CEA Test: Carcinoembryonic Antigen Lab Guide
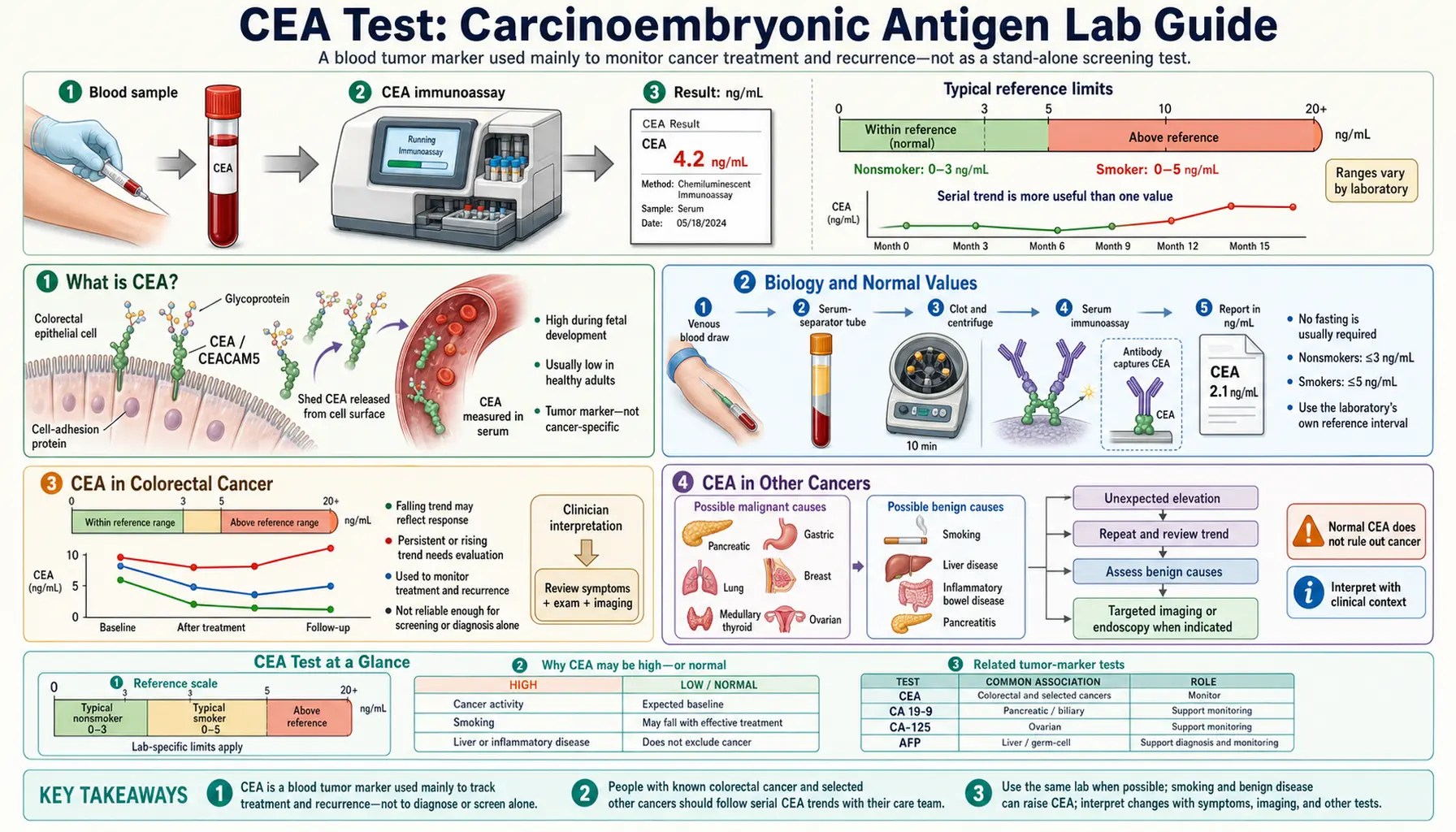
Table of Contents
- What is CEA?
- Biology and Normal Values
- CEA in Colorectal Cancer
- CEA in Other Cancers
- Benign Causes of CEA Elevation
- Pre-Operative CEA as a Prognostic Marker
- Post-Resection CEA Monitoring Protocol
- Interpretation Pitfalls
- Key Research Papers
- Connections
- Featured Videos
What is CEA?
