CA-125 Test: Ovarian Cancer Marker Lab Guide
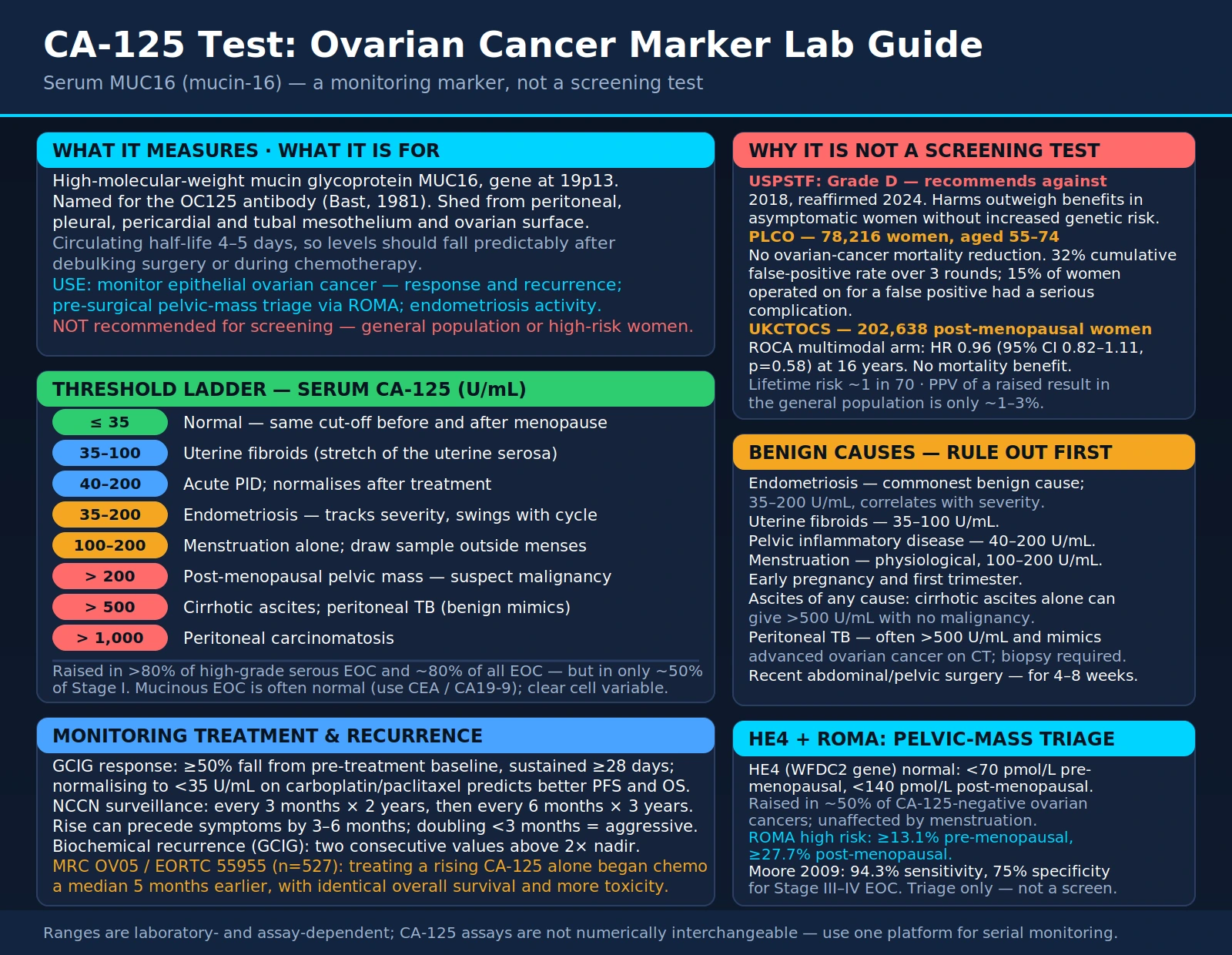
Table of Contents
- What is CA-125?
- Biology and Normal Values
- CA-125 in Ovarian Cancer
- Why CA-125 Alone Fails as a Screening Test
- PLCO and UKCTOCS: Definitive Screening Evidence
- HE4 and the ROMA Score
- Benign Causes of CA-125 Elevation
- CA-125 in BRCA1/2 Carriers and High-Risk Women
- Monitoring Treatment and Recurrence
- Key Research Papers
- Connections
- Featured Videos
What is CA-125?
