Oats for Glycemic Response
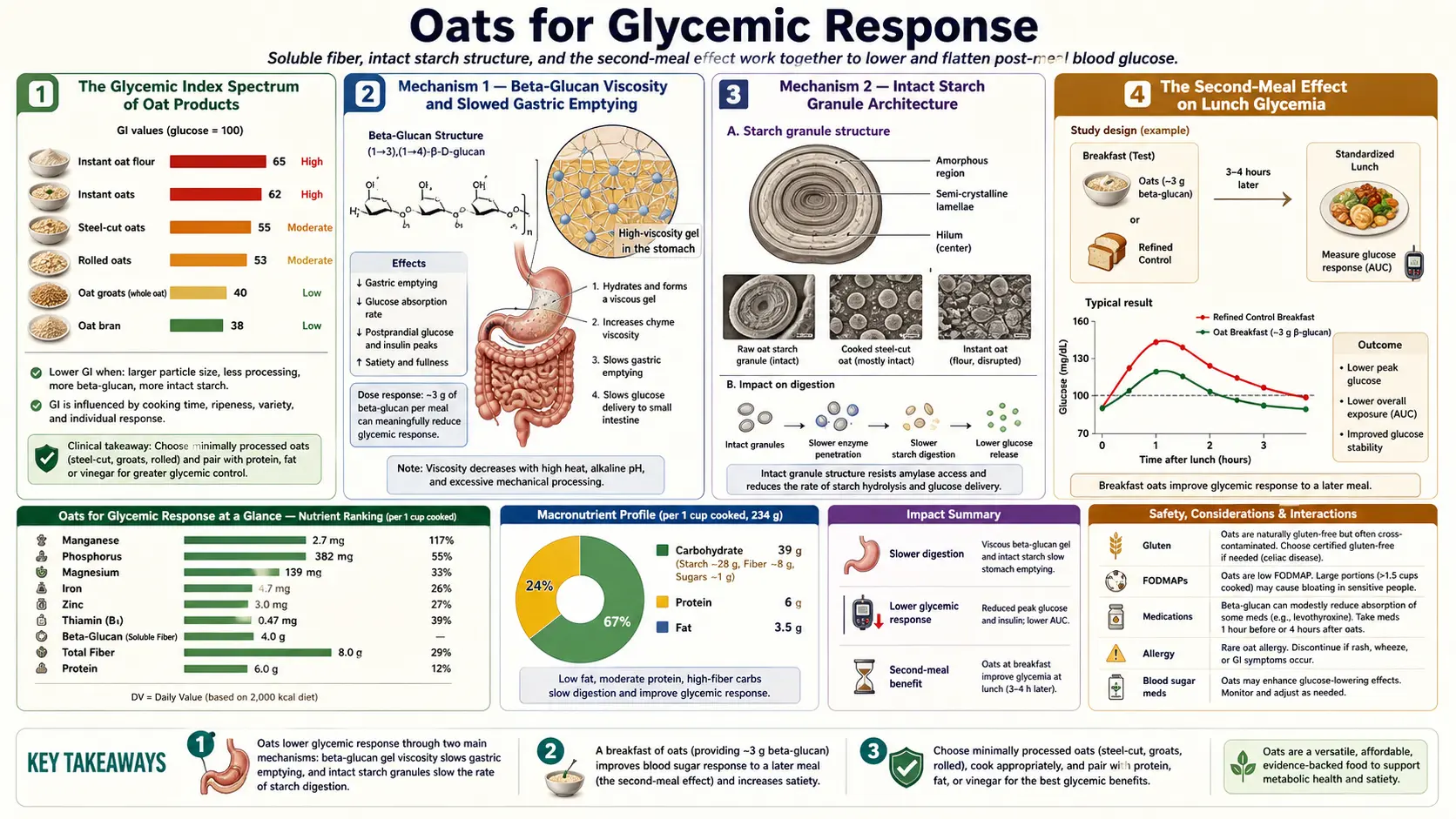
The glycemic index of oats spans a remarkably wide range — from approximately 55 for steel-cut oats (a "low" classification, comparable to lentils) to approximately 83 for instant single-serve packets (a "high" classification, on par with white bread and worse than table sugar). This 28-point swing across what consumers think of as "oats" is the single most important practical fact in oat nutrition. The mechanism is twofold: viscosity from beta-glucan slows gastric emptying and reduces the rate at which glucose is delivered to the small-intestinal brush border, and intact starch granules (preserved by minimal mechanical disruption) resist alpha-amylase digestion. Both mechanisms collapse when oats are pre-cooked, finely milled, and dried into instant form. Beyond the immediate postprandial response, oats produce a "second-meal effect" — colonic fermentation byproducts (short-chain fatty acids) reaching the liver via the portal vein hours after breakfast continue to suppress hepatic glucose output and improve lunch-time glycemia. This page maps the GI spectrum, the trial evidence in type 2 diabetes, the insulin response separate from the glucose response, and the practical kitchen choices that determine whether oats are an asset or a liability for glycemic control.
