Clostridium difficile (C. diff): Causes, Symptoms, Treatment, and Prevention
Symptoms & C. diff
Why antibiotics open the door to C. diff and what the infection feels like.
Diarrhea & Colitis
Watery diarrhea, abdominal cramps, and the pseudomembranous colitis pattern.
Severe C. diff
Toxic megacolon, colectomy, ICU admission, and who is most at risk of dying.
Diagnosis Tests
NAAT, GDH antigen, toxin EIA, and the two-step testing algorithm.
Treatment & Prevention
Stopping the offending antibiotic, oral vancomycin, and microbiome restoration.
Antibiotic Treatment
Oral vancomycin, fidaxomicin, and bezlotoxumab for recurrent CDI.
Fecal Transplant
FMT for recurrent CDI — how donor stool restores a healthy microbiome.
Infection Control
Spore survival on surfaces, soap (not alcohol gel) for hand hygiene, antibiotic stewardship.
Clostridium difficile — commonly called C. diff — is a spore-forming bacterium that infects the lining of the colon and causes severe diarrhea, cramping, and inflammation of the colon (colitis). Unlike most bacterial infections, C. diff does not spread through contaminated food or water; it strikes when antibiotics wipe out the protective bacteria that normally live in the gut, leaving an opening for C. diff to move in and multiply. It is one of the most common and most dangerous healthcare-associated infections in the United States, responsible for nearly half a million illnesses and tens of thousands of deaths each year. For people who develop it once, it has a troubling tendency to come back — but a growing set of treatments, including a therapy that transfers healthy gut bacteria from a donor, is changing that picture.
Table of Contents
- What C. diff Is
- How Antibiotics Enable It
- Symptoms
- Severity Levels
- Diagnosis
- Treatment
- Prevention
- Research Papers
- Connections
- Featured Videos
What C. diff Is
Clostridium difficile (recently renamed Clostridioides difficile in scientific literature, though C. diff is still the everyday term) is a gram-positive, anaerobic bacterium that produces two potent toxins — Toxin A and Toxin B — that damage the cells lining the colon, trigger intense inflammation, and cause the watery, often bloody diarrhea that defines the infection.
What makes C. diff uniquely dangerous is its ability to form spores: hardy, dormant structures that can survive on surfaces, hands, and equipment for months, are completely resistant to most alcohol-based hand sanitizers, and can only be destroyed by soap-and-water handwashing or bleach-based cleaning. Spores are shed in the stool of infected people and swallowed by the next host, where they germinate in the colon and begin producing toxins.
C. diff is carried asymptomatically by a small percentage of healthy adults, but in the gut of someone whose normal microbial ecosystem has been disrupted — most commonly by antibiotics — it finds an almost uncontested environment to grow. Rates are highest in hospitals and long-term care facilities, where the combination of antibiotic use, vulnerable patients, and environmental contamination creates ideal conditions.
How Antibiotics Enable It
The human gut normally hosts trillions of bacteria in a balanced community that competes for space and nutrients and produces compounds that keep pathogens at bay. When antibiotics are taken — even a short course for an unrelated condition such as a dental procedure or a urinary tract infection — they kill not just the target bacteria but large numbers of these protective gut residents.
C. diff spores, already present in the environment or consumed unknowingly, are largely unaffected by antibiotics. Once the protective community is thinned out, C. diff germinates, colonizes the now-open colon, and begins releasing toxins. This is why C. diff infection almost always begins during antibiotic treatment or in the days and weeks after a course ends.
The antibiotics most strongly associated with triggering C. diff include clindamycin, fluoroquinolones (such as ciprofloxacin and levofloxacin), and cephalosporins — not because they are more toxic to patients, but because they are particularly disruptive to the gut microbiome. However, virtually any antibiotic can trigger C. diff in a susceptible person. Additional risk factors include advanced age, hospitalization, proton pump inhibitor use, immune suppression, inflammatory bowel disease, and prior C. diff infection.
Symptoms
Symptoms of C. diff infection typically begin 2 to 3 days after antibiotic exposure but can appear as late as 8 weeks afterward. The hallmark is:
- Watery diarrhea — typically three or more loose stools per day, sometimes many more. The diarrhea is often described as foul-smelling.
- Abdominal cramping and pain, often in the lower abdomen, that may worsen before a bowel movement.
- Fever, particularly in moderate to severe cases.
- Nausea and reduced appetite.
- Tenderness over the abdomen when pressed.
In mild cases, patients feel miserable but remain stable. As the infection worsens, the volume and frequency of diarrhea increase, fever rises, and signs of dehydration appear. Blood in the stool, while less common than in some other colitis types, can be present in severe cases.
