Sjögren's Syndrome: History and Discovery
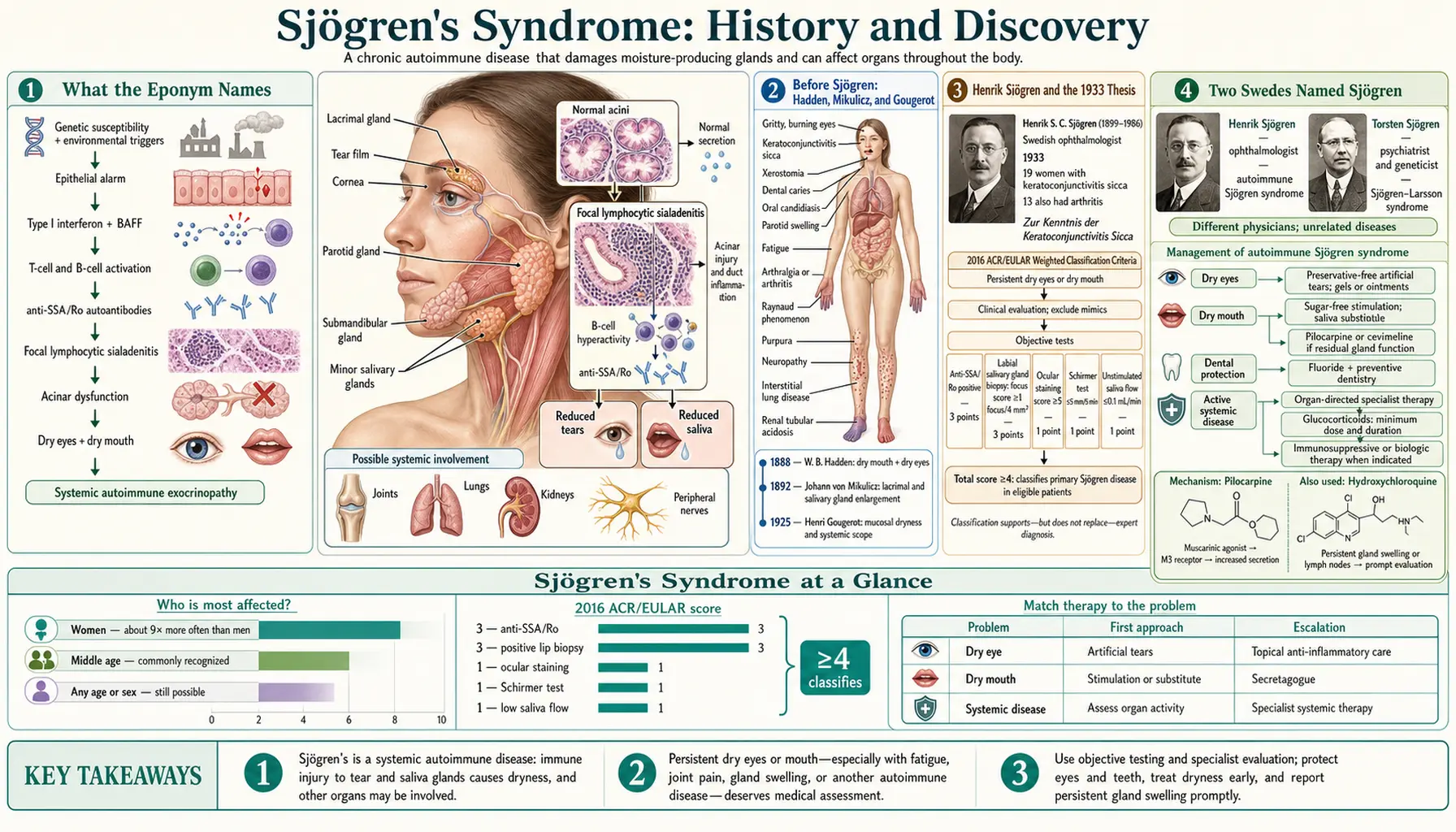
Sjögren's syndrome is named for Henrik Sjögren (1899–1986), a Swedish ophthalmologist whose 1933 doctoral thesis, Zur Kenntnis der Keratoconjunctivitis sicca, brought together dry eyes (keratoconjunctivitis sicca), dry mouth (xerostomia), and joint disease into a single recognizable picture. He was not the first to notice the pieces — Hadden (1888) reported a patient with both dry eyes and dry mouth, Mikulicz (1892) described enlarged tear and salivary glands, and Gougerot (1925) in France linked tear-gland failure to filamentary keratitis. Sjögren's contribution was to study the condition systematically and argue it was one disease. Its autoimmune nature, the anti-Ro/SSA and anti-La/SSB antibodies, the raised lymphoma risk, and the primary-versus-secondary distinction all came decades later. This page traces that history carefully, separating earlier partial reports from the eponym and from the modern science.