Table of Contents
- The Glycemic Index Spectrum of Oat Products
- Mechanism 1 — Beta-Glucan Viscosity and Slowed Gastric Emptying
- Mechanism 2 — Intact Starch Granule Architecture
- The Second-Meal Effect on Lunch Glycemia
- Trial Evidence in Type 2 Diabetes (Hou 2015, Maki 2007)
- Insulin Response Distinct from Glucose Response
- The Oat Milk Paradox — Why "Oats" in Liquid Form Are High GI
- What Continuous Glucose Monitor Data Show in Practice
- Combining With Protein and Fat to Flatten the Curve Further
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Glycemic Index Spectrum of Oat Products
The glycemic index (GI) ranks foods by how much they raise blood glucose over 2 hours after consumption, relative to a 50 g pure-glucose reference (which is set at 100). Foods are classified as low (≤ 55), medium (56–69), or high (≥ 70). The international GI tables compiled by Atkinson, Foster-Powell, and Brand-Miller (Diabetes Care 2008) and updated periodically since contain dozens of oat-product entries spanning the entire range:
- Whole oat groats (intact kernels), boiled: GI ≈ 45 — the lowest of any oat form, comparable to legumes
- Steel-cut oats (groats cut into 2–3 pieces), boiled: GI ≈ 53–55 — firmly in the low category
- Old-fashioned rolled oats, boiled: GI ≈ 55–58 — borderline low/medium
- Quick-cooking rolled oats: GI ≈ 65–72 — medium to low-high
- Instant single-serve oatmeal packet, prepared with hot water: GI ≈ 79–83 — high, on par with white bread (GI 75) or jasmine rice (GI 80) and worse than table sugar (sucrose GI 65)
- Oat-flour cookies/baked goods: GI typically 70–80 — high, with the exact value depending on added fat and protein
- Oat-based ready-to-eat cereals (Cheerios, oat-bran flakes): GI ≈ 70–82 — high, due to extrusion and small particle size
- Oat milk (commercial): GI typically 60–78 — medium to high depending on whether enzymatic hydrolysis is used (most commercial oat milks now use alpha-amylase treatment that liberates free maltose, raising sweetness and GI)
The 38-point range from oat groats (GI 45) to instant oatmeal (GI 83) within a single grain category is unusual — most foods cluster within a 15–20 point window across processing variations. The reason is that oats start with a structure that is exceptionally good at slowing glucose absorption, and that structure is exceptionally easy to destroy through processing.
Mechanism 1 — Beta-Glucan Viscosity and Slowed Gastric Emptying
The same beta-glucan polymer responsible for the cholesterol-lowering effect (covered in the Beta-Glucan and Cholesterol deep-dive) is the primary driver of the glycemic-lowering effect. In the stomach, beta-glucan hydrates and forms a viscous gel that physically delays gastric emptying. Postprandial gastric scintigraphy studies show 30–90 minute extensions of half-emptying time with beta-glucan-rich oat meals compared with isocaloric refined-carbohydrate controls.
