Pneumonia: History and Discovery
Pneumonia is one of the oldest named diseases in medicine. Hippocrates described it around 400 BCE and treated it as a malady already named by “the ancients” before him; the very word comes from the Greek pneumon, meaning lung. For more than two thousand years it could be recognized at the bedside but neither explained nor cured. The story of how pneumonia became understood is really three separate stories — the ancient clinical description of the illness, the nineteenth-century discovery of the microbes that cause it, and the twentieth-century arrival of the antibiotics and vaccines that finally tamed it. Sir William Osler famously called pneumonia the “Captain of the Men of Death.” This page traces, with care for what is documented and what is not, how that captain was first named, then unmasked, and at last largely defeated.
Table of Contents
- Ancient Description: Hippocrates and Peripneumonia
- What the Name Means and Where It Came From
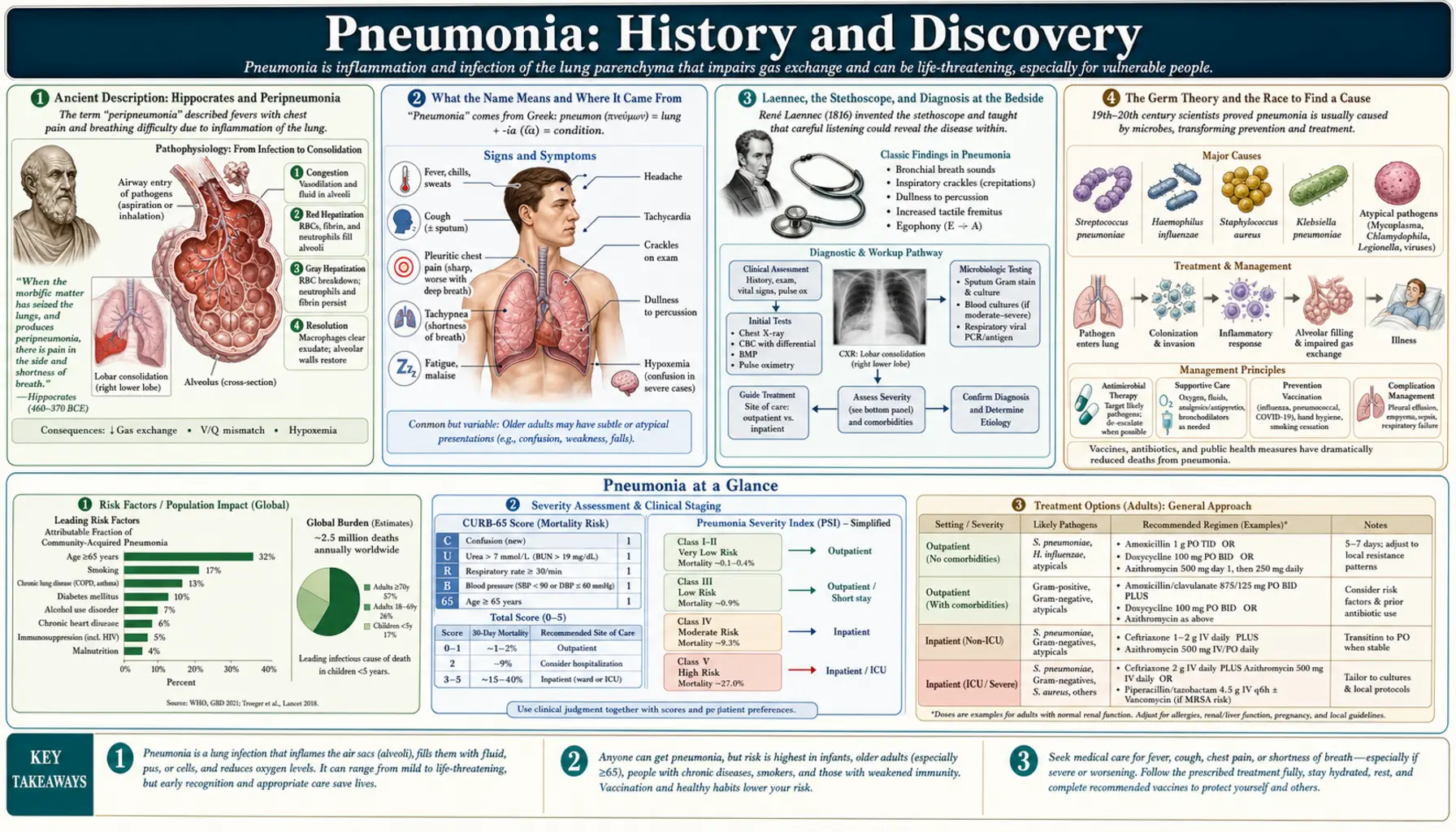
- Laennec, the Stethoscope, and Diagnosis at the Bedside
- The Germ Theory and the Race to Find a Cause
- Isolating the Pneumococcus: 1880–1881
- Friedländer, Fraenkel, and More Than One Culprit
- The “Captain of the Men of Death”
- The Cure: Sulfa Drugs, Penicillin, and Vaccines
- Research Papers and References
- Connections
- Featured Videos
Ancient Description: Hippocrates and Peripneumonia
Pneumonia belongs to the small group of diseases whose clinical picture was recorded with real accuracy in classical antiquity. In the Hippocratic Corpus — the body of medical writings associated with Hippocrates of Kos and his school in the fifth and fourth centuries BCE — the acute febrile illness of the chest is discussed under the name peripneumonia (sometimes rendered “peripneumony”). The Hippocratic physicians grouped pneumonia together with pleurisy because, working without any way to see inside the chest, they found the two extremely difficult to tell apart at the bedside; both produced fever, chest pain, labored painful breathing, and cough. It is important to read this honestly: the ancients described and classified a syndrome they could observe, not a cause they could identify. The notion of an invisible microbe lay more than two millennia in the future.