Table of Contents
- What the Eponym Names
- Before Sjögren: Hadden, Mikulicz, and Gougerot
- Henrik Sjögren and the 1933 Thesis
- Two Swedes Named Sjögren
- Translation, Recognition, and the Eponym
- Discovering the Autoimmune Cause
- The anti-Ro/SSA and anti-La/SSB Antibodies
- The Lymphoma Connection and Modern Classification
- Legacy and Open Questions
- Research Papers and References
- Connections
- Featured Videos
What the Eponym Names
Sjögren's syndrome is a chronic autoimmune disease in which the immune system attacks the body's moisture-producing glands — chiefly the lacrimal (tear) glands and the salivary glands. The two defining features are keratoconjunctivitis sicca (dry, gritty, inflamed eyes from reduced tear production) and xerostomia (dry mouth from reduced saliva). Because the disease is systemic, it commonly travels with joint pain or arthritis, profound fatigue, and dryness of other surfaces, and in some patients it affects the lungs, kidneys, nerves, and blood vessels. Today it is recognized as one of the most common systemic autoimmune diseases, particularly in women.
The word syndrome — a cluster of signs and symptoms that travel together — is the key to its history. The individual symptoms of dry eyes and dry mouth had been noticed by clinicians in the nineteenth century. What had not been done, until Henrik Sjögren's thesis, was the careful clinical and pathological work needed to argue that these features, together with the arthritis that so often accompanied them, represented a single distinct disorder rather than unrelated complaints. The history of the eponym is therefore really the history of an idea: that scattered dryness and joint disease are one thing.
It is worth noting at the outset that medical usage has been shifting. International expert consensus published in recent years (the 2023 Rome nomenclature statement) has favored the term Sjögren disease over Sjögren's syndrome, on the reasoning that it is a defined disease entity rather than a loose syndrome. Both names refer to the same condition; this page uses the long-familiar Sjögren's syndrome while noting the newer preference.
Before Sjögren: Hadden, Mikulicz, and Gougerot
Several physicians described pieces of the picture decades before 1933, and honesty about the record means giving them their due. In 1888, the English physician W. B. Hadden, working in London, presented a patient with both severe dry mouth and dry eyes — an early report explicitly linking the two glandular failures that would later become the hallmark of the syndrome. Hadden's case is widely cited as the first clear clinical association of xerostomia with keratoconjunctivitis sicca in the same person. (A handful of even earlier nineteenth-century mentions of dry mouth or dry eye exist in the literature, but Hadden's 1888 report is the one consistently credited with joining the two.)
In 1892, the surgeon Johann von Mikulicz-Radecki described a 42-year-old man with symmetrical enlargement of the lacrimal, parotid, and submandibular glands, and — crucially — examined the glands microscopically and found them infiltrated by small round (mononuclear) cells. This was an early histological glimpse of the gland inflammation that underlies Sjögren's, and the picture of bilateral tear- and salivary-gland swelling became known as Mikulicz disease. The relationship between “Mikulicz disease” and Sjögren's syndrome was debated for much of the twentieth century; today the benign lymphoepithelial gland lesion Mikulicz described is regarded as overlapping with, or a presentation within, the Sjögren spectrum, though some cases historically labeled Mikulicz disease are now attributed to IgG4-related disease.
In 1925, the French dermatologist Henri Gougerot described patients with failure of the lacrimal and salivary glands together with filamentary keratitis, framing the dryness as a systemic glandular insufficiency. Because of Gougerot's contribution, French-language sources to this day frequently call the condition “Gougerot-Sjögren syndrome” (syndrome de Gougerot-Sjögren) — a usage worth recognizing, since it credits the earlier French observations alongside the later Swedish synthesis. None of these earlier authors, however, assembled the full clinical-and-pathological argument that the dryness plus arthritis constituted one defined disease; that step is what the eponym ultimately commemorates.