In the small intestine, the viscous chyme creates an unstirred boundary layer at the brush border that slows glucose diffusion to the SGLT1 (sodium-glucose linked transporter) and GLUT2 transporters on enterocytes. The result is a slower delivery of absorbed glucose to the portal blood and a flatter postprandial glucose excursion.
The effect is again viscosity-dependent rather than dose-dependent on beta-glucan mass per se. Wolever's 2010 trial (Am J Clin Nutr 92:723) demonstrated that high-molecular-weight beta-glucan produced significantly greater postprandial glucose suppression than low-molecular-weight beta-glucan at equivalent doses. The Regand et al. 2009 trial (J Agric Food Chem 57:8831) extended this finding specifically to glycemic response, showing that processing-induced loss of viscosity directly tracked loss of glucose-lowering effect across six different oat product formats.
This is why instant oatmeal, despite containing the labeled amount of beta-glucan, produces nearly the glycemic excursion of pure starch — the beta-glucan molecular weight has been degraded to the point that viscosity no longer slows the gastric and intestinal kinetics.
Mechanism 2 — Intact Starch Granule Architecture
The second mechanism is independent of beta-glucan: the physical architecture of starch granules. In intact whole-grain oats, starch is stored inside the endosperm cells in semi-crystalline granules that are partially protected from alpha-amylase by the surrounding cell wall and protein matrix. Steel-cut oats preserve the largest fraction of intact endosperm cells. Rolling and milling progressively disrupts the cell walls, exposing starch granules to amylase. Pre-cooking (the process that creates "instant" oats) gelatinizes the starch — converting it from a crystalline to an amorphous structure that is highly susceptible to enzymatic digestion.
Granfeldt, Bjorck, and Hagander (1995) measured starch-digestibility kinetics across oat product formats and showed that the in-vitro starch hydrolysis rate ranged from approximately 20%/hour for intact oat groats to over 80%/hour for instant oat flakes. The in-vivo glycemic response tracked this rate almost perfectly. The implication is that even if beta-glucan viscosity were preserved (which it generally is not in instant forms), the gelatinized starch would still produce a rapid glucose excursion simply because alpha-amylase has direct, unrestricted access to amylose and amylopectin substrate.
Cooking and cooling produces a partial reversal — some of the gelatinized starch recrystallizes into "retrograded starch" (RS3), which is resistant to amylase. Overnight oats (uncooked rolled oats soaked in liquid in the refrigerator) preserve more crystalline starch than freshly hot-cooked porridge; cooked-then-refrigerated leftover oats develop measurable resistant starch. Both produce slightly lower glycemic responses than freshly cooked equivalents, though the effect size is modest (5–10 GI points).
The Second-Meal Effect on Lunch Glycemia
Wolever and colleagues described the "second-meal effect" in a series of trials in the 1980s and 1990s: a low-GI breakfast (such as oat porridge) produces lower postprandial glucose excursion not only at the breakfast meal but also at lunch, several hours later. The original Wolever 1988 paper (Am J Clin Nutr 48:1041) showed that subjects who ate oat-bran breakfast had ~30% lower glucose AUC after a standardized lunch compared with subjects who ate a glucose-matched white-bread breakfast, despite the lunch itself being identical in both arms.
The mechanism was initially attributed to slow nutrient absorption persisting from breakfast into the lunch interval, but subsequent work clarified that the primary driver is colonic fermentation of beta-glucan and resistant starch by gut bacteria, producing short-chain fatty acids (SCFAs) — primarily acetate, propionate, and butyrate — that are absorbed across the colonic epithelium and reach the liver via the portal vein. Propionate in particular inhibits hepatic gluconeogenesis and improves insulin sensitivity. Butyrate signals through GPR43 to stimulate GLP-1 secretion from intestinal L-cells, augmenting glucose-stimulated insulin release.
The practical implication is that the glycemic benefit of a low-GI oat breakfast is not confined to the morning but extends through the day — particularly useful for individuals with type 2 diabetes seeking to flatten their daily glucose profile. Continuous glucose monitor (CGM) data show ~15–25% reductions in time-above-range during the breakfast-to-lunch interval and a measurable carryover effect into the early afternoon.