What the Hippocratic writers got right was the clinical observation. The Aphorisms and related texts describe the diagnosis of peripneumonia and pleuritic conditions through acute fever, pain on one or both sides of the chest, pain on breathing out, cough, and the color of the expectorated sputum, and they paid close attention to which signs boded well or ill for survival. This is recognizable bedside medicine: a careful catalogue of what the disease looks like and how it tends to run its course. These works are named here as historical primary sources rather than as modern citations, but the modern scholarly literature — for example the scoping review of Hippocratic concepts of acute respiratory disease cited below — confirms how detailed and clinically shrewd these ancient descriptions were.
Strikingly, Hippocrates did not claim to have discovered or first named the disease. The Hippocratic and later Greek tradition treats peripneumonia as a malady already recognized and named by earlier physicians — “the ancients” — meaning that the condition was known and labelled before the Hippocratic school itself. Pneumonia, in other words, has no single human discoverer and no datable moment of first description; it is genuinely ancient, recognized as a distinct deadly illness from the very dawn of written medicine. The honest historical statement is that Hippocrates gave us one of the earliest surviving systematic descriptions, not the first description.
What the Name Means and Where It Came From
The English word pneumonia descends directly from Greek. Its root is pneumon (πνευμων), the Greek word for “lung,” which is itself related to pneuma, meaning “breath” or “wind.” A disease of the pneumon is, quite literally, a disease of the lung. The older clinical term peripneumonia — built from the prefix peri- (“around” or “about”) plus the lung root — reflected the ancient uncertainty about exactly which structures around and within the chest were inflamed, since pneumonia and pleurisy were so often seen together. Over the centuries the longer peripneumonia gradually gave way to the simpler pneumonia for inflammation of the lung tissue itself.
This etymology is worth dwelling on because the name encodes the limits of ancient knowledge. The Greeks named the disease for the organ they could reason was affected — the lung — not for any cause, because no cause was knowable to them. Compare this with the much later, mechanism-bearing terms that modern medicine attaches to specific forms of the illness, such as “pneumococcal pneumonia” (named for the bacterium) or “lobar pneumonia” (named for the anatomical pattern of a whole lobe filling with inflammatory exudate). The journey of the vocabulary — from an organ-based Greek name to cause-based and pattern-based modern names — mirrors the journey of understanding itself, from describing the lung that suffered to identifying the microbe responsible and the precise tissue changes it produces.
