GLP-1 Receptor Agonists: History and Origins
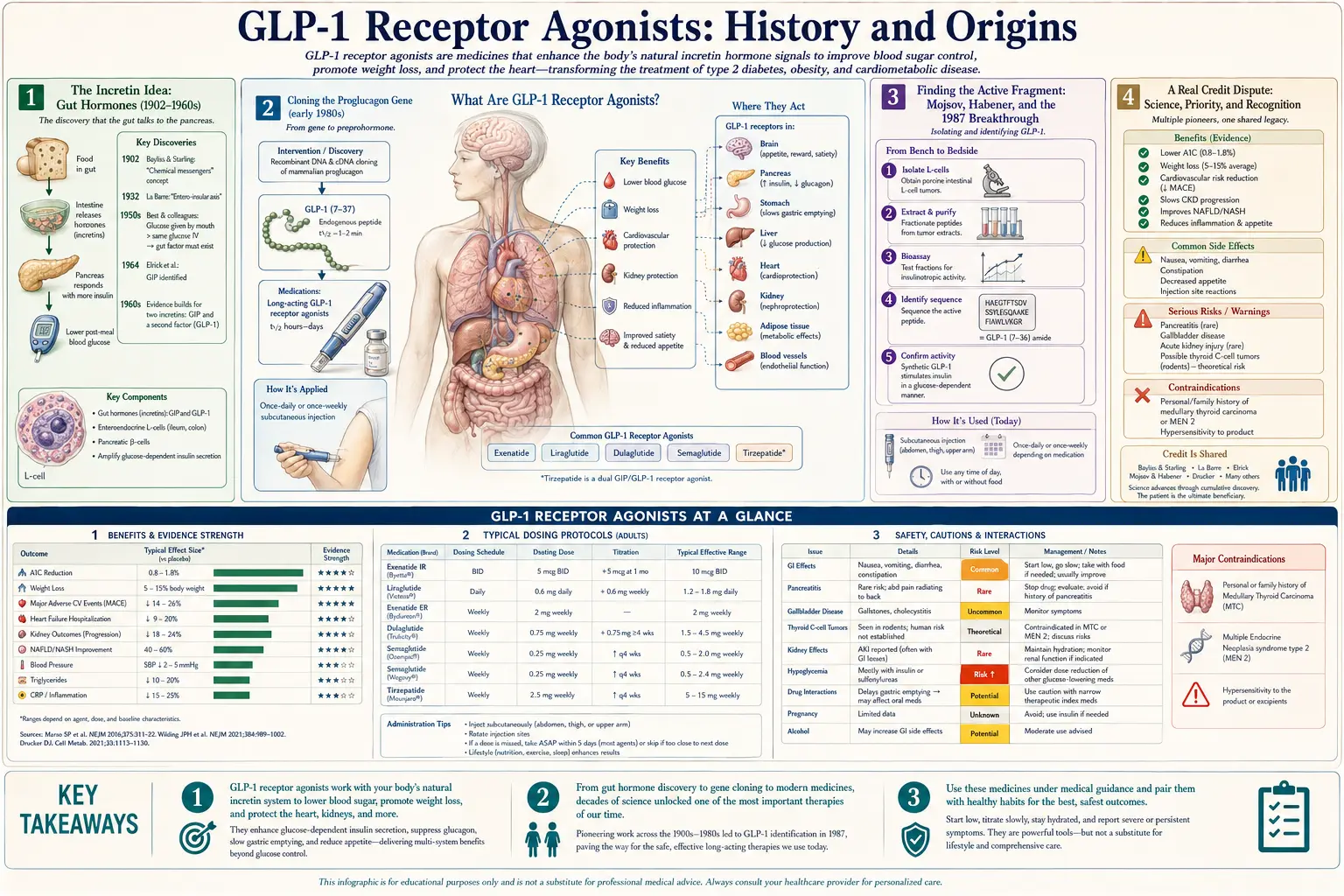
Unlike a folk remedy handed down through tradition, the GLP-1 receptor agonists have a documented, datable scientific origin — and not a single inventor, but a relay of named scientists working across four decades and several countries. The thread runs from the discovery of gut hormones at the start of the twentieth century, through the cloning of the proglucagon gene in the early 1980s, to the moment in 1986–1987 when Svetlana Mojsov, Joel Habener, and their colleagues pinned down the small active fragment of GLP-1 and proved it triggers insulin; through a venomous desert lizard whose saliva yielded the first usable drug; to the Danish chemists who engineered semaglutide into a once-weekly injection. This article tells that real story — who did what and when — and is honest about a genuine credit dispute along the way, and about what the evidence does and does not yet show. Where the record is firm we say so; where a question is still argued, we name it as such.