Seek medical care immediately if you develop diarrhea during or shortly after antibiotics, especially if it is severe, associated with fever, or accompanied by signs of dehydration. C. diff is not a condition to manage at home with over-the-counter remedies.
Severity Levels
Infectious disease guidelines categorize C. diff infection into three tiers, because the appropriate treatment and urgency differ significantly between them.
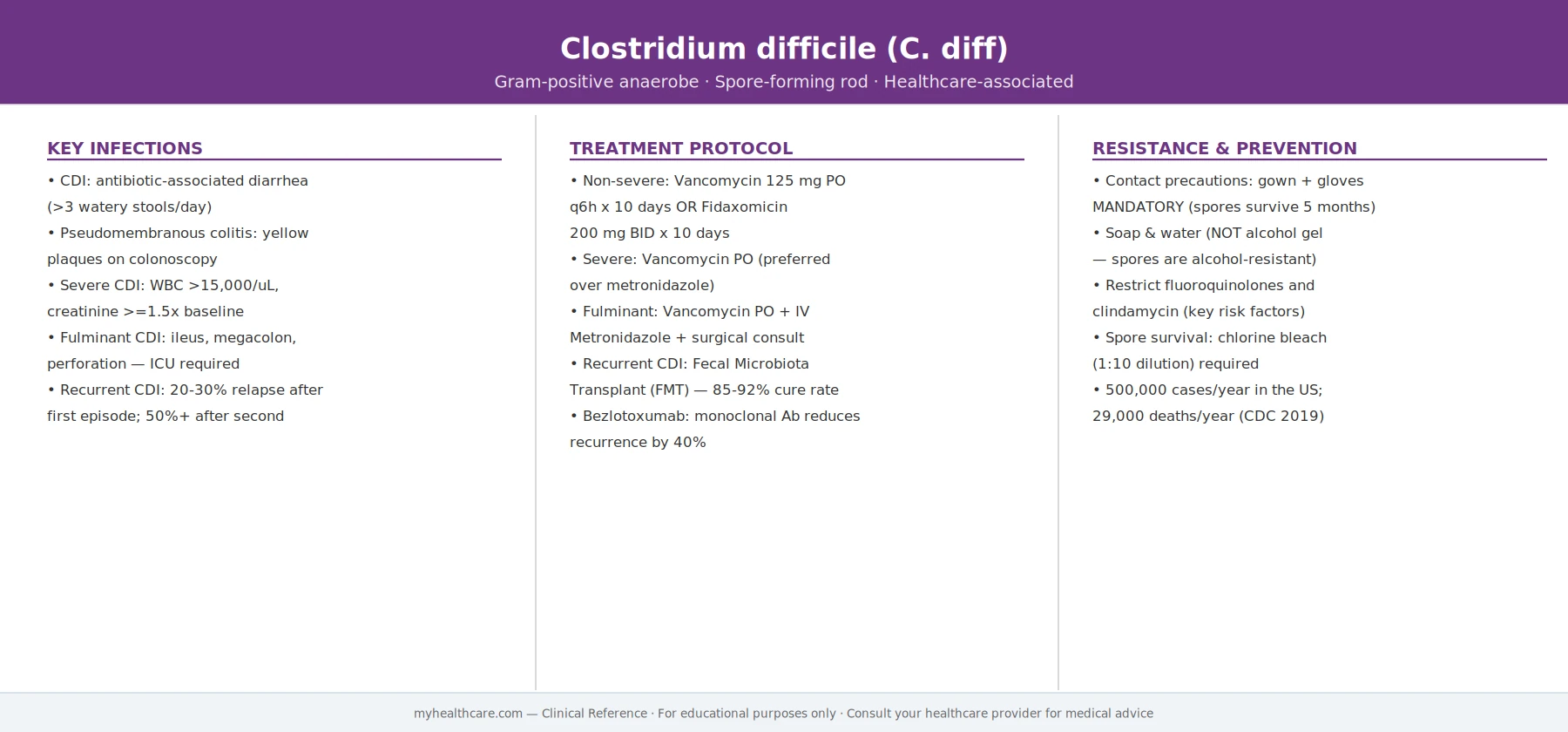
- Mild to moderate: Diarrhea with a white blood cell count below 15,000 cells/mm³ and a creatinine level below 1.5 times the patient's baseline. Most patients fall into this category and respond well to oral antibiotics.
- Severe: White blood cell count of 15,000 or higher, or creatinine at least 1.5 times baseline. These patients are sicker and at risk of escalating quickly. Some guidelines include a fever above 38.5°C (101.3°F) or significant abdominal pain and tenderness as additional markers.
