Ketogenic Diet
The ketogenic ("keto") diet is a very-low-carbohydrate, high-fat way of eating that forces the body to run on fat instead of sugar. It began as a medical treatment for epilepsy in the 1920s and remains a proven therapy for hard-to-control childhood seizures today. More recently it has drawn intense interest for type 2 diabetes and weight loss, where the evidence is promising but more limited. Many other popular claims — that keto boosts energy, prevents disease, or extends lifespan — are not well supported. This page lays out, honestly, where the science is strong, where it is still emerging, and where it simply isn't there yet.
Table of Contents
- What the Ketogenic Diet Is
- How It Works (Ketosis)
- The Strongest Evidence: Epilepsy
- Type 2 Diabetes & Weight
- Other Claims — Proven and Unproven
- What You Eat
- Risks, Side Effects & Who Should Avoid
- The Bottom Line
- Research Papers
- Connections
- Featured Videos
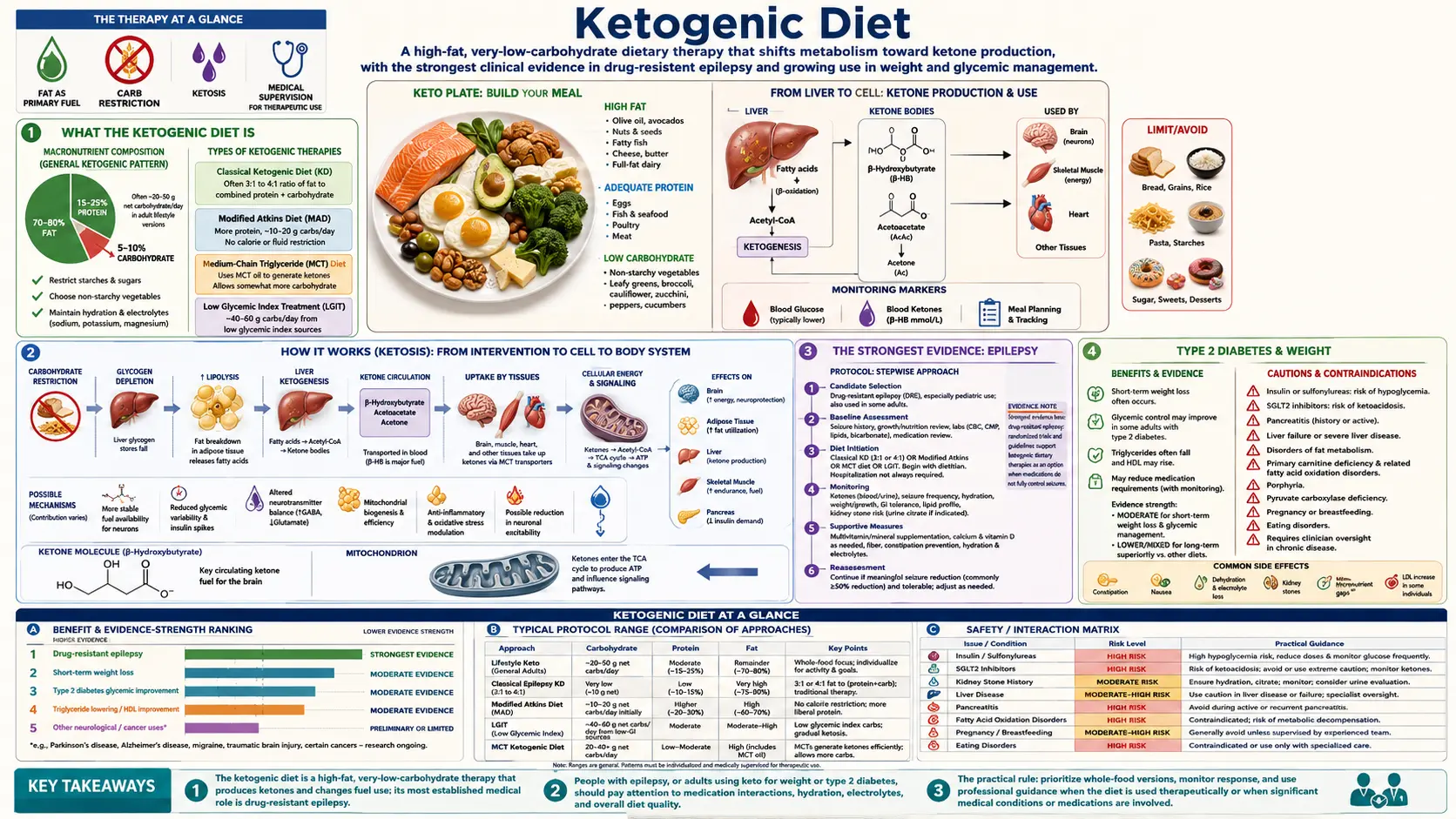
What the Ketogenic Diet Is
A ketogenic diet is built around three ideas: very few carbohydrates, plenty of fat, and a moderate amount of protein. Most versions keep total carbohydrates under about 50 grams a day — and stricter medical versions go lower, around 20-30 grams. To put that in perspective, a single bagel or a cup of rice can use up an entire day's carb budget.
