Axial Spondyloarthritis (nr-axSpA and Ankylosing Spondylitis)
- Overview and the axSpA Spectrum
- Non-Radiographic Axial SpA (nr-axSpA) — Definition and Significance
- ASAS Classification Criteria (2009)
- Pathogenesis: HLA-B27 and Beyond
- Clinical Manifestations
- Extra-Articular Features
- Imaging: MRI Sacroiliitis and Plain Radiography
- Diagnosis and Differential Diagnosis
- Treatment: NSAIDs, Biologics, and Treat-to-Target
- Monitoring and Disease Activity Scores
- References
- Connections
Overview and the axSpA Spectrum
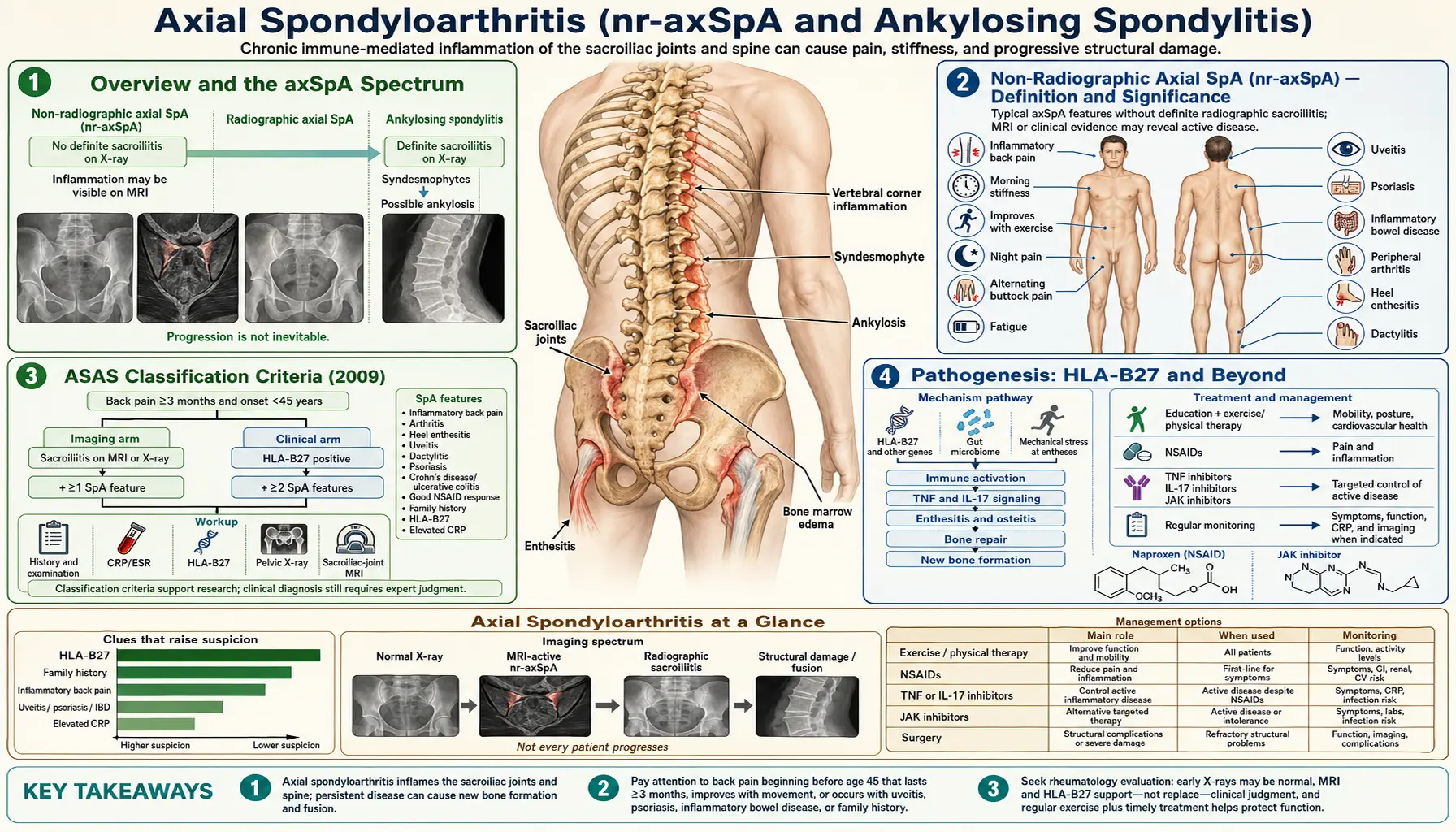
Axial spondyloarthritis (axSpA) is an umbrella term for a spectrum of chronic inflammatory arthritis that predominantly affects the sacroiliac joints and spine. The condition belongs to a broader family of diseases collectively called spondyloarthritis (SpA), which share overlapping features including association with the gene marker HLA-B27, inflammation at entheses (the sites where tendons and ligaments attach to bone), and the tendency to involve the sacroiliac joints. Within the axSpA spectrum, two forms are recognized based on whether joint damage is visible on plain X-rays.
Radiographic axSpA (r-axSpA) corresponds to classical ankylosing spondylitis (AS) — the form in which structural sacroiliac joint damage, such as erosions, sclerosis, and eventual fusion, has become visible on standard pelvic X-rays. Non-radiographic axSpA (nr-axSpA), by contrast, describes the form where characteristic sacroiliac joint inflammation is detectable only by MRI, or is inferred from clinical and laboratory features, without visible X-ray changes meeting the modified New York criteria. This page focuses on both forms as parts of one continuous spectrum, with particular attention to nr-axSpA as the form that remained diagnostically invisible for decades before MRI became standard and dedicated classification criteria were developed.