- Fulminant (formerly severe-complicated): The most dangerous presentation — patients develop hypotension (dangerously low blood pressure), shock, ileus (the bowel stops moving), or toxic megacolon (massive dilation of the colon with risk of rupture). This is a surgical emergency with high mortality. Emergency colectomy — surgical removal of the colon — may be necessary to save the patient's life.
Recurrent infection — C. diff coming back after an apparently successful course of treatment — is a major clinical problem. Approximately 15–25% of patients have one recurrence, and having recurred once significantly raises the risk of recurrence again. Recurrences happen because antibiotics that treat C. diff also suppress the remaining protective gut bacteria, and because C. diff spores left in the environment or colon can germinate anew once treatment ends.
Diagnosis
C. diff is diagnosed by laboratory testing of a stool sample. The main tests are:
- Nucleic acid amplification test (NAAT / PCR): Detects C. diff DNA in stool with very high sensitivity. Can produce false positives by detecting colonized patients who carry the bacteria but are not producing toxins. For this reason, many labs use a two-step approach.
- Enzyme immunoassay (EIA) for toxins A and B: Directly detects the toxins that cause illness. Less sensitive than PCR but more specific for active, toxin-producing disease. A positive toxin EIA with diarrhea is strong evidence of true infection.
- Glutamate dehydrogenase (GDH) antigen test: A rapid screening test for a C. diff enzyme. High sensitivity makes it useful as a first screen; positive GDH results are typically confirmed by toxin EIA or PCR.
- Two-step or three-step algorithms combining these tests are now standard in most hospitals and help balance sensitivity with the need to avoid treating colonized but asymptomatic patients.
Importantly, testing should only be done on unformed (liquid or soft) stool from a patient with clinically significant diarrhea. Testing formed stool or patients without symptoms leads to false-positive diagnoses and unnecessary treatment. Repeat testing during the same episode is not recommended — a negative test in someone with ongoing diarrhea does not rule out C. diff if clinical suspicion is high, but repeat testing in the same episode rarely adds information.
In severe or fulminant cases, imaging (CT scan of the abdomen and pelvis) is used to detect complications such as toxic megacolon, perforation, or pericolitis.
Treatment
The first step when C. diff is diagnosed is to stop the offending antibiotic if at all possible. In some patients, this alone is enough to allow the gut flora to recover and the infection to resolve. In most patients, however, C. diff requires specific treatment.
Antibiotic Treatment
Treatment depends on severity:
- Fidaxomicin (Dificid) is now the preferred first-line antibiotic for non-severe C. diff in most patients. It is a narrow-spectrum antibiotic that acts locally in the gut, kills C. diff, and — critically — causes less disruption to the broader gut flora than vancomycin, which translates to a significantly lower rate of recurrence. It is given orally for 10 days.
- Oral vancomycin is an effective first-line alternative and is preferred for severe infection. It is given in a standard or tapered-and-pulsed regimen depending on whether the patient has recurrent disease.
- Metronidazole, once the most common treatment, is now only recommended for mild disease when the preferred agents are unavailable or too costly. It has a higher recurrence rate and is less effective in severe disease.
- For fulminant infection, high-dose oral vancomycin is used, often combined with intravenous metronidazole. Surgical consultation is essential.
Bezlotoxumab
Bezlotoxumab (Zinplava) is a monoclonal antibody — not an antibiotic — that works by neutralizing C. diff Toxin B. It is given as a single intravenous infusion during a course of antibiotic treatment. It does not treat the current infection but significantly reduces the risk of recurrence, particularly in patients at high risk (age 65+, prior C. diff, compromised immune system, severe infection). The 2021 IDSA/SHEA guidelines recommend considering it in high-risk patients.
Fecal Microbiota Transplantation (FMT)
FMT is the most effective treatment for recurrent C. diff, with cure rates of 80–90% or higher in clinical trials — dramatically better than repeated courses of antibiotics alone. The procedure involves transferring processed stool from a healthy, thoroughly screened donor into the colon of the patient, rapidly restoring a diverse gut microbial community that outcompetes C. diff.
FMT can be delivered by colonoscopy, enema, nasogastric tube, or (increasingly) oral capsules containing freeze-dried donor material. The FDA approved the first standardized FMT products in 2022–2023, making it a more accessible, standardized option. FMT is recommended for patients with two or more recurrences of C. diff who have not responded to antibiotic optimization alone.