Interactive Visualization Hunger, Leptin & Why Diets Fight Back Watch the hunger neurons and the fullness neurons fight it out — then lose weight and see leptin fall, hunger climb and metabolism drop. It isn’t willpower. It’s a defended system. Launch →
Table of Contents
- The Incretin Idea: Gut Hormones (1902–1960s)
- Cloning the Proglucagon Gene (early 1980s)
- Finding the Active Fragment: Mojsov, Habener, and the 1987 Breakthrough
- A Real Credit Dispute
- From Gila Monster Venom to the First Drug (1990–2005)
- Engineering a Better Molecule: Liraglutide and Semaglutide
- The Dual Agonist: Tirzepatide and What Came Next
- Evidence, Reception, and Honest Limits
- Research Papers and References
- Connections
- Featured Videos
The Incretin Idea: Gut Hormones (1902–1960s)
The GLP-1 story begins long before anyone had heard of GLP-1, with a simple and then-radical idea: that the gut talks to the rest of the body using chemical messengers. In 1902 the English physiologists William Bayliss and Ernest Starling identified secretin, the first hormone ever described — a substance released by the intestine that signals the pancreas. Their work helped found the entire concept of a hormone (a word Starling popularised).
Out of this grew a specific puzzle that turned out to be the key to everything that follows. Researchers noticed that glucose taken by mouth triggers far more insulin than the same amount of glucose given intravenously. Something in the gut, released when food arrives, was amplifying the insulin response. In 1932 the Belgian physiologist Jean La Barre coined the term incrétine (incretin) for this hypothesised gut factor. The hunt for the incretins — the gut hormones that prime the pancreas after a meal — would occupy physiologists for the rest of the century. GLP-1 would eventually prove to be one of the two most important of them.
Cloning the Proglucagon Gene (early 1980s)
The modern chapter opens with molecular biology. In the early 1980s, work on the gene that codes for the hormone glucagon revealed that this single gene — proglucagon — encodes not just glucagon but several other peptides hidden within the same precursor protein. Two of these newly revealed sequences were named glucagon-like peptide-1 (GLP-1) and glucagon-like peptide-2 (GLP-2), so called because they resembled glucagon.
The cloning was achieved by more than one group working in parallel. The endocrinologist Joel Habener at Massachusetts General Hospital and Harvard isolated proglucagon-coding DNA (his early work used anglerfish pancreatic islets, then mammalian tissue), and the geneticist Graeme Bell and colleagues independently reported the human proglucagon gene sequence in 1983. Knowing the sequence was a beginning, not an answer: it revealed that GLP-1 existed as a possible peptide, but not what biological job — if any — it actually did, nor which exact piece of it was active. Answering that required the next, crucial step.
Finding the Active Fragment: Mojsov, Habener, and the 1987 Breakthrough
This is the pivotal episode in the whole history, and it centres on a chemist named Svetlana Mojsov. Born in Skopje (in what was then Yugoslavia, now North Macedonia) on 8 December 1947, Mojsov studied physical chemistry in Belgrade and earned her PhD at Rockefeller University in 1978, training in the laboratory of Nobel laureate Bruce Merrifield — the inventor of solid-phase peptide synthesis, the technique for building peptides chemically. That expertise made her uniquely equipped for the problem at hand.