Laennec, the Stethoscope, and Diagnosis at the Bedside
For more than two thousand years after Hippocrates, a physician faced with a feverish, coughing, breathless patient had little more to work with than the ancient Greek catalogue of signs: inspection of the patient, the pulse, the appearance of the sputum, and the patient’s own account. The first great leap forward in diagnosing pneumonia — as opposed to understanding its cause — came not from a microscope but from a simple wooden tube. In 1816, the French physician René Théophile Hyacinthe Laennec (1781–1826), working at the Necker Hospital in Paris, reportedly rolled a sheet of paper into a cylinder to listen to a patient’s chest, finding that the tube transmitted internal sounds more clearly than pressing his ear directly to the skin. From that improvisation he developed a turned wooden instrument about a foot long, which he called the stethoscope, from the Greek for “chest” (stethos) and “to examine” (skopein).
Between 1816 and 1819 Laennec refined the instrument and, far more importantly, systematically correlated the sounds he heard in living patients with the diseased lungs and hearts he later examined at autopsy. He published this work in 1819 as De l’Auscultation Médiate (“On Mediate Auscultation,” the full title translating as a treatise on the diagnosis of diseases of the lungs and heart). Laennec called his method mediate auscultation — indirect listening through an instrument — in contrast to the older immediate auscultation of placing the ear on the chest. He coined and defined much of the vocabulary chest physicians still use today, including rales (the crackles of fluid-filled airspaces), rhonchi, crepitance, and egophony (the bleating, nasal change in the voice heard over consolidated lung). His treatise contained dedicated discussions of both pneumonia and tuberculosis.
The significance for pneumonia was profound. For the first time, the inflammation and consolidation deep inside the lung produced audible, reproducible signs that a clinician could detect at the bedside in a living patient — the crackling rales of fluid in the alveoli, the changed transmission of the voice over solid lung, the diminished breath sounds of a region filling with exudate. Diagnosis became something more than guesswork from fever and sputum. It is essential to be precise about what Laennec did and did not accomplish: the stethoscope let physicians hear and localize pneumonia with new confidence, but it did nothing to reveal what caused the disease or how to cure it. That second revolution required the germ theory and the microscope, which arrived only after Laennec’s early death from tuberculosis.
The Germ Theory and the Race to Find a Cause
The middle and later nineteenth century brought the single greatest change in the understanding of pneumonia since Hippocrates: the realization that the disease is caused by living microorganisms. The germ theory of disease, advanced above all by Louis Pasteur in France and Robert Koch in Germany, transformed medicine from a discipline that described illnesses into one that could identify their causes. Koch’s demonstration in 1882 that tuberculosis was caused by a specific bacterium — Mycobacterium tuberculosis — showed that even the most common and dreaded chest diseases had discrete microbial agents that could, in principle, be isolated, grown, and ultimately fought. Pneumonia became a natural target for the new science of bacteriology.
An important early clue came in 1875, when the German-Swiss pathologist Edwin Klebs reported observing bacteria in the airways of patients who had died of pneumonia. Observing organisms in diseased tissue, however, is not the same as proving that a particular organism is the cause — the bacteria might be incidental, or contaminants, or secondary invaders. Establishing causation required isolating an organism in pure culture, reproducing the disease, and showing the organism was consistently associated with it — the rigorous logic that Koch was formalizing into his famous postulates during exactly these years. The stage was set for a focused effort to find and prove the cause of the most common form of pneumonia, the lobar pneumonia that filled an entire lobe of the lung with inflammatory exudate.
Isolating the Pneumococcus: 1880–1881
The organism now known as Streptococcus pneumoniae — long called simply the pneumococcus — was first isolated in 1880–1881, and remarkably it was isolated independently and almost simultaneously by two investigators on opposite sides of the Atlantic. In the United States, the U.S. Army physician George Miller Sternberg isolated the organism after injecting his own saliva into rabbits, which sickened and died; he recovered the same diplococcus (a bacterium that grows in pairs) from their blood. In France, Louis Pasteur isolated the same organism at essentially the same time, working with saliva from a child who had died of rabies and likewise inoculating rabbits. Neither man initially grasped that he had captured the chief cause of human pneumonia; each named the new microbe in his own way (Sternberg as Micrococcus pasteuri, Pasteur with a descriptive French term for the microbe of saliva), and the connection to pneumonia was clarified only afterward.