Henrik Sjögren and the 1933 Thesis
Henrik Samuel Conrad Sjögren (1899–1986) was a Swedish ophthalmologist. In his 1933 doctoral thesis, written in German and titled Zur Kenntnis der Keratoconjunctivitis sicca (Keratitis filiformis bei Hypofunktion der Tränendrüsen) — roughly “On knowledge of keratoconjunctivitis sicca” — he reported a series of patients (commonly cited as 19 women, the majority of them past menopause) who had dry, filament-forming inflammation of the cornea and conjunctiva. He documented that many of these same patients also had dry mouth and, in a large fraction, chronic arthritis. The thesis combined a clinical part with a pathological part, and it was Sjögren who popularized the diagnostic term keratoconjunctivitis sicca itself and pioneered the use of rose bengal staining to reveal the damaged, dried ocular surface.
Sjögren's wife, Maria Hellgren Sjögren — herself from a distinguished ophthalmological family — is consistently credited in historical accounts with assisting him in the clinical work behind the thesis. Their collaboration is a recurring and well-attested detail of the story: the foundational case series rested in part on her help.
The decisive intellectual move was synthesis. Rather than treating dry eyes, dry mouth, and arthritis as coincidental, Sjögren argued from his cases and gland pathology that they were manifestations of a single systemic disorder of the secretory glands. That argument — not the bare observation of dryness, which predated him — is why his name became attached to the condition.
Two Swedes Named Sjögren
A point of frequent confusion deserves to be cleared up plainly, because the medical literature itself warns about it. There were two prominent, unrelated Swedish physicians named Sjögren active in roughly the same era, and they must not be conflated.
Henrik Sjögren (1899–1986), the ophthalmologist of this page, gave his name to Sjögren's syndrome (the dry-eye, dry-mouth autoimmune disease). A different man, Karl Gustaf Torsten Sjögren (1896–1974), was a Swedish psychiatrist and medical geneticist, unrelated except by the common surname. Torsten Sjögren's name is attached to several entirely separate, mostly inherited neurological conditions — including Sjögren–Larsson syndrome, Marinesco–Sjögren syndrome, and the Spielmeyer–Sjögren form of neuronal ceroid lipofuscinosis — which have nothing to do with the dry-gland autoimmune disease covered here.
Confusing the two is a genuine and documented pitfall, and reputable historical reviews of the surname exist specifically to disentangle them. For the purposes of this page: every reference to “Sjögren's syndrome,” the 1933 thesis, and keratoconjunctivitis sicca refers to Henrik the ophthalmologist.
Translation, Recognition, and the Eponym
Sjögren's thesis was, at first, under-appreciated. It received a mediocre examination grade (recorded as 1.5 on a 1–3 scale), which fell short of the mark needed for the docent (associate-professor) qualification and effectively foreclosed his hopes of a university academic career. The work was written in German for a Swedish audience, and for roughly a decade it remained little known outside Scandinavia.
Recognition came chiefly through translation. In 1943, the thesis was rendered into English by the Australian ophthalmologist John Bruce Hamilton under the title A New Conception of Keratoconjunctivitis Sicca. The English version put Sjögren's synthesis in front of the wider international medical community, and over the following years the condition came to be called “Sjögren's syndrome.” The eponym thus reflects not instant acclaim but a delayed appreciation that built over the 1940s and beyond, as clinicians elsewhere confirmed and extended his observations.
Sjögren himself went on to a respected clinical career in ophthalmology and lived to see the condition bearing his name become a recognized and actively studied disease. The gap between his under-rewarded 1933 defense and his later international standing is one of the more striking arcs in twentieth-century eponymous medicine.
Discovering the Autoimmune Cause
Henrik Sjögren described what the disease looked like; he did not establish why it happened. The concept of autoimmunity — the body's immune system mistakenly attacking its own tissues — did not become a workable, evidence-based framework until the 1950s and 1960s, well after his thesis. It is important not to read the modern autoimmune understanding back into the 1933 work; that explanation belongs to a later generation.