The distinction between these two forms matters enormously for patients. Under the old modified New York (mNY) criteria for ankylosing spondylitis, which required radiographic evidence of sacroiliitis graded at least 2+ bilaterally or 3+ unilaterally on plain films, patients with equivalent disease burden — identical pain levels, equivalent functional impairment, equivalent systemic inflammation on blood tests, and clear sacroiliac joint inflammation on MRI — were simply not diagnosable. They were labeled "possible AS," "pre-radiographic AS," "undifferentiated SpA," or simply "inflammatory back pain of unknown cause." Many of these patients, a disproportionate number of them women, went five to ten years or longer without a specific diagnosis and without access to the biologic medications (TNF inhibitors, IL-17 inhibitors) that were being prescribed for AS. The 2009 ASAS (Assessment of SpondyloArthritis International Society) classification criteria changed this by creating nr-axSpA as a recognized diagnostic category, enabling earlier and more equitable access to diagnosis and treatment.
The spondyloarthritis family includes several overlapping conditions: axial SpA (both nr-axSpA and AS), psoriatic arthritis, reactive arthritis, enteropathic arthritis associated with inflammatory bowel disease (Crohn's disease and ulcerative colitis), and undifferentiated SpA. All share HLA-B27 association to varying degrees, the tendency toward enthesitis, sacroiliitis, and asymmetric oligoarthritis affecting the lower limbs. The distinction between these entities is not always sharp — a patient with psoriasis and sacroiliitis may qualify as both psoriatic arthritis and axSpA, and management decisions account for the full picture rather than insisting on a single diagnosis.
Non-Radiographic Axial SpA (nr-axSpA) — Definition and Significance
For most of the twentieth century, the working diagnosis for inflammatory back pain centered on ankylosing spondylitis, and AS diagnosis required visible sacroiliac joint damage on a pelvic X-ray. This created a structural blind spot: the inflammatory process driving symptoms in the sacroiliac joints often takes years — sometimes a decade or more — to produce X-ray-visible structural changes. During that entire period, a patient could have active, disabling, objective inflammation at the sacroiliac joints detectable on MRI, elevated C-reactive protein (CRP), HLA-B27 positivity, and classic inflammatory back pain pattern, yet not qualify for an AS diagnosis. Those patients were diagnosed with nr-axSpA — a condition that in retrospect had probably always existed but simply lacked recognition.
The introduction of MRI as a clinical tool for evaluating the sacroiliac joints, particularly using STIR (short tau inversion recovery) sequences sensitive to bone marrow edema, made it possible to see active sacroiliitis before it produced structural X-ray changes. Studies in early inflammatory back pain cohorts revealed that many patients presenting with symptoms highly suggestive of SpA had unambiguous MRI sacroiliitis despite normal or borderline X-rays. These observations drove the development of the ASAS criteria in 2009, which formally incorporated MRI sacroiliitis as an alternative diagnostic pathway to the imaging arm of the criteria, allowing classification of axSpA even without X-ray changes.
A critical point for patients to understand is that the "non-radiographic" designation is a statement about imaging findings — specifically the absence of certain X-ray changes — and emphatically not a statement about disease severity. Studies consistently show that disease burden in nr-axSpA, measured by pain intensity, morning stiffness, functional impairment, fatigue, and quality-of-life metrics, is statistically comparable to that in established AS. Patients with nr-axSpA frequently report years of inadequately treated pain, missed workdays, and reduced physical capacity long before receiving a diagnosis.
The natural history of nr-axSpA is heterogeneous. Approximately 50% of patients classified as nr-axSpA will progress to radiographic axSpA (AS) — visible X-ray sacroiliitis — within 10 to 20 years of follow-up, particularly those who are male, HLA-B27 positive, have elevated CRP, or show active MRI sacroiliitis. The remaining 50% may remain in the nr-axSpA category indefinitely without developing radiographic changes. This variability makes long-term cohort studies challenging and has fueled debate about whether nr-axSpA and AS are truly two stages of a single progressive disease or partially distinct phenotypes. From a treatment standpoint, the distinction has become less critical over time: TNF inhibitors, IL-17 inhibitors, and JAK inhibitors are equally effective in nr-axSpA as in established AS, and regulatory approval now extends to nr-axSpA with objective signs of inflammation (elevated CRP or positive MRI), removing the previous requirement to wait for radiographic damage before initiating biologic therapy.
Women are represented more equitably in nr-axSpA than in AS. Classical AS has a roughly 2–3:1 male-to-female ratio, partly an artifact of the diagnostic criteria requiring radiographic sacroiliitis, since women with AS were consistently shown to progress more slowly to radiographic changes and were therefore underdiagnosed. In nr-axSpA cohorts, the sex ratio approaches 1:1. This normalization likely reflects the removal of the radiographic bottleneck and suggests that the true disease burden of SpA in women was historically underestimated.
ASAS Classification Criteria (2009)
The Assessment of SpondyloArthritis International Society (ASAS) classification criteria for axial SpA, published in 2009 by Rudwaleit and colleagues, apply to patients who have chronic back pain lasting three months or longer with onset before the age of 45. This age cutoff is important because it reflects the typical age of onset for inflammatory SpA and helps distinguish it from degenerative causes of back pain, which become far more common after 45. The criteria provide two separate pathways — the imaging arm and the clinical arm — and meeting either arm classifies a patient as having axSpA.
The imaging arm requires evidence of sacroiliitis either on MRI or on plain X-rays, plus at least one additional SpA feature. For MRI, the specific criterion is active inflammation — bone marrow edema or osteitis in the periarticular subchondral bone of the sacroiliac joints — that is highly suggestive of SpA. The ASAS definition specifies that this finding must be present in at least two consecutive image slices, or if only on a single slice, the lesion must be seen on at least two different locations within that slice. The bone marrow edema must be in the subchondral bone immediately adjacent to the sacroiliac joint — not isolated synovial enhancement, which is less specific. For radiographic sacroiliitis, the mNY criteria apply: grade 2 or higher bilaterally, or grade 3 to 4 unilaterally.