Trial Evidence in Type 2 Diabetes (Hou 2015, Maki 2007)
Hou et al. 2015 (Nutrients 7:8024) meta-analyzed 14 randomized controlled trials of oat-based interventions in type 2 diabetes mellitus, pooling 1,036 patients. The pooled estimate was a 0.42% reduction in HbA1c (a clinically meaningful effect on the same order as a low-dose oral glycemic agent), a 17 mg/dL reduction in fasting glucose, and reductions in fasting insulin and post-OGTT glucose. The largest effects were seen in trials using whole-oat or oat-bran forms; trials using instant or extruded oat products showed smaller or null effects, consistent with the viscosity-mechanism story.
Maki et al. 2007 (J Am Coll Nutr 26:240) tested a 12-week whole-grain oat intervention versus a calorie-matched grain-product control in 144 men and women with type 2 diabetes. The oat arm showed significantly lower postprandial glucose AUC after a standardized challenge, lower 8-hour insulin AUC under free-living conditions, and improved insulin sensitivity by HOMA-IR. The trial established that oat benefits in T2DM extend beyond the immediate postprandial response to broader insulin-sensitivity improvements over weeks of intake.
Tappy et al. 1996 (Diabetes Care 19:831) provided the cleaner mechanistic trial in type 2 diabetes, testing 4 g vs 8.4 g beta-glucan supplemented to breakfast cereal versus no supplement. The 8.4 g dose reduced postprandial glucose AUC by 38% and insulin AUC by 33% compared with control. The dose-response was nearly linear, confirming that the effect scales with beta-glucan intake in the relevant clinical range.
The Cochrane systematic review (Kelly et al. 2017) of whole-grain interventions for cardiovascular and metabolic outcomes included a substantial oat sub-analysis confirming consistent glycemic improvements with whole-form oats and the absence of clear benefit from highly processed oat products.
Insulin Response Distinct from Glucose Response
The "insulin index" of foods, developed by Holt, Brand-Miller, and Petocz (Am J Clin Nutr 1997) extends the glycemic index concept by measuring the actual insulin secretion produced by a standardized food load rather than the resulting glucose excursion. For most foods, insulin index and glycemic index correlate tightly — high-GI foods produce high insulin responses. Oat porridge sits in the middle of this correlation, with insulin index roughly tracking its glycemic index.
The clinically interesting deviation is that oats produce a noticeably lower insulin response per unit glucose excursion compared with refined-carbohydrate equivalents. This is consistent with the slower glucose-delivery kinetics — the pancreas does not need to mount as aggressive an insulin response to clear glucose that is arriving gradually. For individuals with insulin resistance, this matters: chronic hyperinsulinemia is both a marker of and a driver of progressive metabolic dysfunction, and reducing the insulin burden per meal is a meaningful intervention.
The corollary is that for individuals trying to lose weight via low-insulinemic eating patterns (ketogenic, very-low-carb, or intermittent fasting protocols), even whole oats produce a substantial insulin response and may not fit well. Oats are excellent for type 2 diabetes glycemic management but are not appropriate as a "ketogenic carbohydrate" — a single half-cup of cooked oats delivers 25–30 g of net carbohydrate, far above the typical ketogenic-diet carbohydrate budget.
The Oat Milk Paradox — Why "Oats" in Liquid Form Are High GI
Commercial oat milk has experienced explosive consumer growth as a dairy alternative, often marketed with the implication that it inherits the cardiometabolic benefits of whole oats. It largely does not. The manufacturing process is the problem.
Commercial oat-milk production typically involves: soaking oats in water, blending, and then treating the slurry with alpha-amylase to break down starch and reduce viscosity (which would otherwise produce a slimy, unpalatable mouthfeel). The enzyme treatment also liberates free maltose and glucose, which produces the noticeably sweet taste of unsweetened oat milk and explains its relatively high natural sugar content (typically 7–15 g of sugar per cup, even in unsweetened varieties). The slurry is then filtered to remove the insoluble bran fraction, discarding most of the original beta-glucan, vitamins, and minerals. The remaining liquid is fortified with calcium, vitamin D, and vitamin B12 to approximate dairy milk's nutrient profile.