When carbohydrates are cut this far, the body can no longer rely on its usual fuel — glucose (blood sugar) from carbs. Instead, the liver starts breaking down fat into compounds called ketone bodies, which most of the body and brain can burn for energy. This shift is called nutritional ketosis, and it is the whole point of the diet.
One important safety note up front: nutritional ketosis is not the same as diabetic ketoacidosis (DKA). DKA is a dangerous, sometimes life-threatening emergency in which ketones and blood sugar both climb to extreme levels, mostly in people with type 1 diabetes or, less often, type 2. In nutritional ketosis the body keeps ketones in a low, controlled range while blood sugar stays normal. The two share a word but are completely different situations — one is a chosen dietary state, the other is a medical crisis.
How It Works (Ketosis)
Normally your body prefers glucose. Eat a meal with bread, fruit, or pasta and your blood sugar rises, your body burns what it needs, and it stores the rest. When carbohydrates stay very low for a day or two, those glucose stores run down and the body needs another fuel source.
That is where the liver steps in. It converts fatty acids — both from the food you eat and from your own body fat — into ketone bodies. Ketones travel through the bloodstream to tissues that need energy, and crucially they can cross into the brain, which cannot burn fat directly. In effect, ketones become a "backup fuel" the brain can use when sugar is scarce.
Reaching ketosis usually takes two to four days of strict carbohydrate restriction. Becoming fully "fat-adapted" — feeling steady energy and physical performance on this fuel — can take several more weeks. The early transition is when many people feel worst (see Risks), because the body is still switching over.
The Strongest Evidence: Epilepsy
The clearest, best-established use of the ketogenic diet has nothing to do with weight loss. It is epilepsy. Doctors at the Mayo Clinic developed the diet in the 1920s specifically to reduce seizures, and after nearly a century it is still a recognized, evidence-based therapy — especially for children whose seizures are not controlled by medication (so-called drug-resistant or refractory epilepsy).
This is not a fringe or alternative claim. In a landmark randomized controlled trial, children placed on the ketogenic diet had a roughly 38% drop in seizures over three months, while a comparison group on usual care got slightly worse. A Cochrane systematic review — among the most rigorous types of evidence in medicine — concluded that ketogenic diets meaningfully reduce seizures in people with drug-resistant epilepsy.
The critical point for readers: medical ketogenic diets for epilepsy are prescribed and closely supervised by a specialist team, usually a neurologist and a dietitian, often starting in a hospital. They are far stricter than a casual "keto" eating plan and require careful monitoring. If seizures are the concern, this is a medical treatment to pursue with a doctor — not something to self-administer from the internet.
