatures as low as 0°C (32°F), meaning it can reproduce inside a properly functioning refrigerator. This cold-tolerance is its most dangerous and unusual property: ordinary refrigeration, which stops almost every other foodborne pathogen, does nothing to control Listeria growth.
The bacterium was first isolated and described in 1926 by E.G.D. Murray and colleagues in Cambridge, England, from the blood and liver of laboratory rabbits. It was later named in honor of the pioneering surgeon and antiseptic champion Joseph Lister. Human foodborne listeriosis was not clearly recognized as a clinical entity until major outbreaks in North America and Europe in the 1980s established the link between contaminated food and severe disease in pregnant women and immunocompromised patients.
In the United States, the CDC estimates approximately 1,600 people develop invasive listeriosis each year and about 260 die — a toll disproportionately large for the number of cases, and one that makes Listeria the leading cause of death among all foodborne pathogens tracked in the US.
Why It Is Uniquely Dangerous
Most foodborne pathogens cause disease by staying in the gut. Listeria monocytogenes is different: it is one of the very few food-transmitted bacteria that routinely crosses into the bloodstream, the brain, and — during pregnancy — the placenta. This ability to invade deep tissue is what makes it so lethal compared with, say, Salmonella, which kills far fewer of the people it infects.
The key to this invasion is a set of specialized proteins, most famously internalins A and B (InlA and InlB), which the bacterium uses to trick normal cells into swallowing it whole. Once inside a cell it dissolves the membrane of the compartment trapping it, escapes into the cytoplasm, hijacks the cell's own actin skeleton to propel itself from cell to cell, and spreads without ever returning to the bloodstream — making it invisible to antibodies and difficult for the immune system to reach. This "intracellular stealth" is a major reason immunocompromised people, in whom cell-mediated (T-cell) immunity is weak, are hit so much harder.
The bacterium also produces a pore-forming toxin called listeriolysin O (LLO) that damages host cell membranes and is essential to its virulence. These properties together — cold-tolerance, intracellular lifestyle, listeriolysin toxin, and placental tropism — are what set L. monocytogenes apart from other foodborne bacteria.
Who Is at High Risk