CA-125 (Cancer Antigen 125) is a high-molecular-weight mucin glycoprotein encoded by the MUC16 gene on chromosome 19p13. Also known as mucin-16 (MUC16), the name "CA-125" reflects the monoclonal antibody (OC125) used to detect it, first developed by Robert Bast Jr. and colleagues in 1981.
In healthy adults, CA-125 is expressed on the surface of mesothelial cells lining the peritoneum, pleura, pericardium, and fallopian tubes, as well as the surface epithelium of the ovary. A normal serum CA-125 is ≤35 U/mL, established by the original OC125 immunoradiometric assay; most second-generation assays retain the same cut-off.
CA-125 has several distinct clinical roles:
- Primary role: Monitoring epithelial ovarian cancer (EOC) — treatment response and recurrence detection.
- Pre-surgical triage: Adjunct in evaluating pelvic masses using the ROMA score (combined with HE4).
- Endometriosis: Reflects disease activity, though not diagnostic; fluctuates with the menstrual cycle.
- Other cancers: Less commonly used to monitor uterine, fallopian tube, and primary peritoneal carcinomas.
- NOT recommended for ovarian cancer screening in the general population or even high-risk women — see the PLCO and UKCTOCS trials.
Biology and Normal Values
MUC16 is a large transmembrane protein with a heavily glycosylated extracellular domain containing repeating SEA (Sea Urchin Sperm Protein, Enterokinase, Agrin) modules. Proteolytic cleavage and shedding of this extracellular portion into circulation is what is measured as "CA-125" in blood. In cancer, overexpression and accelerated shedding dramatically raises serum concentrations.
Physiologically, CA-125 acts as a lubricant and anti-adhesion molecule at mesothelial surfaces — preventing cells from sticking together in the peritoneal cavity. Its circulating half-life is approximately 4–5 days, which is clinically important: after a successful surgical debulking or during active chemotherapy, CA-125 levels should fall predictably, and a slower-than-expected fall signals inadequate response.
Reference Ranges
- Pre-menopausal: <35 U/mL (menstrual-phase elevation up to 100 U/mL is not pathological).
- Post-menopausal: <35 U/mL; because post-menopausal women lack the cyclic endometrial shedding that confounds results, any elevation >35 U/mL in a post-menopausal woman with a pelvic mass is more clinically significant.
- Markedly elevated (>200 U/mL): Strongly associated with malignancy in post-menopausal women with a pelvic mass; peritoneal carcinomatosis commonly produces values >1,000 U/mL.
- Menstrual cycle variation: CA-125 can double or triple during menstruation due to endometrial shedding. Blood should ideally be drawn outside menses for a reliable baseline.
Assay Generations
First-generation assays use only the OC125 antibody. Second-generation two-site assays (M11 + OC125) generally show better precision. These assays are not numerically interchangeable — always use the same assay platform for serial monitoring of an individual patient.
CA-125 in Ovarian Cancer
Epithelial ovarian cancer (EOC) is the deadliest gynecologic malignancy. Approximately 80% of cases are serous, endometrioid, clear cell, or mucinous histology — grouped as "Type II" high-grade serous cancers dominate, accounting for most deaths. CA-125 performance varies significantly by histologic subtype:
- High-grade serous EOC: CA-125 elevated (>35 U/mL) in >80% of cases; values at presentation often reach hundreds to thousands U/mL due to extensive peritoneal seeding.
- All EOC combined: CA-125 elevated in approximately 80% overall, but only ~50% of Stage I disease — the relatively low sensitivity for early-stage cancer is a fundamental limitation.
- Mucinous EOC: CA-125 is frequently normal in this subtype. CEA and CA19-9 are more reliable markers for mucinous tumors.
- Clear cell EOC: CA-125 elevation is variable and may be lower than expected for equivalent-stage serous disease.
Treatment Response Criteria
The Gynecologic Cancer InterGroup (GCIG) defines CA-125 response as ≥50% decrease from pre-treatment baseline, sustained for ≥28 days. Patients who normalize CA-125 (<35 U/mL) during first-line carboplatin/paclitaxel chemotherapy have significantly better progression-free and overall survival than those who do not normalize.
Surveillance After Complete Response
Standard surveillance (NCCN guidelines): CA-125 every 3 months for 2 years, then every 6 months for 3 years; a rising CA-125 on surveillance triggers CT imaging. CA-125 can precede clinical symptoms of recurrence by 3–6 months. However, the MRC OV05/EORTC 55955 trial demonstrated that triggering chemotherapy at CA-125-only recurrence — without waiting for symptoms — did not improve overall survival. Patients were simply exposed to platinum toxicity for longer without benefit. This finding is counterintuitive but robust, and means that rising CA-125 should prompt discussion and investigation, not immediate re-treatment.