Type 2 Diabetes & Weight
Outside epilepsy, the most promising research is in type 2 diabetes. Because the diet keeps carbohydrate — and therefore blood sugar — low, it can directly lower glucose. Several studies show that low-carbohydrate and ketogenic approaches can reduce HbA1c (a three-month average of blood sugar), aid short-term weight loss, and let some people cut back on diabetes medications. A two-year study of a closely supported ketogenic program reported about a 1-point drop in HbA1c, roughly 10% weight loss, and large reductions in insulin and other drugs — though, importantly, it was not a randomized trial, so it can't fully separate the diet from the intensive coaching that came with it. A systematic review of randomized trials found that low-carbohydrate diets could put some people into diabetes remission at six months.
That is genuinely encouraging — but it comes with honest caveats:
- Adherence is hard. Many people struggle to stay this strict long-term, and benefits fade if the diet is abandoned. In that same body of research, the diabetes-remission advantage had largely diminished by twelve months.
- The weight-loss edge shrinks over time. Low-carb diets often win in the first few months, but head-to-head meta-analyses find that the difference versus other diets is small and narrows over a year or two — on the order of about one kilogram. The best diet for weight loss is largely the one a person can actually stick with.
- Long-term and heart outcomes are less certain. Short-term metabolic markers improve, but we have less high-quality evidence on hard long-term outcomes like heart attacks or lifespan.
One safety point matters enormously here: if you take diabetes or blood-pressure medication, do not start keto on your own. As blood sugar and blood pressure fall, your existing doses can become too strong, causing dangerously low blood sugar (hypoglycemia) or low blood pressure. This needs to be managed by a doctor who can adjust your medications as you go.
Other Claims — What's Proven and What Isn't
The ketogenic diet has been attached to a long list of health promises. It's worth separating what's backed by evidence from what's speculation.
Areas of legitimate research interest (not yet proven therapies)
- Certain neurological conditions. Beyond epilepsy, researchers are studying ketogenic diets in conditions such as migraine and some neurodegenerative diseases. This work is early and investigational — interesting, but not established treatment.
- Cancer (as an add-on, under study). Some laboratory and small clinical studies are exploring ketogenic diets alongside standard cancer treatment. To be clear: this is experimental and unproven. A ketogenic diet is not a cancer therapy and should never replace conventional treatment recommended by an oncologist.
Popular claims that are largely unproven
- Claims that keto reliably boosts energy, sharpens thinking for everyone, slows aging, or improves general health in healthy people are not well supported by strong human evidence.
- Individual people sometimes feel better, but personal stories are not the same as proof, and the early transition often makes people feel worse, not better.
In short: keto is a real medical tool for specific problems, not a cure-all. Be skeptical of anyone selling it as one.
What You Eat
A ketogenic diet reshapes the plate around fat and protein while cutting almost all starch and sugar.
Emphasized foods
- Non-starchy vegetables — leafy greens, broccoli, cauliflower, zucchini, peppers, asparagus
- Eggs and fish (including fatty fish like salmon and sardines)
- Meat and poultry
- Nuts and seeds
- Healthy fats — olive oil, avocado and avocado oil
- Some dairy and cheese, in moderation
Foods to avoid or strictly limit
- Grains and starches — bread, pasta, rice, cereal, oats
- Sugar and sweets — soda, candy, desserts, most packaged snacks
- Most fruit (small portions of berries are the usual exception)
- Starchy vegetables — potatoes, corn
- Most legumes — beans, lentils, chickpeas
Food quality matters — a lot. "Keto" is not automatically healthy. A diet built on vegetables, fish, olive oil, nuts, and avocado is very different from one built on processed meats, bacon, and butter. The first is sometimes called "clean" or whole-food keto; the second can be high in processed meat and saturated fat. If you try this way of eating, leaning toward whole foods and unsaturated fats is the more prudent choice.
Risks, Side Effects & Who Should Avoid
The ketogenic diet is a significant change, and it carries real downsides and risks.
Common side effects
- "Keto flu." In the first days to weeks, many people feel tired, headachy, irritable, foggy, or nauseated as the body adapts. It's usually temporary, and staying hydrated and replacing salt and other electrolytes often helps.
- Constipation and digestive changes, partly from cutting out fiber-rich grains, fruit, and legumes.