The clinical arm requires HLA-B27 positivity plus at least two SpA features. This arm can classify axSpA even when imaging is normal or inconclusive, recognizing that some patients have objective inflammatory SpA with classic clinical features and positive HLA-B27 but early or mild sacroiliac joint changes not yet detectable by either MRI or X-ray.
The SpA features counted in both arms are: inflammatory back pain; arthritis (past or present); enthesitis — most commonly heel enthesitis (plantar fasciitis or Achilles tendon insertion); anterior uveitis (past or present); dactylitis; psoriasis (past or present); inflammatory bowel disease, meaning Crohn's disease or ulcerative colitis (past or present); good response to NSAIDs, meaning marked improvement in back pain within 48 hours of a full anti-inflammatory dose; family history of SpA in a first- or second-degree relative; HLA-B27 positivity; and elevated CRP in the context of back pain after other causes have been excluded.
These criteria were designed and validated for classification — for use in clinical trials and cohort studies — rather than as a standalone diagnostic algorithm for individual patients in clinical practice. In practice, rheumatologists make diagnostic judgments based on the full clinical picture, recognizing that false positives and false negatives occur with any set of criteria. MRI findings in particular require careful interpretation: bone marrow edema in the sacroiliac joints can appear in other conditions (e.g., osteitis condensans ilii, infection, metabolic bone disease) and in healthy individuals after intense exercise or during and after pregnancy. The pattern, distribution, and combination with clinical features determines diagnostic weight.
Pathogenesis: HLA-B27 and Beyond
HLA-B27 is the strongest single genetic risk factor for axSpA and has been associated with the disease since 1973. The gene is present in approximately 80–95% of patients with ankylosing spondylitis and approximately 65–75% of patients with nr-axSpA, compared with 6–8% of the general population in most Western countries and less than 1% in some Asian and African populations. Despite this striking association, only 1–5% of HLA-B27-positive individuals ever develop axSpA, confirming that HLA-B27 is necessary but far from sufficient. Multiple other genetic loci contribute to risk — genome-wide association studies have identified variants in ERAP1 (endoplasmic reticulum aminopeptidase 1), IL23R, IL12B, PTGER4, and dozens of other loci — and environmental triggers, particularly infections and gut microbiome alterations, appear to play an essential initiating role.
Three main hypotheses have been advanced to explain how HLA-B27 promotes SpA. The arthritogenic peptide hypothesis proposes that HLA-B27 presents specific bacterial- or self-derived peptides to CD8+ cytotoxic T lymphocytes, triggering an autoimmune attack on joint tissue. Candidate peptides from gut bacteria have been identified in animal models, and the hypothesis is supported by the observation that germ-free HLA-B27 transgenic rats do not develop SpA unless colonized with normal gut flora. The misfolding hypothesis proposes that HLA-B27 heavy chains have an unusual tendency to misfold in the endoplasmic reticulum (ER), triggering the unfolded protein response (UPR) and ER stress, which in turn activates IL-23 and downstream IL-17 production by myeloid and innate immune cells, independent of classic antigen presentation. The homodimer hypothesis proposes that misfolded HLA-B27 forms homodimers on the cell surface that interact with KIR3DL2 and other natural killer cell receptors, activating NK cells and promoting IL-17 production.
The IL-23/IL-17 axis is the dominant inflammatory pathway in axSpA regardless of which upstream mechanism initiates it, and this understanding has driven the development of effective biologics. IL-23 (produced by myeloid dendritic cells and macrophages) drives differentiation and activation of Th17 cells and innate lymphoid cells, which produce IL-17A and IL-17F. IL-17A in turn drives neutrophil recruitment, osteoclast activation, and synovial and entheseal inflammation. TNF-alpha is a parallel and equally important effector cytokine: it drives synovial inflammation, bone destruction, and systemic manifestations including fatigue, fever, and anemia of chronic disease.
The enthesis — the site where tendons, ligaments, and joint capsules insert into bone — is the primary anatomical target in axSpA. Entheses are mechanically stressed and relatively avascular tissues with sparse immune surveillance, and they harbor a population of innate immune cells (macrophages, mast cells, and resident T cells) that can initiate inflammation when activated by stress signals or microbial products. Entheseal inflammation at the sacroiliac joints and spinal ligaments produces the characteristic MRI findings of bone marrow edema and, over time, structural damage including erosions, fatty replacement of bone marrow, and new bone formation.
New bone formation — the process driving syndesmophyte growth and eventual spinal ankylosis in established AS — is mediated by Wnt signaling and bone morphogenetic proteins (BMPs) and appears to be partially independent of ongoing inflammation. This uncoupling of inflammation from bone formation has important therapeutic implications: anti-inflammatory biologics that dramatically suppress MRI inflammation and symptoms may not fully prevent radiographic progression, and patients with long-standing uncontrolled inflammation may continue to develop syndesmophytes even after starting effective biologic therapy. Continuous NSAID therapy, which may partially inhibit new bone formation through prostaglandin-dependent pathways, remains the only strategy with some evidence for slowing radiographic progression in AS, though the evidence base is limited and inconsistent.
Gut inflammation plays a larger role in axSpA than was previously appreciated. Subclinical gut inflammation detectable on ileocolonoscopy is present in approximately 30–50% of patients with established AS, even in the absence of overt IBD symptoms. Gut dysbiosis — alterations in the composition of the intestinal microbiome — has been documented in SpA cohorts, with relative depletion of Faecalibacterium prausnitzii and enrichment of pro-inflammatory Prevotella species. The "gut-joint axis" is now a central theme in SpA research, and the mutual overlap between axSpA and IBD (5–10% of axSpA patients develop clinical IBD; 20–30% of IBD patients have subclinical sacroiliitis) underscores the biological connection.