Probiotics
The evidence for probiotics in preventing or treating C. diff infection is mixed and inconsistent. Some meta-analyses suggest modest benefit in prevention when given during antibiotic courses, but no specific probiotic product is approved for C. diff treatment, and they are not part of standard guideline recommendations. They may cause harm in severely ill or immunocompromised patients.
Prevention
Preventing C. diff requires action at three levels: the patient, the healthcare setting, and society.
Hand Hygiene
C. diff spores are not killed by alcohol-based hand sanitizers — this is a critical and widely misunderstood point. Soap and water is essential for removing spores from hands. Healthcare workers caring for C. diff patients must use soap and water before and after patient contact. Visitors and patients should also wash hands, particularly before eating and after using the toilet.
Contact Precautions in Healthcare Settings
Patients diagnosed with C. diff are placed in contact precautions: a private room when possible, gown and gloves for anyone entering the room, and dedicated equipment that stays in the room. Environmental cleaning with bleach-based disinfectants (at least 1:10 dilution of household bleach) is required to kill spores on surfaces, toilets, and equipment. Standard quaternary ammonium disinfectants do not kill C. diff spores and must not be used as the sole cleaning agent in C. diff rooms.
Antibiotic Stewardship
Since antibiotics are the root cause of most C. diff infections, using them more carefully is the most important systemic prevention strategy. Antibiotic stewardship programs — hospital-based teams that guide which antibiotics are prescribed, at what dose, and for how long — have been shown in multiple studies to significantly reduce C. diff rates in hospitals. Key principles include: using the narrowest-spectrum antibiotic appropriate for the infection, prescribing for the shortest effective duration, and avoiding antibiotics in cases where they are not genuinely needed (such as viral respiratory infections).
Patient Risk Reduction
For individual patients, the key message is: only take antibiotics when a doctor determines they are genuinely necessary, finish prescribed courses completely, and alert any healthcare provider to a prior history of C. diff before starting a new antibiotic course. People who have had C. diff before are at substantially higher risk of recurrence with any future antibiotic use.
Research Papers
- Johnson S, Lavergne V, Skinner AM, et al. Clinical Practice Guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 Focused Update Guidelines on Management of Clostridioides difficile Infection in Adults. Clin Infect Dis. 2021;73(5):e1029–e1044. doi:10.1093/cid/ciab549 — The 2021 IDSA/SHEA focused update recommending fidaxomicin as preferred first-line therapy, defining severity tiers, and endorsing FMT and bezlotoxumab for recurrent disease.
- Louie TJ, Miller MA, Mullane KM, et al. (OPCDT-10 Study Group). Fidaxomicin versus Vancomycin for Clostridium difficile Infection. Pediatrics in Review. 2012 (replicated report). doi:10.1016/j.yped.2011.06.018 — Phase 3 trial showing fidaxomicin was non-inferior to vancomycin for clinical cure but produced significantly fewer recurrences, establishing fidaxomicin as the preferred agent.
- van Nood E, Vrieze A, Nieuwdorp M, et al. Duodenal Infusion of Donor Feces for Recurrent Clostridium difficile. N Engl J Med. 2013;368(5):407–415. doi:10.1056/nejmoa1205037 — Landmark randomized controlled trial demonstrating that fecal microbiota transplantation cured 81% of recurrent C. diff cases after a single infusion, compared with 31% for vancomycin, establishing FMT as a standard of care.
- Taibi A, Comelli EM. Bezlotoxumab in Patients with a Primary Clostridioides difficile Infection: A Literature Review. Antibiotics. 2022;11(11):1495. doi:10.3390/antibiotics11111495 — Systematic review of bezlotoxumab evidence, summarizing its mechanism of action (neutralizing Toxin B) and clinical utility in reducing recurrence among high-risk patients.
- Tagashira Y, Sakamoto N, Terao K, et al. Effects of Antibiotic Stewardship Program on Antibiotic Consumption and the Incidence of Clostridioides difficile Infection. Antibiotics. 2025;14(2):112. doi:10.3390/antibiotics15020112 — Prospective study showing that a structured antibiotic stewardship program significantly reduced both total antibiotic consumption and C. diff infection rates in a hospital setting, supporting stewardship as a primary prevention tool.
Connections
- C. diff: History and Discovery — where today’s treatment came from — Hall and O’Toole’s 1935 isolate from healthy newborns, the pseudomembranous-colitis mystery, Bartlett closing the loop in 1978, the NAP1/027 epidemic strain, and the rise of fecal transplant.
- Inflammatory Bowel Disease
- Gastroenterology Conditions
- Infectious Disease
- SIBO (Small Intestinal Bacterial Overgrowth)
- Irritable Bowel Syndrome
- All Conditions