Oil Pulling
Oil pulling is an old Ayurvedic mouth-care practice: you take a spoonful of edible oil — most often coconut or sesame — swish it slowly around your mouth for several minutes, and then spit it out. It has become popular again through wellness blogs and social media, where it is sometimes sold as a way to “detox” the body, whiten teeth, or even cure disease. This page is meant to separate the modest, real evidence from the tall claims, in plain language, without hype. The short version is this: a handful of small, mostly low-quality studies suggest oil pulling may slightly reduce dental plaque, gum inflammation, and the bacteria linked to bad breath — but it has never been shown to beat ordinary brushing, flossing, and fluoride, and the “detox” and disease-curing claims have no scientific support at all. Used gently as an add-on, it is probably harmless for most healthy adults. Used as a replacement for real dental care, it is a mistake. There is also one genuine safety caveat worth knowing about — a rare lung problem called lipoid pneumonia — which we cover honestly below.
Table of Contents
- What Oil Pulling Is and How It Is Done
- Ayurvedic Origins: Kavala and Gandusha
- Which Oil? Coconut, Sesame, or Sunflower
- What the Evidence Actually Shows
- How It Might Work: Proposed Mechanisms
- The Debunked Claims
- The Real Safety Concern: Lipoid Pneumonia
- Not a Substitute for the Basics
- How to Try It Safely as an Adjunct
- The Honest Bottom Line
- Research Papers
- Connections
- Featured Videos
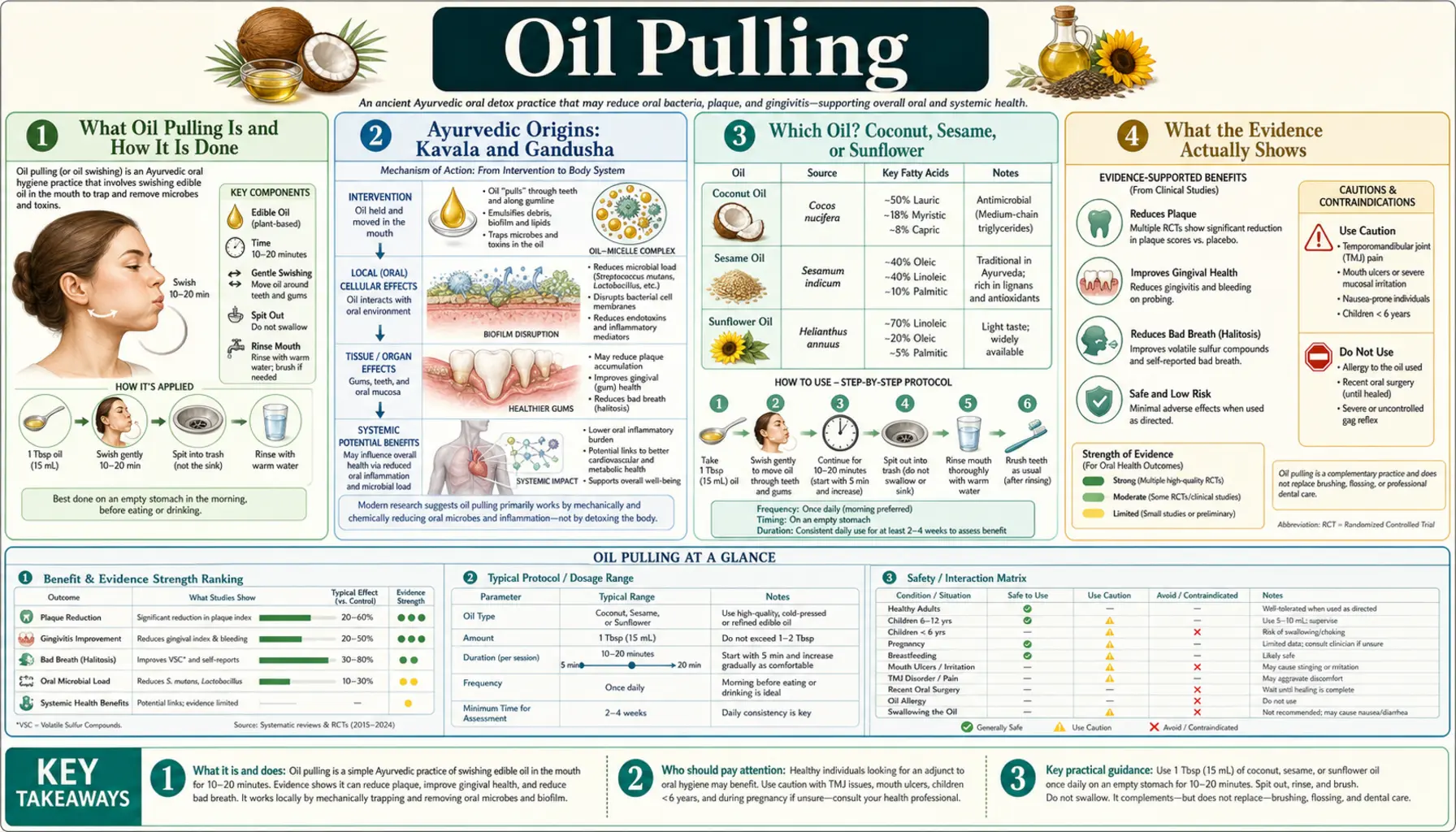
What Oil Pulling Is and How It Is Done
At its simplest, oil pulling means holding a small amount of edible oil in your mouth and swishing it around — pulling and pushing it between your teeth — for a stretch of time, then spitting it out and rinsing. The name is a rough translation of the practice’s traditional idea that the swishing action “pulls” unwanted material out of the mouth. Nothing is swallowed; the oil is meant to be worked around and then discarded.
A typical modern routine looks like this:
- Take about one tablespoon (roughly 10–15 mL) of oil first thing in the morning, before eating or drinking.
- Swish gently and steadily for several minutes — many traditional and popular protocols suggest up to 15 to 20 minutes, though the studies that have tested it often used shorter times.
- Keep the motion relaxed. Vigorous swishing for a long time can tire the jaw and cheeks, which is one reason many people cut the time short.
- Spit the used oil into a trash can or paper towel — not the sink or toilet, because oil can congeal and clog pipes.