Across the 1950s and 1960s, researchers came to understand Sjögren's syndrome as an autoimmune exocrinopathy: a disease in which lymphocytes infiltrate and progressively damage the exocrine (secretory) glands, with the characteristic focal collections of immune cells visible on biopsy of the minor salivary glands — a finding that remains central to diagnosis. The recognition that the disease commonly coexists with other autoimmune rheumatic conditions, especially rheumatoid arthritis and lupus, reinforced its place within autoimmunity.
A landmark in this consolidation was the 1965 study by Kurt Bloch, W. W. Buchanan, Martin Wohl, and Joseph Bunim, “Sjögren's syndrome: a clinical, pathological, and serological study of sixty-two cases.” This careful 62-patient series helped define the modern clinical and serological profile of the disease and laid groundwork for the later separation of primary from secondary forms.
The anti-Ro/SSA and anti-La/SSB Antibodies
The autoantibodies now used to help diagnose Sjögren's syndrome were characterized in the late 1960s and 1970s — again, decades after the eponym was coined. Two laboratories working in parallel identified the same key antigen-antibody systems under different names, which is why the dual nomenclature persists today.
In 1969, Gordon Clark, Morris Reichlin, and Thomas Tomasi described a soluble cytoplasmic antigen reactive with sera from patients with systemic lupus erythematosus, naming the antigen Ro after the patient from whose serum the antibody was obtained. Around the same period, working on Sjögren's syndrome specifically, Alspaugh and Tan described antibodies they labeled SS-A and SS-B (Sjögren's Syndrome antigens A and B). It later became clear that Ro and SS-A referred to the same system, and that La and SS-B likewise coincided — an equivalence confirmed through interlaboratory exchange of sera around 1979. Hence the modern combined labels anti-Ro/SSA and anti-La/SSB.
These antibodies became, and remain, important diagnostic markers: anti-Ro/SSA in particular is incorporated into the modern classification criteria for the disease, alongside characteristic salivary-gland biopsy findings and objective tests of dry eyes and dry mouth. They are markers and classification aids, however — not all patients carry them, and their discovery is a chapter after the disease itself was defined, not part of its original description.
The Lymphoma Connection and Modern Classification
One of the most consequential modern findings is that Sjögren's syndrome carries an increased risk of non-Hodgkin lymphoma — the highest such risk among the systemic autoimmune rheumatic diseases. This was not part of Sjögren's original picture; it emerged from long-term follow-up of patients decades later. The pivotal report was the 1964 paper by Norman Talal and Joseph Bunim, “The Development of Malignant Lymphoma in the Course of Sjögren's Syndrome,” which documented lymphoma arising in patients followed for the disease and established the association as real and clinically important.
That link is now understood mechanistically as a progression from chronic immune stimulation of B-lymphocytes in the affected glands toward, in a minority of patients, clonal B-cell expansion and malignant lymphoma (often a marginal-zone / MALT lymphoma of the salivary glands). It is the reason persistent salivary-gland swelling and certain laboratory findings prompt closer monitoring. This is a genuine, evidence-based risk — though it remains a minority outcome, and it should be presented as a managed clinical concern rather than an inevitability.
The modern primary-versus-secondary distinction is likewise a later refinement. Patients with the dry-eye/dry-mouth disease occurring on its own were first grouped under terms such as “sicca syndrome” and later primary Sjögren's syndrome, while the same dryness occurring alongside another defined connective-tissue disease — classically rheumatoid arthritis, and later lupus or scleroderma — was called secondary Sjögren's syndrome. Formal classification criteria have been proposed and revised repeatedly since 1965, culminating in widely used international criteria in 2002 and the data-driven ACR–EULAR criteria of 2016, with the 2023 Rome consensus updating the nomenclature toward “Sjögren disease.”
Legacy and Open Questions
The arc of this history is a useful corrective to the idea that diseases are “discovered” in a single moment by a single person. The dryness was observed by Hadden in 1888; the gland pathology by Mikulicz in 1892; the systemic framing by Gougerot in 1925; the unifying clinical-and-pathological synthesis by Henrik Sjögren in 1933; the autoimmune cause across the 1950s–60s; the antibodies in 1969–1979; and the lymphoma risk and primary/secondary distinction in the 1960s and after. Each contributor added a layer, and the eponym fairly honors the synthesis while the fuller credit is shared.