- Nutrient gaps. Eliminating whole food groups can shortchange fiber and certain vitamins and minerals.
- Cholesterol changes. Some people see a rise in LDL ("bad") cholesterol on keto — meta-analysis data confirm LDL can go up even as some other markers improve. Anyone on this diet long-term should have their blood lipids monitored by a doctor.
- Hard to sustain. The strictness leads many people to quit, and benefits tend to reverse if old eating patterns return.
Who should avoid it or only use it with expert care
- Type 1 diabetes — only under specialist supervision, because of the risk of ketoacidosis.
- Pancreatic, liver, or gallbladder disease — these organs are central to handling fat.
- Certain inherited metabolic disorders (for example, problems with fat metabolism) — keto can be dangerous.
- Pregnancy and breastfeeding.
- A history of eating disorders — the rigid rules can be harmful.
The bottom-line caution: talk to a doctor before starting, especially if you take any medication or have a chronic condition. This is doubly true for diabetes and blood-pressure drugs, where doses often need adjusting.
The Bottom Line
The ketogenic diet is two things at once. It is a legitimate, well-proven medical therapy for drug-resistant epilepsy, especially in children — used under specialist care. And it is a promising tool that can help certain people with type 2 diabetes lower blood sugar, lose weight in the short term, and reduce medications — but only with medical supervision, and with honest expectations that long-term adherence is hard and the advantage over other diets tends to shrink.
What it is not is a magic diet or a proven cure for everything. Claims about energy, longevity, and general wellness are largely unproven, and "keto" done with lots of processed meat is not a health food. If you're considering it, focus on whole-food quality, choose an approach you can sustain, and — especially if you have a medical condition or take medication — make the decision together with your doctor.
Research Papers
- Neal EG, Chaffe H, Schwartz RH, et al. The ketogenic diet for the treatment of childhood epilepsy: a randomised controlled trial. Lancet Neurology, 2008;7(6):500-506. doi:10.1016/S1474-4422(08)70092-9 — The pivotal randomized trial: children on the ketogenic diet had about a 38% reduction in seizures versus a slight increase in controls.
- Martin-McGill KJ, Bresnahan R, Levy RG, Cooper PN. Ketogenic diets for drug-resistant epilepsy. Cochrane Database of Systematic Reviews, 2020;(6):CD001903. doi:10.1002/14651858.CD001903.pub5 — A high-quality systematic review concluding ketogenic diets reduce seizures in drug-resistant epilepsy.
- Goldenberg JZ, Day A, Brinkworth GD, et al. Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission: systematic review and meta-analysis of published and unpublished randomized trial data. BMJ, 2021;372:m4743. doi:10.1136/bmj.m4743 — Low-carb diets achieved diabetes remission at 6 months, but the benefit largely faded by 12 months.
- Athinarayanan SJ, Adams RN, Hallberg SJ, et al. Long-term effects of a novel continuous remote care intervention including nutritional ketosis for the management of type 2 diabetes: a 2-year non-randomized clinical trial. Frontiers in Endocrinology, 2019;10:348. doi:10.3389/fendo.2019.00348 — A supervised 2-year ketogenic program lowered HbA1c and medication use; note it was non-randomized and paired with intensive coaching.
- Bueno NB, de Melo ISV, de Oliveira SL, da Rocha Ataide T. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials. British Journal of Nutrition, 2013;110(7):1178-1187. doi:10.1017/S0007114513000548 — Keto produced slightly more long-term weight loss (about 0.9 kg) but also raised LDL cholesterol; the practical difference was modest.
- Tobias DK, Chen M, Manson JE, Ludwig DS, Willett W, Hu FB. Effect of low-fat diet interventions versus other diet interventions on long-term weight change in adults: a systematic review and meta-analysis. Lancet Diabetes & Endocrinology, 2015;3(12):968-979. doi:10.1016/S2213-8587(15)00367-8 — Across many trials, differences in long-term weight loss between diet types were small, reinforcing that sustainability matters most.