CA-125 doubling time can help characterize recurrence: a doubling time shorter than 3 months suggests a more aggressive relapse.
Why CA-125 Alone Fails as a Screening Test
The idea of detecting ovarian cancer early via a simple blood test is appealing — ovarian cancer is often diagnosed late (Stage III–IV) precisely because early-stage disease is asymptomatic. Yet multiple large randomized trials have failed to show that CA-125-based screening saves lives. The core reasons are statistical and biological:
- Low disease prevalence in the general population: Ovarian cancer affects ~1 in 70 women lifetime, but new cases per year are rare. Even a test with 80% sensitivity and 99% specificity will generate many more false positives than true positives in a low-prevalence population. The positive predictive value (PPV) in the general population is only ~1–3%, meaning most elevated CA-125 results represent benign disease.
- Insufficient early-stage sensitivity: CA-125 is normal in ~50% of Stage I cancers — precisely the stage where cure is most achievable.
- High false-positive rate from benign conditions: Endometriosis, fibroids, PID, liver disease, and even menstruation all elevate CA-125, generating large numbers of false positives that trigger invasive workup.
- Harms of workup: False-positive CA-125 leads to diagnostic laparoscopy or laparotomy. Population studies show complication rates up to 15% for these procedures — perforations, infections, bowel injuries, anesthesia risks.
The USPSTF (2018, reaffirmed 2024) gives ovarian cancer screening with CA-125 or transvaginal ultrasound a Grade D recommendation — meaning the harms outweigh the benefits — for asymptomatic women without increased genetic risk. This is not a close call; it is a definitive recommendation against screening.
PLCO and UKCTOCS: Definitive Screening Evidence
Two large randomized controlled trials provide the definitive evidence base against CA-125 screening:
PLCO Trial (United States)
The Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial randomized 78,216 women aged 55–74 to annual CA-125 + transvaginal ultrasound (TVUS) for up to 4 rounds vs. usual care. Results:
- No reduction in ovarian cancer mortality in the screened group.
- 32% cumulative false-positive rate over 3 rounds of screening.
- 15% of women who underwent surgery for false-positive results experienced at least one serious complication.
- Conclusion: Screening caused net harm without saving lives (PMID 21249220).
UKCTOCS Trial (United Kingdom)
The UK Collaborative Trial of Ovarian Cancer Screening was the largest ovarian cancer screening RCT ever conducted. It randomized 202,638 post-menopausal women to three arms:
- Multimodal screening (MMS): Annual CA-125 using the Risk of Ovarian Cancer Algorithm (ROCA) + TVUS when CA-125 trend was rising.
- Annual TVUS alone.
- No screening (control).
The ROCA algorithm is more sophisticated than a single CA-125 cut-off: it models the pattern of CA-125 change over time, triggering repeat testing when CA-125 is rising even within the normal range. This approach was developed specifically to improve on the limitations of a single threshold. Yet the 2021 final analysis (16 years of follow-up) found:
- MMS did not significantly reduce ovarian cancer mortality (HR 0.96, 95% CI 0.82–1.11; p=0.58).
- TVUS alone also showed no mortality benefit.
- Conclusion: Even the most sophisticated CA-125 screening strategy tested to date failed to save lives from ovarian cancer (PMID 33956050).
These two trials collectively enrolled over 280,000 women and followed them for up to 16 years. Their consistent null finding is the reason professional societies worldwide recommend against ovarian cancer screening in the general population.
HE4 and the ROMA Score
While CA-125 alone is not adequate for screening, combining it with a second biomarker significantly improves pre-surgical characterization of pelvic masses.
HE4 (Human Epididymis Protein 4)
HE4 is encoded by the WFDC2 gene and is overexpressed in ovarian and endometrial cancers. Key characteristics:
- Normal values: <70 pmol/L (pre-menopausal), <140 pmol/L (post-menopausal).
- Elevated in approximately 50% of ovarian cancers that are CA-125-negative — highly complementary to CA-125.
- Higher specificity than CA-125 for malignancy: HE4 is much less frequently elevated in endometriosis, fibroids, and PID, the conditions that most commonly cause false-positive CA-125 results.
- Not significantly elevated during menstruation — avoids the cyclic variation that complicates CA-125 interpretation in pre-menopausal women.