Carcinoembryonic antigen (CEA) is a heavily glycosylated cell adhesion molecule — a GPI-anchored membrane protein in the immunoglobulin superfamily — encoded by the CEACAM5 gene on chromosome 19q. It was first described by Gold and Freedman in 1965 from human colon cancer tissue, where they observed an antigen expressed at high levels in fetal gastrointestinal epithelium and in colorectal carcinoma but largely absent from normal adult tissue.
In healthy adults, CEA expression is very low and confined mainly to colonic mucosal cells. Most CEA produced in the gut is shed into bile rather than entering systemic circulation, which explains why blood levels remain low under normal conditions. When colonic epithelium undergoes malignant transformation, CEA production increases dramatically and the protein leaks into the bloodstream.
- Normal serum CEA: <5 ng/mL in non-smokers; <10 ng/mL in active smokers
- Primary clinical role: monitoring colorectal cancer (CRC) after surgical resection for recurrence — not useful as a general screening test (very poor sensitivity and specificity for early-stage CRC)
- Pre-treatment prognosis: elevated pre-operative CEA is an independent poor prognostic marker in Stage II–III CRC
- Secondary monitoring roles: pancreatic cancer, gastric cancer, lung adenocarcinoma, and breast cancer to varying degrees
Biology and Normal Values
CEA belongs to the carcinoembryonic antigen-related cell adhesion molecule (CEACAM) family, which comprises 19 members. CEACAM5 is the classic "CEA" measured in clinical practice. Its molecular weight is approximately 180–200 kDa, with significant variability due to extensive glycosylation — roughly 50% of the molecule's mass is carbohydrate.
CEA has a circulating half-life of approximately 7 days. This is clinically important: after complete tumor resection (R0 resection), serum CEA should normalize within 4–6 weeks. Failure to normalize is a red flag for occult residual disease or micrometastatic deposits. CEA is cleared primarily by Kupffer cells in the liver, with hepatic extraction accounting for approximately 70% of clearance. Any significant liver disease therefore impairs CEA clearance and elevates levels independently of cancer.
Reference Ranges
- Non-smokers: <5 ng/mL (most laboratory reference ranges)
- Active smokers: up to <10 ng/mL (smoking upregulates colonic CEACAM5 expression 2–3 fold)
- Mild elevation (5–10 ng/mL): non-specific; common in smokers, liver disease, IBD, and COPD
- Moderate elevation (10–100 ng/mL): concerning for malignancy, particularly in non-smokers
- High elevation (>100 ng/mL): strongly suggests metastatic cancer — most commonly CRC, pancreatic, gastric, or lung adenocarcinoma
- Very high (>1000 ng/mL): often indicates widespread metastatic disease; CRC with extensive liver metastases is a common cause
CEA in Colorectal Cancer
CEA is most valuable in the management of colorectal cancer (CRC), where it is recommended by both the American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Network (NCCN) for post-resection surveillance in Stage II–IV patients.
Pre-Treatment Role
A CEA drawn before surgery (pre-operative CEA) serves as both a baseline and a prognostic marker. An elevated pre-op CEA (>5 ng/mL) is an independent poor prognostic factor in Stage II–III CRC and is included in several staging nomograms. Stage II colon cancer patients with elevated pre-operative CEA have recurrence rates closer to Stage III, which has prompted some clinicians to recommend adjuvant chemotherapy consideration in this subgroup.
Post-Resection Monitoring
After curative-intent (R0) resection, CEA is monitored serially on the following schedule per NCCN/ASCO guidelines:
- Years 1–3: every 3–6 months
- Years 4–5: every 6 months
- After 5 years: routine CEA monitoring is generally discontinued (recurrence risk falls to background)
Post-resection CEA normalization should occur within 4–6 weeks. Failure to normalize after R0 resection suggests occult residual disease. A rising CEA on surveillance — defined as serial increase over two or more consecutive measurements, or a single value >10 ng/mL above the post-operative nadir — triggers CT of chest, abdomen, and pelvis.