Several things remain genuinely open. The ultimate trigger of the autoimmune attack is not settled: a combination of genetic susceptibility, hormonal factors (which may help explain the strong female predominance), and possible environmental or viral triggers is the leading hypothesis, but no single cause is proven, and it should be read as a hypothesis rather than established fact. Why some patients stay limited to dryness while others develop systemic organ involvement or lymphoma is also incompletely understood.
What is firmly established is the clinical reality the history produced: a recognizable, diagnosable, manageable autoimmune disease, with objective tests, defined antibodies, classification criteria, and a known need for long-term monitoring. From a Swedish ophthalmologist's under-graded 1933 thesis to an internationally classified disease entity, the story of Sjögren's syndrome is a model of how careful observation, honest attribution, and decades of accumulating science turn scattered symptoms into understood medicine.
Research Papers and References
The references below combine key historical and peer-reviewed sources with curated PubMed topic-search links. Where a specific landmark paper is well established, its DOI or PMID is given; broader historical themes are linked as PubMed topic searches. Each external link opens in a new tab. Henrik Sjögren's 1933 thesis and its 1943 English translation are named in the text as historical primary sources.
- Talal N, Bunim JJ. The development of malignant lymphoma in the course of Sjögren's syndrome. American Journal of Medicine. 1964;36(4):529-540. — doi:10.1016/0002-9343(64)90101-9 (PMID: 14142406)
- Clark G, Reichlin M, Tomasi TB. Characterization of a soluble cytoplasmic antigen reactive with sera from patients with systemic lupus erythematosus. Journal of Immunology. 1969;102(1):117-122. — Search PubMed
- Bloch KJ, Buchanan WW, Wohl MJ, Bunim JJ. Sjögren's syndrome: a clinical, pathological, and serological study of sixty-two cases. Medicine (Baltimore). 1965;44:187-231. — Search PubMed
- Mavragani CP, Moutsopoulos HM. Sjögren's syndrome: old and new therapeutic targets. Journal of Autoimmunity. PubMed: Sjögren autoimmune exocrinopathy (Mavragani & Moutsopoulos)
- Murube J. Henrik Sjögren, 1899–1986. The Ocular Surface. 2010. PubMed: Murube — Henrik Sjögren biography
- Historical review — Sjögren's before Sjögren: did Henrik Sjögren (1899–1986) really discover Sjögren's disease? PubMed: history of Sjögren's — Hadden, Mikulicz, Gougerot
- Two men, four syndromes — the Sjögren surname (Henrik vs. Torsten Sjögren). — PubMed: Sjögren — unique surname, two men, four syndromes (PMID 38653487)
- Anti-Ro/SSA and anti-La/SSB antigen-antibody systems — history and significance. PubMed: anti-Ro/SSA and anti-La/SSB autoantibodies
- Shiboski CH, et al. 2016 ACR-EULAR classification criteria for primary Sjögren's syndrome. Arthritis & Rheumatology. 2017;69(1):35-45. — doi:10.1002/art.39859
- 2023 International Rome consensus for the nomenclature of Sjögren disease. PubMed: 2023 Rome nomenclature consensus (Sjögren disease)
- Mikulicz disease, lymphoepithelial sialadenitis, and the Sjögren spectrum. PubMed: Mikulicz disease and the Sjögren / IgG4 spectrum
- Lymphoma risk and B-cell lymphoproliferation in primary Sjögren's syndrome. PubMed: Sjögren's syndrome and non-Hodgkin lymphoma risk
- Primary versus secondary Sjögren's syndrome — concept and history. PubMed: primary vs. secondary Sjögren's classification
- Gougerot-Sjögren syndrome — the French historical attribution. PubMed: Gougerot-Sjögren syndrome (French literature)
External Authoritative Resources
- NINDS (NIH) — Sjögren's Syndrome Information
- MedlinePlus — Sjögren's Syndrome
- PubMed — History of Sjögren's Syndrome
Connections
- Rheumatology
- Sjögren's Syndrome (Overview)
- All Conditions
- Lupus (Systemic Lupus Erythematosus)
- Arthritis
- Raynaud's Disease
- Fibromyalgia
- Hashimoto's Thyroiditis