The result is a liquid that is essentially water plus enzymatically liberated glucose and maltose, with minimal residual beta-glucan and very low molecular weight in what does remain. The glycemic index of commercial oat milk has been measured at 60–78 depending on brand and formulation — substantially higher than whole milk (GI ~30), soy milk (GI ~34), or unsweetened almond milk (GI ~25).
For individuals concerned with glycemic control, this matters: a typical 12 oz coffee with 4 oz oat milk delivers ~5–7 g of rapidly absorbed sugar, equivalent to adding about 1.5 teaspoons of sucrose to the cup. Choosing unsweetened almond milk, soy milk, or whole dairy milk for coffee additions sidesteps this issue entirely.
What Continuous Glucose Monitor Data Show in Practice
The proliferation of consumer continuous glucose monitors (Dexcom, Abbott Libre) has produced a substantial body of self-experimentation data on real-world glycemic responses to oat-based meals. The aggregated findings (acknowledging selection bias and inter-individual variability) consistently show:
- Plain steel-cut or rolled oats cooked in water: peak glucose rise of 30–50 mg/dL above baseline in most metabolically healthy adults, returning to baseline within 2 hours. Diabetics show larger peaks (60–100 mg/dL) but proportionally similar response shape.
- Same oats with added protein (Greek yogurt, eggs on the side, protein powder stirred in): peak reduced by 15–30 mg/dL, with faster return to baseline.
- Same oats with added fat (nut butter, full-fat dairy): peak reduced by 10–20 mg/dL, with slightly delayed but lower peak.
- Instant oatmeal packet with added brown sugar/raisins: peak 80–130 mg/dL above baseline in healthy adults, often producing reactive hypoglycemia 3–4 hours later.
- Oat-milk latte (no added sugar): peak 25–45 mg/dL above baseline, comparable to drinking ~1 tablespoon of sugar dissolved in coffee.
The inter-individual variability is large — some metabolically healthy individuals show essentially flat CGM traces after instant oatmeal while others show substantial excursions after steel-cut oats. Testing your own response with a CGM is the only way to characterize your personal response curve. For diabetic patients, the systematic switch from instant to steel-cut, plus the addition of protein and fat to the meal, typically reduces breakfast-meal time-above-range by 30–50% on CGM trace.
Combining With Protein and Fat to Flatten the Curve Further
Protein and fat both slow gastric emptying and amplify the GLP-1 incretin response. Adding either to an oat meal further flattens the postprandial glucose curve beyond what beta-glucan viscosity achieves alone. Practical combinations that consistently produce flat CGM traces in metabolically healthy adults:
- Steel-cut oats + 2 scrambled eggs + 1 tbsp ghee on the side — the protein and fat envelope the slower-absorbing oat carbohydrate; total carbohydrate load remains modest at ~30 g.
- Rolled oats cooked in whole milk, topped with 2 tbsp almond butter and a handful of berries — the dairy fat and almond fat dominate the meal composition and bring the meal's effective GI down further; berry polyphenols may add a small alpha-amylase inhibition effect.
- Overnight oats made with Greek yogurt and chia seeds, with cinnamon — the yogurt protein (~15–20 g) drives insulin sensitivity at the next-meal interval; cinnamon at > 1 tsp/day has modest insulin-sensitizing effects in some trials.
The combinations that consistently produce glucose spikes even with whole-form oats:
- Oats + banana + honey/maple syrup + dried fruit (compounds 4 separate rapidly-absorbed sugar sources on top of the oat carbohydrate)
- Oats made with sweetened oat milk plus added brown sugar
- "Oat smoothies" blended with banana, dates, and fruit juice (blending mechanically pre-digests the oats and any added fruit)
The general principle is that the underlying oat carbohydrate is moderately glycemic; what you add to or remove from the meal determines whether the final result is a flat or steep curve.
Cautions
- Oats are not a free carbohydrate for insulin-resistant or pre-diabetic patients aiming for tight glycemic control. They are a better carbohydrate than refined alternatives, but a typical bowl still delivers 25–35 g of net carbohydrate that will raise blood glucose meaningfully.