- Rinse with water, then brush and floss as usual.
The oil should be spat out and never swallowed, because by the end it holds saliva, food debris, and oral microbes. It is important to understand that even in the studies where it helped a little, oil pulling was tested as an addition to normal hygiene or against a mouthwash — not as a stand-alone replacement for brushing and flossing.
Ayurvedic Origins: Kavala and Gandusha
Oil pulling comes from Ayurveda, the traditional system of medicine of the Indian subcontinent, where oil-based mouth care is described under two related terms. In gandusha, the mouth is filled completely with oil, held nearly still, and then released. In kavala (sometimes written kavala graha), a smaller amount is taken and actively swished or gargled. The modern “oil pulling” that circulates online is closest to kavala.
Classical Ayurvedic texts recommended these practices as part of daily self-care (dinacharya) and attributed to them a long list of benefits — stronger teeth and jaws, a clearer voice, relief from dry mouth and cracked lips, and general oral freshness. Sesame oil was the traditional oil of choice in much of this literature. It is fair and respectful to note that these were practical observations from a pre-microbiology era, offered as part of a whole lifestyle system. They are the historical root of the practice, but they are not clinical evidence, and it would be a mistake to treat centuries-old recommendations as if they had been tested the way a modern drug is. The honest question for today is a narrower one: when researchers actually measure plaque, gum inflammation, and bacteria, does oil pulling do anything?
Which Oil? Coconut, Sesame, or Sunflower
Three oils dominate both tradition and research. They differ in taste, texture, and chemistry, and each has its advocates.
Sesame oil
Sesame oil is the classical Ayurvedic choice and the oil used in several of the earliest modern studies. It contains antioxidant compounds such as sesamol and sesamin. It has a distinct nutty flavor that some people find pleasant and others do not.
Coconut oil
Coconut oil is the most popular choice today, largely because of its mild taste and because it is rich in a medium-chain fatty acid called lauric acid, which has antimicrobial activity in laboratory settings. Most of the recent oil-pulling trials have used coconut oil. One practical quirk: coconut oil is solid at cooler room temperatures, so it needs a few seconds of swishing to melt in the mouth.
Sunflower oil
Sunflower oil appears in the older research too, often as a comparison oil alongside sesame. It is inexpensive and neutral-tasting.