Clinical Manifestations
The hallmark presentation of axSpA is inflammatory back pain (IBP) — a constellation of features that distinguishes it from the far more common mechanical low back pain. Inflammatory back pain is characterized by insidious onset over weeks to months (rather than sudden onset after an injury or activity), age of onset before 45, duration longer than three months, morning stiffness lasting 45 minutes or more, pain that is worse with rest and improves with activity, and pain that frequently wakes the patient in the second half of the night — typically around 3–5 am — and forces them to get up and move around. Alternating buttock pain — pain that shifts from the left buttock to the right buttock and back over days or weeks — is a particularly specific feature, reflecting inflammation in the sacroiliac joints on alternating sides. This pattern is foreign to mechanical back pain, where pain is typically worse with activity and loading, improved with rest, does not improve with exercise, and does not cause nocturnal awakening.
The Calin criteria (1977) and the Berlin criteria (2006) formalized the definition of inflammatory back pain for research purposes; the ASAS 2009 IBP criteria require at least 4 of 5 features: age at onset younger than 40 years, insidious onset, improvement with exercise, no improvement with rest, and pain at night (with improvement on getting up). In clinical practice, the presence of even two or three of these features in a young patient with chronic back pain should trigger consideration of axSpA and referral to rheumatology.
Sacroiliitis is the cardinal anatomical finding. Clinically it produces deep buttock pain, often unilateral or alternating, that may radiate to the posterior thigh and occasionally to the heel. This can mimic sciatica from lumbar disc herniation, but SpA-related pain characteristically does not radiate below the knee and is not worsened by coughing or Valsalva maneuver. Physical examination findings include direct tenderness over the sacroiliac joints (palpated just medial to the posterior superior iliac spine), pain provoked by FABER (Flexion-ABduction-External Rotation, also called Patrick's test) and FADIR (Flexion-ADduction-Internal Rotation) maneuvers, and positive Gaenslen's test. These provocative tests lack specificity individually but, in context, support sacroiliac involvement.
Spinal involvement in axSpA produces morning stiffness throughout the entire spine — cervical, thoracic, and lumbar — reduced range of motion in all planes, and reduced chest expansion from costovertebral joint inflammation. The Schober test assesses lumbar flexion: a mark is placed at the level of the posterior superior iliac spines (L5) and 10 cm above; on maximal forward flexion, less than 5 cm of increase in this distance (from 10 to 15 cm) indicates reduced lumbar mobility. Cervical rotation in each direction and lateral flexion are also assessed. Chest expansion less than 5 cm measured at the fourth intercostal space during maximal inspiration indicates thoracic cage restriction from costovertebral joint inflammation — this is both a diagnostic clue and a functional impairment measure. In advanced AS, fixed kyphosis and fusion of the cervical spine create the characteristic "question mark" posture and severely restrict the visual field.
Peripheral arthritis occurs in approximately 30–40% of axSpA patients. It is characteristically oligoarticular (fewer than five joints), asymmetric, and predominantly affects large joints of the lower limbs — knees, ankles, and hips — rather than the small joints of the hands and feet (which distinguishes it from rheumatoid arthritis). Hip involvement occurs in roughly 25% of patients and carries particular importance because hip arthritis is a major driver of disability, functional impairment, and ultimately total hip replacement. Early hip involvement, especially in young patients with AS, is an indication for more aggressive treatment. Shoulder involvement is less common but occurs, particularly in women.
Enthesitis — inflammation at tendon and ligament insertion sites — is a defining feature of SpA. The most common sites are the plantar fascia insertion at the calcaneus (plantar heel pain, often confused with simple plantar fasciitis), the Achilles tendon insertion at the posterior calcaneus (posterior heel pain), the costochondral junctions (chest pain that worsens on deep breathing or palpation, easily misattributed to musculoskeletal or cardiac causes), the quadriceps tendon insertion at the superior pole of the patella, and the iliac crest. Systematic examination of entheses using the MASES (Maastricht Ankylosing Spondylitis Enthesitis Score) identifies 13 sites; widespread enthesitis at multiple sites on examination is a hallmark of active SpA and distinguishes it from localized overuse enthesopathies.
Dactylitis — diffuse swelling of an entire finger or toe producing the "sausage digit" appearance — results from combined tenosynovitis, arthritis, and periarticular edema involving the entire digital ray. Dactylitis is more common in psoriatic arthritis than in pure axSpA but can occur in any SpA subtype. Its presence on examination is a strong clinical indicator of SpA and should prompt a systematic SpA evaluation including HLA-B27, sacroiliac imaging, and skin/nail examination for psoriasis.
Extra-Articular Features
Anterior uveitis (acute iritis) is the most common extra-articular manifestation of axSpA, occurring in 20–40% of patients at some point during their disease course. It presents acutely with unilateral eye pain, redness, photophobia, and blurred vision. The attack is typically self-limited but recurs, often in the same eye, and can cause significant visual morbidity including posterior synechiae, cataract, and, if inadequately treated, glaucoma and vision loss. HLA-B27-associated uveitis tends to be anterior, acute, and unilateral (alternating eyes over successive episodes), in contrast to the bilateral, chronic, granulomatous uveitis of sarcoidosis. Any patient with a history of recurrent acute anterior uveitis should be evaluated for axSpA regardless of whether back pain has been prominently reported — uveitis can precede or develop independent of articular symptoms. Management requires urgent ophthalmology evaluation, topical corticosteroids (prednisolone acetate drops hourly acutely), and cycloplegics to prevent synechiae. An important prescribing nuance is that etanercept (a TNF receptor fusion protein) is substantially less effective than the monoclonal anti-TNF agents (infliximab, adalimumab, golimumab, certolizumab) for preventing uveitis recurrence. Patients with frequent or severe uveitis should preferentially receive a monoclonal anti-TNF agent.
Psoriasis occurs in approximately 10% of axSpA patients. When extensive or plaque psoriasis is present, the diagnosis may shift toward psoriatic arthritis (PsA) as the primary classification, since PsA has its own management nuances (particularly the use of IL-17 and IL-23 inhibitors that are also highly effective for skin disease). Nail psoriasis — pitting, onycholysis, oil spots — is particularly associated with joint involvement and should be looked for at examination even when skin disease appears mild.