Performance Characteristics
- Sensitivity for CRC recurrence: 58–80% depending on site (best for liver metastases; lower for local pelvic recurrence)
- Specificity: approximately 82–90%
- Lead time: rising CEA may precede imaging-detectable recurrence by 4–6 months, enabling earlier intervention in potentially resectable disease
Chemotherapy Monitoring and CEA Flare
During systemic chemotherapy (oxaliplatin-based regimens such as FOLFOX or FOLFIRI), CEA can temporarily rise during the first 8–12 weeks before falling in response to effective therapy — the so-called CEA flare phenomenon. Clinicians should not prematurely stop therapy based on this early transient rise; confirm disease status with CT before changing treatment. Persistent rising CEA beyond this window is more likely true progression.
In patients with CRC liver metastases, very high CEA levels (>1000 ng/mL) correlate with heavy hepatic tumor burden, partly because the liver's capacity to clear CEA is overwhelmed by tumor replacement of functional hepatic parenchyma.
CEA in Other Cancers
While CEA is most closely associated with colorectal cancer, it is elevated across a range of other malignancies and plays a secondary monitoring role in several of them.
Pancreatic Cancer
CEA is elevated in approximately 60–80% of pancreatic ductal adenocarcinoma (PDAC). It is most useful in combination with CA 19-9: when both CEA >5 ng/mL and CA 19-9 >37 U/mL are present together, diagnostic specificity for PDAC increases substantially compared to either marker alone.
Gastric Cancer
CEA is elevated in roughly 30–50% of gastric cancers. Asian oncology guidelines (JGCA — Japanese Gastric Cancer Association) recommend using CEA for post-resection monitoring alongside CA 72-4 and CA 19-9 in a complementary panel, since no single marker is sufficiently sensitive for gastric cancer alone.
Lung Adenocarcinoma
CEA is elevated in approximately 40–60% of lung adenocarcinomas, making it a useful monitoring marker in this histologic subtype. It is generally not elevated in squamous cell carcinoma or small cell lung cancer. EGFR-mutant lung adenocarcinomas tend to have higher baseline CEA levels, and CEA can be followed during targeted therapy as a complement to imaging.
Breast Cancer
CEA is elevated in approximately 30–40% of breast cancers. It is less sensitive for breast cancer monitoring than CA 15-3 or CA 27.29, but is sometimes used as an adjunct marker in metastatic breast cancer when the more specific markers are not informative.
Medullary Thyroid Cancer
In medullary thyroid cancer (MTC), CEA and calcitonin are used together. Calcitonin is the primary marker; CEA becomes relevant when MTC dedifferentiates or behaves more aggressively — rising CEA with stable calcitonin can signal histologic dedifferentiation and worsening prognosis.
What CEA Cannot Do
CEA is not a useful screening test for colorectal cancer or any other cancer in the general asymptomatic population. Sensitivity for Stage I CRC is only 30–40%. Elevated CEA warrants investigation only in the appropriate clinical context — not as a routine population screen.
Benign Causes of CEA Elevation
A mildly elevated CEA does not automatically indicate malignancy. A number of common benign conditions raise serum CEA, sometimes into ranges that overlap with early cancer. Interpreting CEA always requires clinical context.
- Smoking: the most common non-malignant cause of CEA elevation. Active smokers can have CEA 2–3 times normal due to direct mucosal CEACAM5 upregulation. CEA typically normalizes 6–12 weeks after smoking cessation.
- Liver disease: cirrhosis, alcoholic hepatitis, and chronic viral hepatitis impair hepatic CEA clearance by reducing functional Kupffer cell mass. CEA can reach 10–50 ng/mL in severe cirrhosis without any malignancy present.
- Inflammatory bowel disease (IBD): both Crohn's disease and ulcerative colitis in active phases increase CEA, typically to 5–15 ng/mL. Always interpret CEA in the context of IBD disease activity and treatment response.
- COPD and emphysema: mild CEA elevation (5–15 ng/mL) is common in COPD; the mechanism is not fully understood. The key feature is a stable, non-progressively rising CEA.
- Pancreatitis: both acute and chronic pancreatitis can produce transient or persistent mild-to-moderate CEA elevation. The overlap with pancreatic cancer CEA values is a genuine diagnostic challenge.
- Hypothyroidism: mild CEA elevation that resolves with adequate thyroid hormone replacement.