Here is the honest part: no high-quality study has clearly shown one oil to be meaningfully better than another for oral health. Coconut oil is the most studied simply because it became the most fashionable, not because it was proven superior head-to-head. If you decide to try oil pulling, the “best” oil is mostly the one you find tolerable enough to use consistently. Use a clean, food-grade oil you would be comfortable eating.
What the Evidence Actually Shows
This is the heart of the matter, so it deserves a careful, honest look. There are real randomized studies of oil pulling, and several of them did report improvements. But the improvements need to be read alongside the serious limitations of the studies.
What the studies found
- Plaque and gingivitis: Small trials, several from the same research group in India, reported that daily oil pulling reduced plaque scores and signs of gum inflammation over two to four weeks compared with a person’s starting point.
- Bacteria: Some trials measured a drop in Streptococcus mutans, a bacterium tied to tooth decay, in plaque and saliva after a period of oil pulling.
- Bad breath (halitosis): A small pilot trial reported reductions in the microorganisms associated with mouth odor.
Why those findings must be read cautiously
When independent reviewers pooled and appraised these studies, they consistently reached a sober conclusion: the research is weak. The main problems are:
- Small and short. Most trials enrolled only a few dozen participants and ran for a few weeks. Small, brief studies easily produce results that do not hold up.
- High risk of bias. Blinding is hard — you can taste and feel oil in your mouth — and many trials had methodological weaknesses. Several came from the same small circle of investigators.
- Improvement over baseline is not the same as being useful. Doing almost any focused oral routine tends to improve numbers a bit, partly because people who are being watched brush more carefully (the “Hawthorne effect”).
- Rarely better than the standard. When oil pulling was compared against chlorhexidine, the well-established antiseptic mouthwash, it was generally not superior; chlorhexidine matched or outperformed it. And no study shows oil pulling beating simple, correct brushing with fluoride toothpaste.
A 2020 systematic review of coconut-oil pulling put it plainly: the existing trials are at high risk of bias and do not provide reliable evidence that oil pulling improves oral health. So the fair summary is not “it does nothing” and not “it works” — it is: the signal is small, the studies are shaky, and nothing suggests it can replace proven dental care.
How It Might Work: Proposed Mechanisms
If oil pulling does anything at all, researchers have proposed a few plausible ways it could nudge oral bacteria and plaque, though none is firmly proven.
- Mechanical action. Swishing any liquid vigorously for several minutes physically loosens and washes away food debris and loosely attached plaque, much like a long rinse would. Part of any benefit may simply be the swishing, not the oil itself.
- Saponification (a soap-like effect). Alkaline conditions and enzymes in the mouth can partly turn fats into soap-like substances. The idea is that these could help emulsify and lift away the sticky bacterial film. One in-vitro study from the practice’s proponents explored this, but it remains a hypothesis.
- A possible antimicrobial contribution. Coconut oil is high in lauric acid, which can inhibit some bacteria in the lab. Whether enough activity survives the brief, diluted, saliva-mixed conditions of real oil pulling to matter clinically is unknown.
- Reduced bacterial adhesion. A thin oily coating might make it slightly harder for microbes to stick to tooth surfaces, though this is speculative.
The key takeaway on mechanism: these are reasonable ideas, mostly supported by test-tube work rather than by strong evidence in people’s mouths. A believable mechanism is not proof of a meaningful benefit.
The Debunked Claims
Oil pulling’s biggest problem is not the practice itself — it is the exaggerated marketing wrapped around it. Several widely repeated claims have no scientific support, and it is worth naming them directly.
- “It detoxifies the body” / “pulls out toxins.” There is no evidence that swishing oil draws toxins, heavy metals, or systemic waste through the lining of the mouth. The body has organs for that job — the liver and kidneys. “Detox” here is a marketing word, not a measured effect.
- “It whitens teeth.” No good study shows oil pulling whitens teeth. Any impression of brightening is most likely from removing surface film, the same as a thorough rinse or brushing would do — not true whitening of the tooth.
- “It cures headaches, arthritis, asthma, diabetes, heart disease,” and other systemic illnesses. These claims trace back to popularized folk assertions, not to clinical trials. There is no reliable evidence that oil pulling treats any disease outside the mouth, and believing it does can be dangerous if it delays real treatment.
- “It replaces the dentist.” It does not. Oil pulling cannot repair a cavity, treat gum disease that has taken hold, or substitute for a professional cleaning.
Being skeptical of these claims is not being closed-minded — it is exactly the honesty the topic deserves. A gentle oral rinse is a modest thing; treating it as a cure-all does real harm by pulling people away from care that works.