For healthy adults under about 65, Listeria in food causes at most a mild, self-limiting gastroenteritis. The groups at serious risk of invasive disease are well-defined:
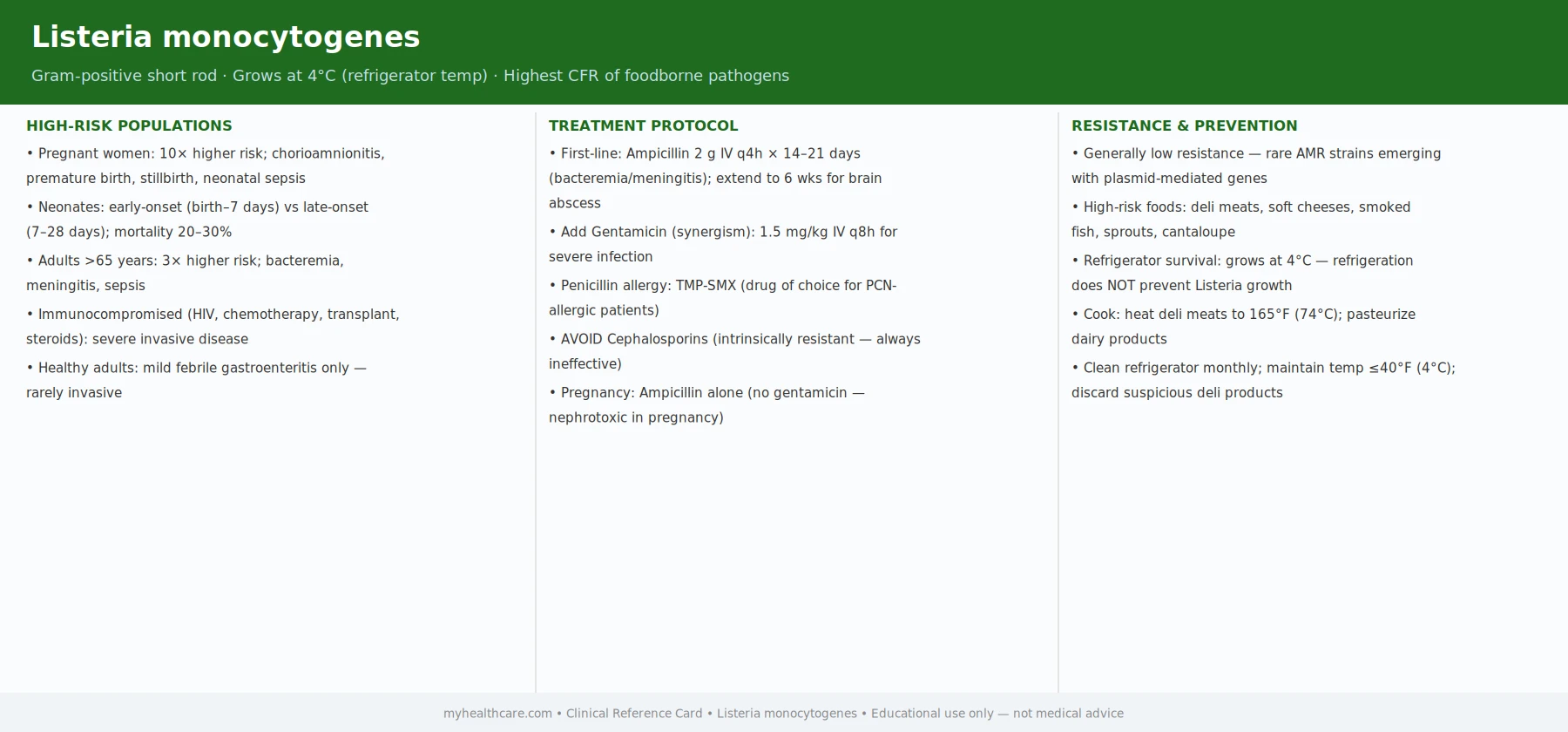
- Pregnant women are about 10 times more likely than the general population to develop invasive listeriosis. Pregnancy alters the immune system in ways that suppress the cell-mediated responses needed to clear the bacteria. The infection can remain mild in the mother — sometimes just a fever and flu-like illness — while spreading silently through the bloodstream to the placenta. Consequences include miscarriage (especially in early-to-mid pregnancy), stillbirth, premature birth, and severe infection in the newborn (neonatal listeriosis), most commonly taking the form of septicemia or meningitis.
- Adults aged 65 and older account for the majority of non-pregnancy-associated listeriosis cases. Immune function declines with age, and older adults often take medications that further impair it.
- People with weakened immune systems due to HIV/AIDS, organ transplantation (and the anti-rejection drugs that come with it), cancer and chemotherapy, long-term steroid use, diabetes, kidney or liver disease, or other conditions that suppress T-cell immunity.
- Newborns infected in the womb or at birth, who lack fully developed immune defenses.
Anyone outside these groups who ingests Listeria-contaminated food will usually notice nothing, or at most a brief stomach upset that clears on its own. This means that when a contaminated food product is identified, public warnings are specifically directed at the high-risk groups above — not the entire population.
How Listeria Gets Into Food
Listeria monocytogenes is nearly ubiquitous in the environment, so it enters food at multiple points along the supply chain — from farm soil and water, to processing equipment and food-plant surfaces, to retail and home kitchens. Several properties make controlling it in food production unusually difficult:
- Biofilm formation. Listeria adheres stubbornly to food-contact surfaces and forms thick biofilms that are highly resistant to standard cleaning and sanitizing procedures. A contaminated slicer, conveyor belt, or drain in a deli or ready-to-eat processing facility can become a persistent source of contamination for months or years.
- Cold-chain survival and growth. Refrigeration does not stop Listeria. Ready-to-eat foods with a long refrigerator shelf life — deli meats, hot dogs, soft cheeses — give the bacteria ample time to multiply to infectious doses even at 4°C.