Inflammatory bowel disease occurs in 5–10% of axSpA patients (Crohn's disease more than ulcerative colitis), and conversely, 20–30% of IBD patients have subclinical or symptomatic sacroiliitis or peripheral SpA. This overlap has pharmacological implications: IL-17 inhibitors (secukinumab, ixekizumab), while highly effective for axSpA and psoriasis, are contraindicated in IBD because they can paradoxically worsen intestinal inflammation. When a patient has both axSpA and IBD, treatment with a TNF monoclonal antibody — infliximab, adalimumab, or golimumab, all of which are approved for both conditions — is the preferred biologic choice. IL-12/23 inhibitors (ustekinumab) and JAK inhibitors (tofacitinib, upadacitinib) may also be used in the IBD+SpA overlap context, with ongoing study.
Cardiac involvement in long-standing AS includes aortitis, aortic regurgitation from aortic root dilation, and conduction abnormalities including varying degrees of atrioventricular block. These complications are generally associated with decades of active disease in established AS rather than with early axSpA or nr-axSpA, but their existence underscores the importance of long-term disease control. Aortic regurgitation in a young or middle-aged patient with chronic back pain should always raise the question of undiagnosed AS. Regular cardiac auscultation and periodic ECG in patients with long-standing AS are reasonable practice.
Osteoporosis and fracture represent underappreciated risks. Vertebral bone density is reduced even in early axSpA, driven by inflammatory cytokines (TNF, IL-17) promoting osteoclast activity that outpaces compensatory new bone formation at the disc-end plate interface. Paradoxically, DXA measurements at the lumbar spine may appear falsely elevated in established AS because syndesmophytes and perivertebral ossification increase measured bone density even as trabecular bone within vertebral bodies is reduced. Femoral neck and total hip measurements are more reliable. In advanced AS with a fused, rigid "bamboo spine," even minor trauma — a fall from standing, an unexpected jolt — can cause catastrophic unstable cervical fractures because the ankylosed spine transmits force like a rigid long bone rather than absorbing it through intervertebral motion. Patients with advanced AS should be counseled about fracture risk, instructed to avoid contact sports and high-fall-risk activities, and considered for bisphosphonate therapy if DXA T-scores are below –2.5.
Imaging: MRI Sacroiliitis and Plain Radiography
Imaging is central to both the diagnosis and monitoring of axSpA, and understanding what each modality does and does not show is essential for interpreting results in clinical practice.
MRI of the sacroiliac joints is the key diagnostic modality for nr-axSpA. The STIR (short tau inversion recovery) sequence is used without contrast and is highly sensitive for bone marrow edema — bright signal in the periarticular subchondral bone of the sacroiliac joints reflecting active inflammation (osteitis). Gadolinium-enhanced T1-weighted images show synovial enhancement and can supplement STIR when equivocal, but STIR is usually sufficient for diagnostic purposes. Fat-suppressed T2 sequences are an alternative. The critical finding is bone marrow edema in the subchondral bone immediately adjacent to the sacroiliac joint surfaces, not simply periarticular soft tissue signal or isolated synovial enhancement. Importantly, some degree of bone marrow edema at the sacroiliac joints can be seen in healthy individuals after intensive physical activity, during and after pregnancy, and in osteitis condensans ilii — the finding must be interpreted in the full clinical context. Active inflammation per ASAS definition requires edema in at least two consecutive MRI slices, or a single lesion present in at least two separate locations within the sacroiliac joint on a single slice.
MRI also identifies structural lesions indicating prior inflammation and damage: erosions appear as loss of low-signal cortical bone on T1-weighted images with subchondral signal abnormality; fat metaplasia (fatty lesions) appears as T1-bright signal replacing normal marrow, indicating post-inflammatory repair; and ankylosis appears as bridging of the joint space by fatty or bony tissue. Structural lesions on MRI are evidence of prior SpA activity and support the diagnosis even in the absence of active edema — for instance, in a patient treated with a biologic whose active inflammation has been suppressed but whose sacroiliac joints show erosions and fat metaplasia from prior disease.
MRI of the spine (STIR sagittal sequences through the cervical, thoracic, and lumbar spine) identifies vertebral corner inflammatory lesions (Romanus lesions) — bone marrow edema at the anterior corners of vertebral bodies where the disc annulus inserts — and facet joint inflammation. These findings support active spinal axSpA and can help assess disease extent and treatment response.
Plain X-ray of the pelvis (anteroposterior view) provides the modified New York grading of sacroiliitis. Grade 0 is normal. Grade 1 is suspicious changes without definite abnormality. Grade 2 (minimum) shows small localized areas with erosion or sclerosis without alteration in the joint width. Grade 3 (moderate) shows erosions, sclerosis, widening or narrowing of the joint space, or partial ankylosis. Grade 4 (severe/ankylosed) shows complete fusion of the sacroiliac joint. The mNY criteria for AS require grade 2 or higher bilaterally or grade 3 to 4 unilaterally. X-ray sacroiliitis at the level required by mNY criteria typically represents at least several years of structural damage and is therefore absent in the early phase of the disease.
Spine radiographs assess for syndesmophytes — thin, vertical bony outgrowths from the anterior (and later posterior) corners of vertebral end plates, growing within the annulus fibrosus to eventually bridge adjacent vertebrae. Syndesmophytes are a defining feature of AS and distinguish it from degenerative osteophytes (which originate from the vertebral body edge and grow horizontally before hooking upward). Progressive syndesmophyte formation leads to the "bamboo spine" in severe long-standing AS — complete fusion of the entire thoracolumbar spine visible on plain film as continuous posterior and anterior ossification. The modified Stoke Ankylosing Spondylitis Spine Score (mSASSS) quantifies radiographic spinal progression and is used in clinical trials.
CT of the sacroiliac joints offers superior bony detail — superior to X-ray for detecting erosions and subtle structural changes — and is particularly valuable when plain films are equivocal and MRI is unavailable or contraindicated. Its significant radiation dose limits its use to specific clinical questions, particularly suspected unstable fracture through an ankylosed cervical spine after trauma, where CT is the imaging of choice.