ROMA Score
The Risk of Ovarian Malignancy Algorithm (ROMA) is an FDA-cleared validated algorithm that combines CA-125 + HE4 + menopausal status to generate a numerical probability of epithelial ovarian cancer in a woman presenting with a pelvic mass:
- High risk (pre-menopausal): ROMA ≥13.1%
- High risk (post-menopausal): ROMA ≥27.7%
In the pivotal validation study (Moore 2009, PMID 19582160), ROMA demonstrated 94.3% sensitivity and 75% specificity for detecting Stage III–IV EOC. The primary clinical application is pre-surgical triage: women with a newly detected pelvic mass who score high-risk on ROMA should be referred to a gynecologic oncologist (rather than a general gynecologist) for surgical evaluation — this routing decision affects staging adequacy and survival outcomes.
Important limitations: ROMA is not a diagnostic test and is not validated for cancer screening. It applies only to women who already have a pelvic mass identified by imaging.
OVA1 and Overa
OVA1 and its successor Overa are FDA-cleared multivariate index assays that incorporate CA-125 and HE4 along with additional protein biomarkers (transthyretin, apolipoprotein A1, beta-2 microglobulin for OVA1; transferrin and follicle-stimulating hormone for Overa). These panels offer modestly improved performance over ROMA alone for pre-surgical malignancy prediction and are used in the same clinical context.
Benign Causes of CA-125 Elevation
Understanding benign causes of CA-125 elevation is essential for avoiding unnecessary surgery. The following conditions commonly elevate CA-125, sometimes to levels that mimic advanced malignancy:
Gynecologic Conditions
- Endometriosis: The most common benign cause. CA-125 typically ranges 35–200 U/mL, correlating with disease severity (deeply infiltrating endometriosis produces higher values than superficial implants). Levels fluctuate significantly with the menstrual cycle. CA-125 is NOT useful for diagnosing or staging endometriosis — laparoscopy remains required.
- Uterine fibroids (leiomyomas): Mild elevation (35–100 U/mL) due to mechanical stretching of the uterine serosa and pressure on peritoneal mesothelium.
- Pelvic inflammatory disease (PID): Acute PID with peritoneal involvement commonly elevates CA-125 (40–200 U/mL); levels normalize after treatment.
- Menstruation: Physiological elevation up to 100–200 U/mL during menses due to endometrial shedding.
- Early pregnancy and first trimester: Elevated from placental trophoblast and decidual tissue.
Non-Gynecologic Conditions
- Liver disease and ascites: Any cause of ascites (cirrhosis, Budd-Chiari, heart failure) markedly elevates CA-125 from peritoneal mesothelium. Cirrhotic ascites alone can produce CA-125 >500 U/mL without malignancy.
- Pleural effusion: CA-125 elevation from pleural mesothelium; seen with mesothelioma, TB pleuritis, and congestive heart failure.
- Peritoneal tuberculosis: A critical diagnostic trap — CA-125 is often very high (>500 U/mL) and peritoneal TB can mimic advanced ovarian cancer both clinically and on CT imaging. Biopsy is required to distinguish these. Misdiagnosing TB as ovarian cancer and initiating chemotherapy is a preventable error.
- Recent abdominal or pelvic surgery: Post-surgical peritoneal inflammation elevates CA-125 for 4–8 weeks after the procedure.
- Pancreatic and other GI cancers: CA-125 can be secondarily elevated, though CEA and CA19-9 are the primary markers for these malignancies.
Clinical Interpretation Rule
In pre-menopausal women with a pelvic mass, a CA-125 value up to 200 U/mL must be interpreted cautiously — endometriosis and PID are common mimics. Post-menopausal women have a narrower differential for elevated CA-125, and the threshold for surgical evaluation is appropriately lower.
CA-125 in BRCA1/2 Carriers and High-Risk Women
Women with germline BRCA1 or BRCA2 mutations face dramatically elevated ovarian cancer risk:
- BRCA1: 40–60% lifetime risk vs. ~1.2% population baseline.
- BRCA2: 20–30% lifetime risk.
For many years, annual TVUS + CA-125 was standard surveillance for BRCA carriers. This practice has been largely abandoned based on the evidence from UKCTOCS and PLCO, which showed no mortality benefit even from optimized screening strategies.
Current NCCN/ACOG/SGO Recommendations (2024)
- BRCA1 carriers: Risk-reducing salpingo-oophorectomy (RRSO) at age 35–40, after completing childbearing, is the only intervention proven to reduce ovarian cancer mortality. Surveillance does NOT substitute for RRSO.
- BRCA2 carriers: RRSO at age 40–45 recommended; the urgency is somewhat less than BRCA1 because peak risk onset is later.
- If surveillance is chosen (patient declines or delays RRSO): the ROCA algorithm (serial CA-125 trend analysis) + TVUS every 6 months at a gynecologic oncology center is the preferred approach — but patients must understand this is not proven to reduce mortality and is offered as a harm-reduction option only.