The Real Safety Concern: Lipoid Pneumonia
For most healthy adults, swishing and spitting a food-grade oil is low-risk. But there is one genuine, documented harm that deserves respect: exogenous lipoid pneumonia. This is an inflammation of the lungs that can occur when oil droplets are accidentally breathed in (aspirated) instead of spat out. Because the practice involves holding a large amount of oil in the mouth for many minutes, sometimes while talking or moving around, small amounts can slip into the airway — especially if someone laughs, coughs, or is prone to swallowing problems.
This is not merely theoretical. Published case reports describe lipoid pneumonia in people who oil-pulled regularly, including cases linked to repeated sesame-oil pulling and a case of recurrent pneumonia tied to the habit. Lipoid pneumonia can cause cough, shortness of breath, and chest discomfort, and it can be slow to resolve.
Practical safety points:
- Never swish so aggressively or for so long that your throat or jaw is fatigued and control slips.
- Do not oil-pull while lying down, talking a lot, walking around, or distracted.
- Do not give oil pulling to young children, and avoid it in anyone with swallowing difficulties or a high risk of aspiration.
- If you develop a cough, wheeze, or shortness of breath after starting oil pulling, stop and see a doctor, and mention the practice specifically.
Other minor issues reported include jaw soreness from over-long swishing, upset stomach or diarrhea if oil is swallowed, and rarely allergic reactions to a particular oil.
Not a Substitute for the Basics
This point is important enough to stand on its own. Whatever oil pulling may or may not add, it must never take the place of the small set of habits that genuinely prevent tooth decay and gum disease:
- Brushing twice a day with fluoride toothpaste. Fluoride is one of the best-evidenced tools in all of medicine for preventing cavities. Nothing in oil pulling replaces it.
- Cleaning between the teeth daily with floss or interdental brushes, where a toothbrush cannot reach.
- Regular dental checkups and cleanings, which catch and treat problems oil pulling cannot touch.
- Limiting frequent sugary and acidic drinks and snacks, the true drivers of decay.
The danger is not that oil pulling is poison — it usually is not. The danger is that someone swaps a proven routine for an unproven one and quietly lets decay or gum disease advance. If oil pulling ever competes with brushing, flossing, or fluoride for your time and trust, the basics win every time.
How to Try It Safely as an Adjunct
If, after reading all of the above, you still want to try oil pulling — perhaps you simply like the fresh-mouth feeling — there is a reasonable, low-risk way to do it as an extra on top of real care, not instead of it.
- Keep the basics first. Brush twice daily with fluoride toothpaste, clean between your teeth, and keep your dental appointments. Oil pulling is the optional add-on, never the foundation.
- Choose a clean, food-grade oil you can tolerate — coconut, sesame, or sunflower are the usual choices.
- Use a modest amount, about a tablespoon, on an empty stomach in the morning if that suits your routine.
- Swish gently. A few minutes of relaxed swishing is plenty; there is no proven advantage to pushing toward 20 minutes, and longer sessions raise the risk of fatigue and accidental aspiration.
- Never swallow it. Spit the used oil into the trash or a paper towel — not the sink or toilet, to avoid clogged drains.
- Rinse, then brush and floss.
- Stop if anything feels wrong — a cough, breathlessness, jaw pain, stomach upset, or an allergic reaction — and speak with a professional.
Treated this way, oil pulling is a harmless little ritual for people who enjoy it. Just keep your expectations honest and your fluoride toothpaste closer.
The Honest Bottom Line
Oil pulling is an ancient practice with a small, shaky modern evidence base. At best, the research hints that swishing oil may slightly reduce plaque, gum inflammation, and cavity-linked bacteria — but the studies are small, short, and biased, and oil pulling has never been shown to outperform an ordinary antiseptic mouthwash, let alone brushing with fluoride. The popular claims that it “detoxes,” whitens teeth, or cures disease are not supported by evidence and should be set aside.
So the fair, non-promotional verdict is this: oil pulling is, at most, a harmless adjunct — not a substitute for the dental basics that actually work. If it appeals to you and you do it carefully, it is unlikely to hurt (with the real but rare exception of lipoid pneumonia if oil is inhaled). If you are choosing between oil pulling and brushing, flossing, fluoride, and seeing a dentist, choose the proven basics without hesitation.