Ultrasound can identify enthesitis (power Doppler signal at entheseal insertions, thickening, calcification) at peripheral sites such as the Achilles, plantar fascia, and quadriceps tendons. It is not used for sacroiliac joint assessment but can contribute to the diagnostic picture and monitor peripheral enthesitis response to treatment.
Diagnosis and Differential Diagnosis
Diagnosing axSpA requires synthesizing clinical features, laboratory findings, imaging, and — critically — excluding other conditions that can mimic it. The average diagnostic delay from symptom onset to diagnosis remains 5–10 years in many countries, driven by the prevalence of mechanical low back pain, lack of awareness of inflammatory back pain features among primary care providers, and the subtle early appearance of axSpA on X-rays. Shortening this delay is a primary goal of current education and referral pathway initiatives.
Laboratory evaluation should include HLA-B27 typing, CRP, ESR, complete blood count, comprehensive metabolic panel, urinalysis, and — to exclude mimics — ANA, RF, and anti-CCP. HLA-B27 is positive in approximately 80–90% of AS and 65–75% of nr-axSpA; a positive result in a young patient with inflammatory back pain substantially raises the pre-test probability and supports the diagnosis, while a negative result in a patient with classic clinical features and MRI sacroiliitis does not exclude axSpA. CRP and ESR are elevated in approximately 50% of axSpA patients overall; a normal CRP does not exclude active disease. ANA, RF, and anti-CCP are typically negative in axSpA (the "seronegative" designation) and their presence should prompt consideration of an overlap syndrome or an alternative diagnosis. Urine analysis and renal function are relevant because long-term NSAID use (common in axSpA management) carries nephrotoxic risk and chronic inflammation can cause secondary amyloidosis affecting the kidneys in very long-standing AS.
The differential diagnosis includes several conditions that can closely mimic axSpA. Mechanical low back pain is the most common and important distinction: mechanical pain typically has an identifiable precipitant (lifting, twisting), is worse with activity and loading, improves with rest, does not cause nocturnal awakening, and improves with NSAIDs at analgesic rather than anti-inflammatory doses. MRI in mechanical LBP may show disc degeneration, disc herniation, or facet arthropathy without sacroiliac joint edema. Diffuse idiopathic skeletal hyperostosis (DISH) produces flowing osteophytes bridging vertebral bodies that can superficially resemble syndesmophytes, but DISH involves the anterolateral vertebral body (right side of the thoracic spine predominantly), does not involve the sacroiliac joints, and occurs in older, often obese patients without systemic inflammation. Osteitis condensans ilii (OCI) produces bilateral triangular sclerosis on the iliac side of the sacroiliac joints, typically in young women during or after pregnancy, and can be mistaken for sacroiliac joint inflammation on X-ray; it causes no erosions, no joint space change, and MRI does not show active bone marrow edema in the articular cartilage zone. Infectious sacroiliitis is typically unilateral, presents with severe focal tenderness and systemic features of infection (fever, elevated WBC, positive blood cultures or aspirate), and the MRI shows more dramatic periarticular soft tissue edema and abscess formation than inflammatory SpA. Spondylodiscitis (vertebral osteomyelitis) presents with focal spine pain, fever, elevated inflammatory markers, and MRI showing disc and vertebral body signal abnormalities; blood cultures and disc aspirate are required. Fibromyalgia causes widespread musculoskeletal pain, fatigue, and sleep disturbance but has normal MRI, normal CRP, and normal joint examination — fibromyalgia and SpA are not mutually exclusive and can coexist, complicating disease activity assessment.
Treatment: NSAIDs, Biologics, and Treat-to-Target
Non-steroidal anti-inflammatory drugs (NSAIDs) are the first-line pharmacological treatment for axSpA, used at full anti-inflammatory doses — not the lower analgesic doses used for pain relief in mechanical conditions. Any NSAID can be used: naproxen 500 mg twice daily, indomethacin 50 mg three times daily (most potent, more side effects), celecoxib 200 mg twice daily (selective COX-2 inhibitor with reduced GI toxicity), or diclofenac 75 mg twice daily. The test of an adequate NSAID trial is clinically important: a two-week trial at full anti-inflammatory dose is typically required before concluding that NSAIDs are inadequate. Patients with classical AS frequently report dramatic, near-complete relief of morning stiffness and pain within hours to a few days of a full NSAID dose — a response so characteristic that it is one of the SpA features in the ASAS classification criteria. Failure of two different NSAIDs at full anti-inflammatory dose is the primary trigger for escalation to biologic therapy in most guidelines.
The question of continuous versus on-demand NSAID use has practical importance. In established AS, some evidence from imaging studies suggests that continuous daily NSAID use may retard syndesmophyte formation and radiographic progression compared with on-demand use, by suppressing the prostaglandin-dependent bone formation pathways. However, the evidence base is limited — primarily from one randomized controlled trial showing slowed radiographic progression with continuous celecoxib — and the benefit must be weighed against the cumulative GI, renal, and cardiovascular risks of long-term daily NSAID use. For patients with nr-axSpA, where syndesmophyte formation is not yet established, the balance of benefits and risks generally favors on-demand use unless symptoms require continuous therapy for quality of life.
Physical therapy, exercise, and lifestyle are not optional adjuncts in axSpA — they are core treatments with evidence of sustained, meaningful benefit on pain, stiffness, and function that is independent of pharmacological management. Disease-specific exercises include axial stretching targeting spinal flexibility (daily thoracic extension over a roll, cervical rotation and side-bending), chest expansion exercises (deep breathing against resistance), strengthening of postural muscles, and aerobic conditioning. Swimming is ideal because the buoyancy unloads the spine while allowing full range of motion exercise. Group hydrotherapy programs and supervised weekly exercise classes for AS patients (offered in many European countries) have demonstrated significant improvements in functional indices in randomized controlled trials. Physical therapy should be established early, reviewed periodically, and maintained as a lifelong habit — the effect of exercise is lost if it is discontinued.