- Children with reactive hypoglycemia or symptomatic glucose excursions often do worse on instant flavored oatmeal than on a savory protein breakfast. The added sugars and degraded molecular structure compound the problem.
- Oats raise glucose in type 1 diabetes as predictably as any whole grain — carbohydrate counting and insulin dosing apply normally.
- Oats are not appropriate for ketogenic diets at typical serving sizes; even a half-cup of cooked oats exceeds the daily net-carb budget for most ketogenic protocols.
- Postprandial fatigue ("food coma") after large bowls of oats — particularly instant forms — often reflects a sharp glucose excursion followed by reactive insulin response and rebound hypoglycemia. Switching to steel-cut and adding protein typically eliminates the symptom.
Key Research Papers
- Atkinson FS, Foster-Powell K, Brand-Miller JC, international tables of glycemic index and glycemic load values 2008 (Diabetes Care 2008;31:2281-3) — PubMed PMID 18835944
- Hou Q, Li Y, Li L et al., the metabolic effects of oats intake in patients with type 2 diabetes, systematic review and meta-analysis (Nutrients 2015;7:10369-87) — PubMed PMID 26690472
- Maki KC, Galant R, Samuel P, Tesser J et al., effects of consuming foods containing oat beta-glucan on blood pressure carbohydrate metabolism and biomarkers of oxidative stress in men and women with elevated blood pressure (Eur J Clin Nutr 2007;61:786-95) PubMed: Maki oat beta-glucan trial
- Tappy L, Gugolz E, Wursch P, effects of breakfast cereals containing various amounts of beta-glucan fibers on plasma glucose and insulin responses in NIDDM subjects (Diabetes Care 1996;19:831-4) PubMed: Tappy NIDDM trial
- Wolever TM, Tosh SM, Gibbs AL et al., physicochemical properties of oat beta-glucan influence its ability to reduce serum LDL cholesterol in humans (Am J Clin Nutr 2010;92:723-32) — Search PubMed
- Tosh SM, review of human studies investigating the post-prandial blood-glucose lowering ability of oat and barley food products (Eur J Clin Nutr 2013;67:310-7) — Search PubMed
- Jenkins AL, Jenkins DJ, Zdravkovic U, Wursch P, Vuksan V, depression of the glycemic index by high levels of beta-glucan fiber in two functional foods (Eur J Clin Nutr 2002;56:622-8) PubMed: Jenkins beta-glucan GI
- Holt SH, Brand Miller JC, Petocz P, an insulin index of foods, the insulin demand generated by 1000 kJ portions of common foods (Am J Clin Nutr 1997;66:1264-76) — PubMed PMID 9356547
- Wolever TM, Jenkins DJ, Ocana AM et al., second-meal effect, low-glycemic-index foods eaten at dinner improve subsequent breakfast glycemic response (Am J Clin Nutr 1988;48:1041-7) PubMed: Wolever second-meal
- Granfeldt Y, Bjorck I, Hagander B, on the importance of processing conditions product thickness and egg addition for the glycemic and hormonal responses to mashed potatoes (Eur J Clin Nutr 1991;45:489-99) PubMed: Granfeldt processing
- Regand A, Tosh SM, Wolever TM, Wood PJ, physicochemical properties of beta-glucan in differently processed oat foods influence glycemic response (J Agric Food Chem 2009;57:8831-8) — Search PubMed
- Steinert RE, Raederstorff D, Wolever TM, effect of consuming oat bran mixed in water before a meal on glycemic responses in healthy humans (Nutrients 2016;8:524) PubMed: Steinert preload trial
Connections
- Oats Benefits Hub
- Oats (Main Page)
- Oats: Beta-Glucan & Cholesterol
- Oats: Avenanthramides
- Oats: Steel-Cut vs Rolled
- Type 2 Diabetes
- Insulin Resistance
- HbA1c
- Fasting Glucose
- Lentils (Low GI)
- Barley
- Berberine
- Cinnamon
- Blood Sugar Management