- Renal failure: impaired non-hepatic clearance in chronic kidney disease can raise CEA 2–4 times above normal.
- Other GI inflammation: peptic ulcer disease and diverticulitis cause minimal CEA elevation; these are generally not clinically significant.
Key principle: a mildly elevated CEA in isolation does not require an aggressive cancer workup if the clinical context suggests a benign cause. Confirm it is stable or declining over 3–6 months with serial measurements before escalating investigation.
Pre-Operative CEA as a Prognostic Marker
Pre-operative CEA level has been validated as an independent prognostic marker in colorectal cancer across multiple large randomized controlled trials, including NSABP C-07, MOSAIC, and PETACC-3. These landmark adjuvant chemotherapy trials consistently show that patients with elevated pre-operative CEA (>5 ng/mL) have significantly worse disease-free and overall survival than those with normal CEA, independent of TNM stage.
Stage II Implications
Stage II colon cancer patients with elevated pre-operative CEA have recurrence rates and outcomes that resemble Stage III disease. Several national guidelines and multidisciplinary consensus statements now consider elevated pre-operative CEA a high-risk feature in Stage II CRC that should prompt consideration of adjuvant chemotherapy — a decision ordinarily reserved for Stage III and higher.
Stage III: IDEA Collaboration
The IDEA (International Duration Evaluation of Adjuvant Chemotherapy) collaboration, a pooled analysis of six phase III trials, used pre-operative CEA as a stratification variable. Elevated baseline CEA was associated with significantly higher recurrence risk among Stage III CRC patients, reinforcing its use as an independent prognostic variable beyond TNM staging.
Rectal Cancer and Neoadjuvant Therapy
In locally advanced rectal cancer, the baseline CEA level before neoadjuvant chemoradiation predicts pathologic complete response (pCR). Patients with low baseline CEA levels at diagnosis have higher pCR rates after chemoradiation, with implications for watch-and-wait strategies and sphincter preservation.
Stage IV at Presentation
Patients presenting with Stage IV CRC and CEA >200 ng/mL at diagnosis rarely achieve CEA normalization with systemic chemotherapy alone. Very high CEA at diagnosis correlates with greater metastatic tumor burden and is associated with shorter progression-free and overall survival in metastatic CRC.
Post-Resection CEA Monitoring Protocol
ASCO and NCCN guidelines recommend serial CEA monitoring for patients with Stage II–IV CRC who have undergone curative-intent resection. The goal is early detection of recurrence at a stage when salvage surgery (re-resection of isolated liver or lung metastases) may still be possible.
Monitoring Schedule
- Years 1–3: CEA every 3–6 months
- Years 4–5: CEA every 6 months
- After 5 years: routine CEA surveillance is generally stopped; recurrence risk falls to near-background at this point
Triggers for Further Evaluation
- Any single CEA >10 ng/mL above post-operative nadir
- Serial rise of >30% over two consecutive measurements
- Action: CT of chest, abdomen, and pelvis
CEA Flare During Chemotherapy
A transient CEA rise (usually <30%) during the first 8–12 weeks of oxaliplatin-based chemotherapy is a recognized phenomenon. Clinicians should not prematurely stop effective therapy based on this early signal — confirm disease status with CT imaging before acting. If CEA continues to rise beyond 12 weeks, this is more consistent with true disease progression.
CEA Rise With Negative CT
When CEA is rising but CT is negative or equivocal, PET/CT is the preferred next step. PET/CT detects recurrence in approximately 50% of patients with a rising CEA and a negative or inconclusive CT. If PET/CT is also negative, repeat CEA in 4–6 weeks; if still rising, proceed with multidisciplinary tumor board review.
FACS Trial Evidence
The UK FACS (Follow-up After Colorectal Surgery) trial demonstrated that CEA-triggered CT surveillance detected more resectable recurrences compared to detection by symptoms alone. While the trial was not powered to show a definitive overall survival benefit, the data support the practice of regular CEA surveillance as a means of identifying salvageable recurrences earlier in the natural history of disease.
Interpretation Pitfalls
CEA is a powerful tool when used correctly, but it is also one of the most commonly misinterpreted tumor markers in clinical practice. Avoiding the following errors will improve the clinical utility of the test.