Biologic therapy is indicated when symptoms remain active (BASDAI ≥4, or ASDAS ≥2.1) despite adequate NSAID therapy and physiotherapy. For nr-axSpA specifically, the additional requirement of objective evidence of inflammation — elevated CRP or active MRI sacroiliitis — is applied before biologic initiation in most regulatory frameworks, reflecting the recognition that some patients classified as nr-axSpA by clinical criteria alone may not have truly inflammatory disease. The available biologic and targeted synthetic DMARDs for axSpA include:
TNF inhibitors were the first biologics approved for axSpA and remain widely used. Five agents are approved: adalimumab (Humira, subcutaneous every two weeks), etanercept (Enbrel, subcutaneous weekly), infliximab (Remicade, intravenous every 6–8 weeks), golimumab (Simponi, subcutaneous monthly or IV), and certolizumab pegol (Cimzia, subcutaneous every two or four weeks). All five produce rapid, substantial reductions in inflammatory back pain, morning stiffness, CRP, and MRI sacroiliitis, and all are approved for both AS (r-axSpA) and nr-axSpA. Certolizumab pegol has the additional approval of being considered appropriate during pregnancy (it lacks the Fc region that crosses the placenta and is negligibly transmitted in breast milk), which is clinically important given that axSpA frequently affects women of childbearing age. The key prescribing distinction among TNF inhibitors is for uveitis: etanercept is consistently less effective for preventing uveitis recurrence than the monoclonal antibodies (adalimumab, infliximab, golimumab, certolizumab). Patients with frequent or severe uveitis should receive a monoclonal anti-TNF agent.
IL-17 inhibitors — secukinumab (Cosentyx, subcutaneous monthly after loading) and ixekizumab (Taltz, subcutaneous every four weeks) — target the IL-17A pathway that is central to entheseal and spinal inflammation in axSpA. Both are approved for AS; secukinumab is approved for nr-axSpA (with MRI evidence of inflammation) in the US and EU, and ixekizumab has data supporting efficacy in this population (SELECT-AXIS 2 trial). IL-17 inhibitors are particularly attractive when psoriasis is prominent (superior skin efficacy compared with TNF inhibitors) and may be preferred in patients who have failed a TNF inhibitor. The critical contraindication is IBD: IL-17 inhibition can paradoxically exacerbate Crohn's disease and ulcerative colitis, and these agents should not be used in patients with IBD comorbidity.
JAK inhibitors represent the most recent addition to axSpA treatment. Tofacitinib (Xeljanz) and upadacitinib (Rinvoq) are approved for AS; upadacitinib demonstrated efficacy in nr-axSpA in the SELECT-AXIS 2 trial. The principal advantages are oral administration (convenience, no injection) and rapid onset of action. Safety considerations include increased risk of herpes zoster (shingles — vaccination recommended before initiation), and the FDA and EMA have issued warnings regarding cardiovascular events and malignancy based on post-marketing data from a tofacitinib comparator trial in rheumatoid arthritis; these concerns have led to cautious prescribing in patients with cardiovascular risk factors, prior malignancy, or thromboembolism history. Filgotinib (Jyseleca) and baricitinib have data in AS with varying regional approval status.
Conventional synthetic DMARDs — methotrexate, sulfasalazine, hydroxychloroquine — have no proven efficacy for axial disease in axSpA and are not recommended for this indication. Sulfasalazine (2–3 g daily) may provide modest benefit for peripheral joint arthritis and enthesitis in SpA and is sometimes used as a bridge or adjunct in patients with predominantly peripheral disease who are not yet biologic candidates, but it should not be used as a substitute for biologic therapy in patients with significant axial disease.
When switching therapies, the distinction between primary non-response (inadequate clinical improvement after three months on a full therapeutic dose) and secondary failure (initial response with subsequent loss of efficacy) guides next steps. Primary non-response to one TNF inhibitor is an indication to consider switching to a different class (IL-17 inhibitor or JAK inhibitor) rather than cycling within TNF inhibitors. Secondary failure may reflect immunogenicity (anti-drug antibodies) and can sometimes be addressed by adding methotrexate as an anti-immunogenicity strategy, though this is more established in rheumatoid arthritis than in axSpA, or by switching to a different TNF inhibitor or a different class.
Monitoring and Disease Activity Scores
Monitoring axSpA requires combining patient-reported outcomes, objective physical measures, laboratory tests, and periodic imaging. The goal is to assess whether disease is adequately controlled and to document the impact of treatment changes. Two validated composite disease activity scores are used in practice: BASDAI and ASDAS.
The BASDAI (Bath Ankylosing Spondylitis Disease Activity Index) is a self-administered patient questionnaire consisting of six questions, each scored on a 0–10 visual analog scale: (1) overall fatigue or tiredness; (2) overall level of AS neck, back, or hip pain; (3) overall level of pain and swelling in joints other than neck, back, and hips; (4) overall discomfort from tenderness to touch or pressure in any area; (5) overall level of morning stiffness since waking; and (6) duration of morning stiffness (scored 0–10 where 10 = two hours or more). The score is calculated as the mean of questions 1–4 plus the mean of questions 5 and 6, divided by 2; the result ranges from 0 to 10. A BASDAI score of 4 or greater is the commonly used threshold for active disease, and a BASDAI of 4 or greater despite full NSAID therapy is the primary criterion for biologic initiation in most national and international guidelines including the ASAS-EULAR recommendations. BASDAI is entirely patient-reported and carries no objective component, which is both its strength (captures patient experience) and its limitation (cannot distinguish active inflammatory disease from nociplastic pain, fibromyalgia, or other non-inflammatory sources of symptoms).