The problem was this: the proglucagon gene predicted a GLP-1 peptide, but the full-length version made in the lab barely worked. Working at Massachusetts General Hospital in the mid-1980s, Mojsov reasoned that the body must trim the peptide to a shorter, active form. Using sequencing and antibodies she generated herself, she identified the truncated fragment — known as GLP-1(7-37) — as the biologically active form actually present in the intestine. Then came the proof. In a landmark 1987 paper in the Journal of Clinical Investigation, Mojsov, together with Gordon Weir and Joel Habener, showed that this short fragment was a remarkably potent stimulator of insulin release in the perfused rat pancreas — powerfully boosting insulin at physiological concentrations. They had found a true incretin: the long-sought gut hormone that primes the pancreas after eating.
Several scientists deserve named credit for converging on this discovery. Daniel Drucker, who joined Habener's laboratory as a postdoctoral fellow in 1984, performed seminal experiments characterising the proglucagon-derived peptides and how the gut and pancreas process them differently (he later identified GLP-2 as an intestinal growth factor). In Denmark, the physiologist Jens Juul Holst independently established that GLP-1 is generated in the gut and demonstrated its effects on insulin secretion — and, later, on appetite — in human beings. The picture that emerged from these groups in the late 1980s and 1990s was the foundation every later drug was built on: GLP-1 lowers blood sugar in a glucose-dependent way (so it rarely causes hypoglycaemia on its own), slows the stomach, and signals fullness to the brain.
A Real Credit Dispute
Honesty about this history requires telling an uncomfortable part of it. For decades, Svetlana Mojsov's central role was largely written out of the popular account, and even out of some of the paperwork. Patents covering GLP-1 work she had contributed to were filed with Joel Habener named as the sole inventor; Mojsov had to fight to correct the record. By her account — and as later reported when the field's pioneers began winning major prizes — Massachusetts General Hospital eventually agreed to amend four patents to add her name, and she received her one-third share of the associated royalties, though for a limited period.
The correction came late but it did come. As GLP-1 drugs reshaped medicine, recognition finally caught up with the science: Mojsov received the VinFuture Prize (2023), shared the Lasker–DeBakey Clinical Medical Research Award in 2024 (with Habener and Lotte Bjerre Knudsen), was named to the Time 100 in 2024, and shared the Breakthrough Prize in Life Sciences (2025), among other honours. We include this episode not to assign blame but because the site's purpose is truth over tidy storytelling: the discovery of GLP-1's active form was a collaborative achievement, and a woman chemist's foundational contribution to one of the most important drug classes of the century was for a long time under-credited.
From Gila Monster Venom to the First Drug (1990–2005)
Knowing GLP-1's biology did not immediately yield a drug, because native GLP-1 is destroyed within about a minute or two in the bloodstream by an enzyme (DPP-4). A medicine needed a molecule that hit the same receptor but survived far longer — and the first such molecule came from one of the most unlikely sources in pharmacology: the venom of a desert lizard.
In the early 1990s, an endocrinologist named John Eng, working at the Veterans Affairs Medical Center in the Bronx, New York, was studying gut peptides using an assay he had developed. He became intrigued by reports that the Gila monster (Heloderma suspectum), a venomous lizard of the American southwest, could go long stretches without eating yet keep its blood sugar and gut tissue healthy. Eng ordered preserved venom samples and, in a paper published in the Journal of Biological Chemistry in 1992, reported the isolation of a 39-amino-acid peptide he named exendin-4. It closely resembled human GLP-1 in structure and action — but, crucially, it resisted rapid breakdown, giving it a useful half-life of a few hours rather than minutes.