- CEA is not a screening test. Sensitivity for Stage I CRC is only 30–40%. Do not use a CEA level to evaluate colorectal cancer risk in asymptomatic patients — use colonoscopy. An elevated CEA in an asymptomatic person does not have sufficient positive predictive value to justify colonoscopy as a direct consequence of the CEA alone.
- CEA-negative cancers. Fibrolamellar hepatocellular carcinoma, pure squamous cell carcinomas, and most ovarian and uterine cancers do not reliably elevate CEA. Absence of CEA elevation does not rule out malignancy in these tumor types.
- Liver disease plus colon cancer. In a patient with both cirrhosis and CRC, very high CEA may be partly attributable to impaired hepatic clearance and not solely to tumor burden. Use CT imaging and the trend over time — not the absolute CEA value alone — to guide decisions.
- Smoking status must always be documented. A CEA of 7 ng/mL in a 40-year-old non-smoker warrants clinical investigation; in a heavy smoker it may represent their baseline. Always record smoking status and, if possible, obtain a pre-cessation baseline.
- Prognostic vs. diagnostic distinction. An elevated pre-operative CEA indicates worse prognosis but does not change TNM staging. Do not "upstage" a patient's cancer based on CEA alone — it is a prognostic modifier, not a staging criterion.
- Avoid aggressive workup for isolated mild elevation. Never pursue invasive investigation for an isolated mildly elevated CEA without supporting clinical findings. Serial measurements and clinical context are essential. A stable CEA of 7 ng/mL in a non-smoker with known liver disease is very different from a CEA that has risen from 5 to 12 to 23 ng/mL over three consecutive measurements.
- Post-hepatic resection for CRC metastases. In patients who have had hepatic resection for CRC liver mets, rising CEA may reflect a combination of regenerating liver parenchyma producing more CEA and residual or recurrent tumor. PET/CT is the most useful modality in this clinically ambiguous setting.
Key Research Papers
- Gold P, Freedman SO. Demonstration of tumor-specific antigens in human colonic carcinomas by immunological tolerance and absorption techniques. J Exp Med. 1965. — Search PubMed
- Duffy MJ. Carcinoembryonic antigen as a marker for colorectal cancer: is it clinically useful? Clin Chem. 2001. — Search PubMed
- Goldstein MJ, Mitchell EP. Carcinoembryonic antigen in the staging and follow-up of patients with colorectal cancer. Cancer Invest. 2005. — Search PubMed
- Locker GY et al. ASCO 2006 update of recommendations for the use of tumor markers in gastrointestinal cancer. J Clin Oncol. 2006. — Search PubMed
- Moertel CG et al. An evaluation of the carcinoembryonic antigen (CEA) test for monitoring patients with resected colon cancer. JAMA. 1993. PMID 18316791
- Primrose JN et al. Effect of 3 to 5 years of scheduled CEA and CT follow-up to detect recurrence of colorectal cancer: the FACS randomized clinical trial. JAMA. 2014. PMID 26033813
- Filella X et al. CEA as a prognostic factor in patients with pancreatic cancer. Anticancer Res. 1994. — Search PubMed
- Peng WJ et al. Serum CEA levels in lung adenocarcinoma: association with clinicopathological features and prognosis. Cancer Biomark. 2011. — Search PubMed
- Yiu HH et al. Smoking and carcinoembryonic antigen levels. Ann Clin Biochem. 2008. — Search PubMed
- Thirunavukarasu P et al. Stage III colon cancers with elevated preoperative carcinoembryonic antigen level: a case for adjuvant chemotherapy. Ann Surg Oncol. 2011. — Search PubMed
- Tie J et al. Circulating tumor DNA analysis detects minimal residual disease and predicts recurrence in patients with stage II colon cancer. Sci Transl Med. 2016. — Search PubMed
- Labianca R et al. Colon cancer. Crit Rev Oncol Hematol. 2010. CEA pre-op prognosis Stage III CRC. — Search PubMed
Connections
- All Lab Tests
- AFP Test
- CA-125 Test
- PSA Test
- Comprehensive Metabolic Panel
- Complete Blood Count
- Colorectal Cancer
- Pancreatic Cancer
- Liver Disease
- Lung Cancer