The ASDAS (Ankylosing Spondylitis Disease Activity Score) incorporates both patient-reported items and the objective acute-phase reactant CRP (or ESR as an alternative). The ASDAS-CRP formula includes questions from the BASDAI (questions 2, 3, and 5 — back pain, peripheral pain, and morning stiffness) plus the patient's global disease activity assessment and CRP in mg/L. ASDAS disease state thresholds are: inactive disease (remission) below 1.3; low disease activity 1.3–2.1; high disease activity 2.1–3.5; very high disease activity above 3.5. Minimum clinically important difference (MCID) is a change of 1.1 or more; major improvement is a change of 2.0 or more. ASDAS is preferred over BASDAI for monitoring by ASAS because it incorporates objective inflammation, making it more sensitive to treatment response and less susceptible to inflation by non-inflammatory pain or mood effects.
The treat-to-target strategy, formally recommended in the 2018 ASAS-EULAR recommendations updated by Smolen and colleagues, specifies that the treatment target should be clinical remission (ASDAS below 1.3) or, if remission is not achievable due to treatment failure or comorbidities, at minimum low disease activity (ASDAS below 2.1). Disease activity should be measured and documented at every clinical visit, with a formal assessment of whether the target is being met. During active disease or treatment adjustment, visits should occur every 3 months; once the target is sustained, reassessment every 6 months is appropriate. This structured approach shifts axSpA management from symptom-reactive prescribing to proactive, goal-directed care — the same philosophy applied successfully in rheumatoid arthritis.
Additional validated instruments include the BASFI (Bath Ankylosing Spondylitis Functional Index), a 10-item patient-reported measure of physical function (ability to perform everyday tasks such as putting on socks, bending to pick up a pen, reaching a high shelf), and the BASMI (Bath Ankylosing Spondylitis Metrology Index), a five-item physical examination measure of spinal mobility (cervical rotation, lumbar side flexion, modified Schober test, tragus-to-wall distance, and intermalleolar distance). These instruments capture dimensions of disease impact — function and mobility — that composite disease activity scores do not fully reflect.
For imaging follow-up, MRI of the sacroiliac joints is used in clinical practice primarily for diagnostic clarification and for documenting treatment response in patients where the clinical picture is uncertain. Routine MRI surveillance in patients with established diagnosis and stable symptoms is not standard practice. X-rays of the spine are performed every 2 years in patients with established AS to monitor syndesmophyte development and radiographic progression. DXA bone density measurement is recommended at baseline and every 2 years given the elevated osteoporosis risk in axSpA, with the caveat that lumbar spine measurements are unreliable in patients with established syndesmophytes or facet joint fusion — lateral DXA or femoral neck measurements should be used instead. Screening echocardiography for aortic regurgitation and ECG for conduction disease is recommended in long-standing AS, particularly in patients with disease duration exceeding 10 years.
References
- Rudwaleit M, van der Heijde D, Landewé R, et al. The development of Assessment of SpondyloArthritis International Society (ASAS) classification criteria for axial spondyloarthritis. Ann Rheum Dis. 2009;68(6):777–783. — Search PubMed
- Sieper J, Rudwaleit M, Baraliakos X, et al. The Assessment of SpondyloArthritis International Society (ASAS) handbook: a guide to assess spondyloarthritis. Ann Rheum Dis. 2009;68(Suppl 2):ii1–44. — Search PubMed
- van der Heijde D, Ramiro S, Landewé R, et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann Rheum Dis. 2017;76(6):978–991. PMID: 28087505
- Deodhar A, Poddubnyy D, Pacheco-Tena C, et al. Efficacy and safety of ixekizumab in the treatment of radiographic axial spondyloarthritis (SELECT-AXIS 2). Arthritis Rheumatol. 2022;74(9):1600–1609. — Search PubMed
- Strand V, Rao SA, Shillington AC, Cifaldi MA, McGuire M, Ruderman EM. Prevalence of axial spondyloarthritis in United States rheumatology practices. Arthritis Care Res (Hoboken). 2013;65(8):1299–1306. — Search PubMed
- Sieper J, Poddubnyy D. Axial spondyloarthritis. Lancet. 2017;390(10089):73–84. PMID: 28110981
- Maksymowych WP, Inman RD, Salonen D, et al. Spondyloarthritis Research Consortium of Canada magnetic resonance imaging index for assessment of sacroiliac joint inflammation in ankylosing spondylitis. Arthritis Rheum. 2005;53(5):703–709. — Search PubMed
- Dougados M, van der Heijde D, Sieper J, et al. Symptomatic efficacy of etanercept and its effects on objective signs of inflammation in early nonradiographic axial spondyloarthritis: a multicenter, randomized, double-blind, placebo-controlled trial. Arthritis Rheumatol. 2014;66(8):2091–2102. — Search PubMed
- Rudwaleit M, Haibel H, Baraliakos X, et al. The early disease stage in axial spondylarthritis: results from the German Spondyloarthritis Inception Cohort (GESPIC). Arthritis Rheum. 2009;60(3):717–727. — Search PubMed
- Haroon NN, Paterson JM, Li P, Haroon N. Increasing proportion of female patients with ankylosing spondylitis: a population-based cohort study. Ann Rheum Dis. 2018;77(9):1300–1305. — Search PubMed
- Smolen JS, Schöls M, Braun J, et al. Treating axial spondyloarthritis and peripheral spondyloarthritis, especially psoriatic arthritis, to target. Ann Rheum Dis. 2018;77(1):3–17. PMID: 28684559
- Poddubnyy D, Hermann KG, Callhoff J, Listing J, Sieper J. Ustekinumab for the treatment of patients with active ankylosing spondylitis: results of a 28-week, prospective, open-label, proof-of-concept study (TOPAS). Ann Rheum Dis. 2014;73(5):817–823. — Search PubMed
Connections
- Rheumatology
- Ankylosing Spondylitis
- Psoriatic Arthritis
- Reactive Arthritis
- Arthritis
- Juvenile Idiopathic Arthritis
- Rheumatoid Arthritis
- Lab Tests
- Lupus