- No cooking step after contamination. Ready-to-eat foods are consumed without reheating, so post-processing contamination from a plant environment bypasses the kill step that cooking would otherwise provide.
The foods most frequently linked to listeriosis outbreaks and recalls in the US include: ready-to-eat deli meats and hot dogs (the most common source historically), soft and semi-soft cheeses made from unpasteurized milk (Brie, Camembert, queso fresco, queso blanco, feta), smoked seafood (particularly cold-smoked or "nova-style" salmon), pre-packaged salads and sprouts, and refrigerated caramel apples (a surprising outbreak vehicle in 2014). Pasteurized dairy products are generally safe, though post-pasteurization contamination in a plant can still occur.
Symptoms
Listeriosis presents in two very different ways depending on who is infected:
Non-invasive gastroenteritis (healthy adults)
In healthy, non-pregnant adults, Listeria typically causes mild, self-limited gastroenteritis that resembles many other foodborne illnesses: nausea, watery diarrhea, cramps, fever, and muscle aches. Symptoms usually appear within 24 hours of eating a heavily contaminated food and resolve within a few days without treatment. This form is likely underdiagnosed because most people assume a brief stomach illness and do not seek testing.
Invasive listeriosis (high-risk groups)
In pregnant women, elderly adults, and immunocompromised people, the bacteria can escape the gut and invade the bloodstream and organs. The incubation period for invasive disease is typically 1 to 4 weeks but can extend to 70 days — much longer than most foodborne illnesses, which makes tracing the contaminated food difficult. Symptoms of invasive disease include:
- Fever and flu-like symptoms (muscle aches, fatigue, headache) that may seem unremarkable at first.
- Bacteremia (bacteria in the bloodstream) — septicemia that can progress to septic shock.
- Meningitis or meningoencephalitis — severe headache, stiff neck, confusion, loss of balance, and sensitivity to light. Listeria is the third most common cause of bacterial meningitis in adults in high-income countries.
- Encephalitis — inflammation of the brain itself, sometimes causing seizures, altered consciousness, or focal neurological deficits.
- In pregnant women: fever, chills, and backache, often without obvious gastrointestinal symptoms; the fetus may not show any symptoms until it dies in utero, making prompt treatment urgent when a pregnant woman has a febrile illness and any plausible food exposure.
Invasive listeriosis requires hospitalization and intravenous antibiotics. Even with optimal treatment, the overall case-fatality rate is approximately 20–30%, and neurological complications can cause permanent disability in survivors.
Diagnosis and Treatment
Diagnosis is made by blood culture in cases of bacteremia, or cerebrospinal fluid (CSF) culture when meningitis is suspected. Because the symptoms of invasive listeriosis can initially resemble influenza or other common febrile illnesses, especially in pregnant women, the diagnosis is often delayed unless the clinician has a high index of suspicion. Stool cultures can detect Listeria but are not routinely used for clinical diagnosis of invasive disease; they are more useful in outbreak investigations.
The standard treatment for invasive listeriosis is intravenous ampicillin, typically in combination with gentamicin (an aminoglycoside antibiotic that acts synergistically with ampicillin to kill Listeria more effectively). The addition of gentamicin is particularly important in severe cases, including meningitis, and in immunocompromised patients. For patients who are truly allergic to penicillin, trimethoprim-sulfamethoxazole (TMP-SMX) is the standard alternative.
A critically important point for clinical management: Listeria is intrinsically resistant to cephalosporins — the class of antibiotics most commonly used empirically for bacterial meningitis. Cephalosporins (including ceftriaxone, which is a mainstay of empirical meningitis treatment) do not work against Listeria. In any meningitis patient over 50, pregnant, or immunocompromised, ampicillin must be added to the empirical regimen to cover this organism, even before culture results are available. Missing this can be fatal.
Duration of treatment depends on the site of infection: bacteremia alone is typically treated for 2 weeks; meningitis for 3 weeks; and encephalitis or brain abscess for 6 weeks or longer.