Eng's path to a drug shows how contingent these stories are. The VA did not pursue a patent, so Eng patented exendin-4 himself, and famously took a booth at an American Diabetes Association meeting to find a partner. The small biotechnology firm Amylin Pharmaceuticals (later with Eli Lilly) took it up and developed a synthetic version, exenatide. Marketed as Byetta, it became the first GLP-1 receptor agonist approved for type 2 diabetes when the U.S. FDA cleared it on 28 April 2005. For his discovery, Eng was later honoured with the Golden Goose Award, which celebrates obscure federally funded research that yields huge payoffs. A twice-daily injection by today's standards, exenatide nonetheless proved the principle that a long-acting GLP-1 mimic could safely lower blood sugar and modestly reduce weight in people.
Engineering a Better Molecule: Liraglutide and Semaglutide
The leap from a workable drug to a transformational one came largely from the Danish company Novo Nordisk and a chemist named Lotte Bjerre Knudsen (born 10 March 1964). Rather than borrow a peptide from a lizard, her team set out to re-engineer human GLP-1 itself so it would last far longer in the body. Their key trick was to attach a fatty-acid chain that lets the drug bind reversibly to albumin, the most abundant protein in blood, which acts as a slow-release reservoir and shields the peptide from rapid degradation.
The first product of this approach was liraglutide, developed at Novo Nordisk in the late 1990s under Knudsen's leadership. After more than a decade of trials it reached the market as a once-daily injection: approved for type 2 diabetes (brand name Victoza) by the FDA on 25 January 2010, and later, at a higher dose, for chronic weight management (brand name Saxenda) on 23 December 2014 — an early, formal acknowledgement that this drug class could treat obesity, not only diabetes.
Knudsen's team, with chemists including Jesper Lau and Thomas Kruse, then refined the molecule further into semaglutide, with even stronger albumin binding and greater stability — enough to make it a once-weekly injection. Semaglutide for type 2 diabetes (Ozempic) was approved in the United States in 2017; an oral daily tablet form (Rybelsus) followed; and in June 2021 a higher-dose version (Wegovy) was approved specifically for chronic weight management, producing average weight loss of roughly 15% of body weight in its pivotal trials — results previously seen only with surgery. It was Wegovy, more than any earlier drug, that turned GLP-1 medicines into a global cultural phenomenon. For her work, Knudsen shared the 2024 Lasker Award with Mojsov and Habener.
The Dual Agonist: Tirzepatide and What Came Next
The most recent chapter belongs to Eli Lilly and a molecule that targets two gut hormones at once. Tirzepatide activates not only the GLP-1 receptor but also the receptor for GIP (glucose-dependent insulinotropic polypeptide), the other major incretin whose existence traced back to the same decades-long incretin hunt. This dual mechanism produced even larger effects in trials than single-target GLP-1 drugs.
Tirzepatide was approved by the FDA for type 2 diabetes under the brand name Mounjaro on 13 May 2022, and for chronic weight management under the name Zepbound in November 2023; in 2024 Zepbound also became the first drug approved for obstructive sleep apnoea in adults with obesity. In its pivotal obesity trial (SURMOUNT-1), the highest dose produced average weight loss of roughly one-fifth of body weight. Research has continued to accelerate: triple-hormone agonists such as retatrutide (adding the glucagon receptor) and combination products are in late-stage testing, and the field that began with a lizard's saliva and a contested patent now anchors one of the largest areas of pharmaceutical development in the world.
Evidence, Reception, and Honest Limits
It is worth being clear about how this history sits with the evidence, because GLP-1 drugs differ from many remedies on this site: their core approved uses are strongly supported by large, randomised clinical trials and they are mainstream, regulator-approved medicines, not fringe or unproven products. The landmark SELECT trial (2023) showed semaglutide cut major cardiovascular events by about 20% in people with overweight or obesity and established heart disease but without diabetes; the STEP (semaglutide) and SURMOUNT (tirzepatide) programmes documented the weight-loss results above. This is a genuinely well-evidenced drug class for blood-sugar control, weight management, and cardiovascular risk reduction.