Research Papers
- Asokan S, Rathan J, Muthu MS, et al. Effect of oil pulling on Streptococcus mutans count in plaque and saliva using Dentocult SM Strip mutans test: a randomized, controlled, triple-blind study. J Indian Soc Pedod Prev Dent. 2008;26(1):12–17. doi:10.4103/0970-4388.40315 — small triple-blind trial reporting a drop in cavity-linked bacteria after sesame-oil pulling.
- Asokan S, Emmadi P, Chamundeswari R. Effect of oil pulling on plaque induced gingivitis: a randomized, controlled, triple-blind study. Indian J Dent Res. 2009;20(1):47–51. doi:10.4103/0970-9290.49067 — reported reductions in plaque and gingivitis scores over two weeks, but in a small, high-risk-of-bias study.
- Asokan S, Rathinasamy TK, Inbamani N, et al. Mechanism of oil-pulling therapy — in vitro study. Indian J Dent Res. 2011;22(1):34–37. doi:10.4103/0970-9290.79971 — laboratory work exploring emulsification/saponification as a proposed mechanism; not clinical proof.
- Asokan S, Kumar RS, Emmadi P, et al. Effect of oil pulling on halitosis and microorganisms causing halitosis: a randomized controlled pilot trial. J Indian Soc Pedod Prev Dent. 2011;29(2):90–94. doi:10.4103/0970-4388.84678 — small pilot reporting reduced odor-causing microbes; preliminary only.
- Peedikayil FC, Sreenivasan P, Narayanan A. Effect of coconut oil in plaque related gingivitis — a preliminary report. Niger Med J. 2015;56(2):143–147. doi:10.4103/0300-1652.153406 — uncontrolled preliminary study of coconut-oil pulling showing decreased plaque and gingival indices.
- Peedikayil FC, Remy V, John S, et al. Comparison of antibacterial efficacy of coconut oil and chlorhexidine on Streptococcus mutans: an in vivo study. J Int Soc Prev Community Dent. 2016;6(5):447–452. doi:10.4103/2231-0762.192934 — found coconut oil and chlorhexidine both lowered bacterial counts, with chlorhexidine as the established comparator.
- Kaushik M, Reddy P, Sharma R, et al. The effect of coconut oil pulling on Streptococcus mutans count in saliva in comparison with chlorhexidine mouthwash. J Contemp Dent Pract. 2016;17(1):38–41. doi:10.5005/jp-journals-10024-1800 — oil pulling reduced salivary bacteria but was not shown superior to chlorhexidine.
- Sezgin Y, Memis Ozgul B, Alptekin NO. Efficacy of oil pulling therapy with coconut oil on four-day supragingival plaque growth: a randomized crossover clinical trial. Complement Ther Med. 2019;47:102193. doi:10.1016/j.ctim.2019.102193 — a more rigorous crossover design testing coconut-oil pulling against plaque regrowth.
- Sood P, Devi M A, Narang R, et al. Comparative efficacy of oil pulling and chlorhexidine on oral malodor: a randomized controlled trial. J Clin Diagn Res. 2014;8(11):ZC18–ZC21. doi:10.7860/JCDR/2014/9393.5112 — both oil pulling and chlorhexidine reduced bad breath, with chlorhexidine the standard comparison.
- Woolley J, Gibbons T, Patel K, et al. The effect of oil pulling with coconut oil to improve dental hygiene and oral health: a systematic review. Heliyon. 2020;6(8):e04789. doi:10.1016/j.heliyon.2020.e04789 — concluded the trials are at high risk of bias and do not provide reliable evidence of benefit.
- Kuroyama M, Kagawa H, Kitada S, et al. Exogenous lipoid pneumonia caused by repeated sesame oil pulling: a report of two cases. BMC Pulm Med. 2015;15:135. doi:10.1186/s12890-015-0134-8 — documents the real lung risk of aspirating oil during the practice.
- Kim JY, Jung JW, Choi JC, et al. Recurrent lipoid pneumonia associated with oil pulling. Int J Tuberc Lung Dis. 2014;18(2):251–252. doi:10.5588/ijtld.13.0852 — a case of recurrent pneumonia tied to oil pulling, underscoring the aspiration caution.
Connections
- Tooth Decay
- Gum Disease
- Canker Sores
- Ear, Nose & Throat Conditions
- Fasting
- Herbs
- All Remedies
- All Conditions