Food Safety and Prevention
Because listeriosis is so dangerous in high-risk groups and there is no vaccine, prevention centers entirely on food safety practices and targeted dietary avoidance for vulnerable individuals.
For pregnant women and immunocompromised people
The CDC and FDA specifically advise these groups to avoid:
- Deli meats and hot dogs unless heated until steaming hot (internal temperature 165°F / 74°C) immediately before eating.
- Soft cheeses made with unpasteurized milk: queso fresco, queso blanco, Brie, Camembert, blue-veined cheeses. Hard cheeses and pasteurized-milk cheeses are generally safe.
- Refrigerated pâtés or meat spreads (canned or shelf-stable versions are safe).
- Refrigerated smoked seafood (e.g., smoked salmon, trout, whitefish) unless it is cooked as part of a dish. Canned or shelf-stable smoked seafood is safe.
- Unpasteurized (raw) milk and any foods made with it.
- Raw sprouts of any kind.
For everyone
- Follow use-by dates on perishable ready-to-eat foods — Listeria growth in a package can accelerate even at refrigerator temperatures over time.
- Keep the refrigerator at or below 40°F (4°C) and check regularly with a thermometer.
- Clean the refrigerator regularly, including the vegetable drawers, and promptly wipe up spills from deli-meat packages or raw meat.
- Wash hands thoroughly before and after handling food, and wash produce well before eating.
- Pay attention to food recalls: the FDA and USDA actively monitor for Listeria contamination in the food supply and issue recalls when a contaminated lot is found. Sign up for recall alerts at foodsafety.gov.
Research Papers
- Cartwright EJ, Jackson KA, Johnson SD, Graves LM, Silk BJ, Mahon BE. Notes from the Field: Outbreak of Listeriosis Associated with Consumption of Packaged Salad — United States and Canada, 2015–2016. MMWR Morb Mortal Wkly Rep. 2016;65(33):879–881. doi:10.15585/mmwr.mm6533a6 — CDC outbreak investigation linking Listeria cases in two countries to pre-packaged salad, illustrating how ready-to-eat produce can carry the pathogen despite refrigerated handling.
- Orsi RH, Wiedmann M. Characteristics and distribution of Listeria spp., including Listeria species newly described since 2009. Appl Microbiol Biotechnol. 2016;100:5273–5287. doi:10.1016/j.meegid.2015.08.008 — Comprehensive review of the evolution and epidemiology of L. monocytogenes in Europe and the United States, covering clonal lineages, outbreak strains, and food-chain ecology.
- Pouillot R, Hoelzer K, Jackson KA, Henao OL, Silk BJ. Relative Risk of Listeriosis in Foodborne Disease Active Surveillance Network (FoodNet) Sites According to Age, Pregnancy, and Ethnicity. Clin Infect Dis. 2012;54(Suppl 5):S405–S410. doi:10.1089/fpd.2017.2419 — US surveillance study on implicated food products for listeriosis and shifts in serovars over recent decades, showing the evolution of outbreak vehicles from deli meat toward produce and dairy.
- Schüpbach-Regula G, Coucheney E, Grunow R, et al. Neonatal Listeriosis with Central Nervous System Involvement: A Case Series and Review of the Literature. Antibiotics. 2025;14(2):206. doi:10.3390/antibiotics15020206 — Case series and literature review of neonatal listeriosis with CNS involvement, detailing clinical presentations, ampicillin-based regimens, and long-term neurodevelopmental outcomes.
- Al Riyami I, Al Rawahi BN, Al Khabouri M, Al Hajri M. Maternal Listeriosis Presenting with Suspected Meningitis in Late Pregnancy: A Case Report. Cureus. 2025;17(5):e99839. doi:10.7759/cureus.99839 — Case report illustrating the diagnostic challenge of maternal listeriosis mimicking meningitis in the third trimester, underscoring the importance of blood culture and early ampicillin therapy in febrile pregnant patients.