That said, honesty cuts both ways, and several real limits and cautions belong in any fair history. The drugs commonly cause gastrointestinal side effects (nausea, vomiting, constipation), carry a boxed warning related to thyroid C-cell tumours seen in rodents (they are contraindicated in people with medullary thyroid cancer or MEN2), and can be associated with gallbladder problems and, rarely, pancreatitis. A large share of the weight lost is lean tissue, including muscle, unless resistance training and adequate protein are maintained; and weight is typically regained after stopping, because they treat appetite biology rather than curing it — for many people they are long-term therapy. Their use for neurological and addiction conditions (Parkinson's, Alzheimer's, alcohol use disorder) is genuinely promising but still investigational and not approved; the popular framing of certain supplements as a "natural Ozempic" is marketing, not equivalence. And the long-term effects over decades of use, along with the cost and access questions these expensive drugs raise, remain unsettled. The detailed evidence, dosing, and cautions are covered on the main GLP-1 Receptor Agonists page and in the companion Benefits articles; this page is concerned with how the class came to exist.
Research Papers and References
The list below combines key peer-reviewed primary papers and reviews tracing the discovery and development of GLP-1 receptor agonists with curated PubMed topic-search links. Author names, titles, and journals are given as plain text; only the stable DOI, PMID, or archive link is hyperlinked, and each opens in a new tab. Historical events such as the 1902 discovery of secretin and the 1932 coining of "incretin" are described in the article as historical facts rather than cited to a modern source.
- Mojsov S, Weir GC, Habener JF. Insulinotropin: glucagon-like peptide I (7-37) co-encoded in the glucagon gene is a potent stimulator of insulin release in the perfused rat pancreas. Journal of Clinical Investigation. 1987;79(2):616-619. — doi:10.1172/JCI112855 · PMID: 3543057
- Eng J, Kleinman WA, Singh L, Singh G, Raufman JP. Isolation and characterization of exendin-4, an exendin-3 analogue, from Heloderma suspectum venom. Journal of Biological Chemistry. 1992;267(11):7402-7405. — PMID: 1313797
- Drucker DJ, Habener JF, Holst JJ. Discovery, characterization, and clinical development of the glucagon-like peptides. Journal of Clinical Investigation. 2017;127(12):4217-4227. — doi:10.1172/JCI97233
- Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metabolism. 2018;27(4):740-756. — doi:10.1016/j.cmet.2018.03.001
- Lane MA. Joel Habener, Svetlana Mojsov, and Lotte Bjerre Knudsen awarded Lasker prize for pioneering work on GLP-1. Journal of Clinical Investigation. 2024;134(19):e186225. — doi:10.1172/JCI186225
- Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity (STEP 1). New England Journal of Medicine. 2021;384(11):989-1002. — doi:10.1056/NEJMoa2032183 · PMID: 33567185
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1). New England Journal of Medicine. 2022;387(3):205-216. — doi:10.1056/NEJMoa2206038
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes (SELECT). New England Journal of Medicine. 2023;389(24):2221-2232. — doi:10.1056/NEJMoa2307563
- GLP-1 receptor agonists — history and discovery — PubMed: GLP-1 receptor agonist history and discovery
- Exendin-4 and exenatide development — PubMed: exendin-4 and exenatide
External Authoritative Resources
- Lasker Foundation — GLP-1-based therapy for obesity (2024 award)
- National Institute on Aging — Exendin-4: from lizard to laboratory
- PubMed — All research on GLP-1 receptor agonists
Connections
- All Remedies
- Hunger, Leptin & Why Diets Fight Back — interactive animation
- GLP-1 Receptor Agonists
- GLP-1 Receptor Agonists Benefits
- Berberine
- Blood Sugar
- Fasting
- Diabetes
- Obesity