- After RRSO: Routine CA-125 surveillance is not recommended. The residual risk of primary peritoneal carcinoma after RRSO is very low, and surveillance of this risk has not been shown to improve outcomes.
Lynch Syndrome
Women with Lynch syndrome (germline MLH1, MSH2, MSH6, or PMS2 mutations) face elevated risk of endometrial and, to a lesser degree, ovarian cancer. Annual endometrial sampling plus gynecologic exam is recommended. The utility of CA-125 in Lynch syndrome surveillance is uncertain and not currently supported by guideline-level evidence.
Monitoring Treatment and Recurrence
Monitoring ovarian cancer treatment is where CA-125 provides its clearest clinical value, despite the counterintuitive finding from MRC OV05 that acting immediately on a rising CA-125 does not improve survival.
During First-Line Chemotherapy
CA-125 is measured at baseline and before each cycle of carboplatin + paclitaxel. The GCIG criteria define treatment response as a ≥50% decrease from pre-treatment baseline sustained for ≥28 days. Patients who normalize CA-125 (<35 U/mL) achieve significantly better progression-free and overall survival than those whose CA-125 does not normalize.
CA-125 and Recurrence Timing: MRC OV05/EORTC 55955
The MRC OV05/EORTC 55955 trial (2010, PMID 20709966) enrolled 527 patients with CA-125-confirmed recurrence and randomized them to early chemotherapy (triggered by rising CA-125) vs. delayed treatment (until clinical symptoms or imaging evidence). Results:
- Early treatment began a median of 5 months earlier in the early arm.
- Overall survival was identical between arms.
- Patients in the early arm had longer cumulative exposure to platinum toxicity (peripheral neuropathy, nephrotoxicity, ototoxicity) without benefit.
The practical implication: inform patients when CA-125 is rising and engage them in shared decision-making about timing of reinvestigation — but do not automatically initiate chemotherapy based on biochemical recurrence alone. The GCIG biochemical recurrence definition (CA-125 on two consecutive measurements above 2× nadir) is a trigger for discussion and imaging, not necessarily immediate treatment.
Maintenance Therapies
- Bevacizumab maintenance: CA-125 is monitored during therapy. Some patients develop CA-125 elevation from bevacizumab-associated ascites or effusion management — interpret carefully in context of imaging and symptoms rather than as presumed recurrence.
- PARP inhibitor maintenance (olaparib, niraparib, rucaparib): Serial CA-125 during maintenance reflects ongoing disease control. Stable or declining CA-125 on PARP inhibitor maintenance is a favorable sign; rising CA-125 may indicate emerging resistance and warrants imaging.
Key Research Papers
- Bast RC Jr. et al. (1981). A radioimmunoassay using a monoclonal antibody to monitor the course of epithelial ovarian cancer. N Engl J Med. Search PubMed
- Buys SS et al. (2011). PLCO trial: effect of screening on ovarian cancer mortality. JAMA. Search PubMed
- Menon U et al. (2021). UKCTOCS final mortality analysis: 16-year follow-up. Lancet. Search PubMed
- Rustin GJ et al. (2010). MRC OV05/EORTC 55955: early vs delayed treatment on rising CA-125. Lancet. Search PubMed
- Moore RG et al. (2009). ROMA score: CA-125 + HE4 for pre-surgical evaluation. Gynecol Oncol. Search PubMed
- Pinsky PF et al. (2013). PLCO false-positive CA-125 surgery complication harms. J Natl Cancer Inst. Search PubMed
- Markman M et al. (2006). GCIG CA-125 response criteria consensus statement. Gynecol Oncol. Search PubMed
- NCCN Clinical Practice Guidelines in Oncology: Ovarian Cancer (2018). CA-125 surveillance recommendations — Search PubMed
- Anastasi E et al. (2010). CA-125 in endometriosis: a systematic review. Gynecol Endocrinol. Search PubMed
- Jacobs I et al. (2011). ROCA prospective study in UKCTOCS: CA-125 trend algorithm performance. Cancer Prev Res. Search PubMed
- Vergote I et al. (2010). BRCA: RRSO vs. surveillance outcomes for ovarian cancer risk. J Clin Oncol. Search PubMed
- Ledermann JA et al. (2012). Olaparib maintenance in platinum-sensitive relapsed ovarian cancer; CA-125 monitoring. N Engl J Med. Search PubMed
Connections
- All Lab Tests
- AFP Test
- CEA Test
- PSA Test
- Complete Blood Count
- Comprehensive Metabolic Panel
- Ovarian Cancer
- Endometriosis
- Uterine Fibroids
- Cervical Cancer