This dual, independent isolation is the carefully documented historical fact, and it is worth stating precisely because popular accounts sometimes credit a single discoverer. Two researchers, in two countries, using similar but separate experiments, captured the same bacterium within roughly a year of each other. The recognition that this diplococcus was the principal agent of lobar pneumonia — and the very name “pneumococcus,” coined for its frequent recovery from the lungs of pneumonia patients — came a few years later, around 1886, in the work of others (notably Albert Fraenkel, discussed below). The bacterium was given its modern scientific name Diplococcus pneumoniae in the early twentieth century and was finally reclassified as Streptococcus pneumoniae in 1974, when it was recognized as closely related to the streptococci.
The pneumococcus would go on to become one of the most scientifically important bacteria in all of history — not only as the leading cause of community-acquired pneumonia, but as the experimental organism through which Fred Griffith (1928) and then Avery, MacLeod, and McCarty (1944) demonstrated that DNA is the molecule of heredity. The humble cause of “the old man’s friend” thus sits at the foundation of modern molecular biology, a legacy far beyond the lungs in which it was first found.
Friedländer, Fraenkel, and More Than One Culprit
The early 1880s made clear something that physicians had long suspected but could not prove: pneumonia is not a single disease with a single cause, but a clinical pattern that several different microbes can produce. Two German investigators are central to this part of the story, and it is important to keep their contributions distinct, because they are easy to conflate. In 1882, the pathologist Carl Friedländer described an encapsulated bacillus that he isolated from the lungs of patients who had died of pneumonia. The organism Friedländer described is not the pneumococcus; it is the bacterium now called Klebsiella pneumoniae, still known to this day as “Friedländer’s bacillus,” the cause of a severe form of pneumonia (Friedländer’s pneumonia). Friedländer’s work was also methodologically significant, as it pushed bacteriologists toward staining techniques to visualize these organisms in tissue.
In 1884, the German physician Albert Fraenkel (1848–1916) established that the diplococcus — the pneumococcus — was the predominant cause of the common lobar pneumonia, distinguishing it clearly from Friedländer’s encapsulated bacillus. The means of telling the two organisms apart arrived in the very same year, 1884, when the Danish bacteriologist Hans Christian Gram introduced the staining method that still bears his name. The Gram stain — developed in part while working with these very pneumonia bacteria — divides bacteria into Gram-positive and Gram-negative classes and made it straightforward to distinguish the Gram-positive pneumococcus from the Gram-negative Friedländer’s bacillus. Within a few short years, then, medicine had not only found bacterial causes of pneumonia but had acquired the laboratory tool to tell competing culprits apart.
The lesson of this period endures in modern practice. Today we recognize that pneumonia can be caused by many organisms: Streptococcus pneumoniae remains the single most common bacterial cause of community-acquired pneumonia, but Klebsiella pneumoniae, Haemophilus influenzae, Staphylococcus aureus, the “atypical” bacteria such as Mycoplasma and Legionella, and a wide range of respiratory viruses (including influenza) all produce the same fundamental syndrome of an inflamed, fluid-filled lung. The nineteenth-century discovery that pneumonia has multiple distinct causes — not one — is the direct ancestor of the modern clinical effort to identify the specific organism in each patient so that treatment can be targeted.
The “Captain of the Men of Death”
No phrase is more closely associated with the historical dread of pneumonia than “the Captain of the Men of Death,” and it was the great clinician-teacher Sir William Osler (1849–1919) who fastened it to the disease. The phrase, however, was not Osler’s invention. It descends from the English writer John Bunyan, who in his 1680 work The Life and Death of Mr. Badman wrote of “Captain Consumption” and “the Captain of all these men of death” — a reference, in the seventeenth century, to consumption, the wasting disease we now call tuberculosis, long before the word “tuberculosis” even existed. Bunyan’s grim military metaphor cast the deadliest disease of the age as the commanding officer of an army of fatal ailments.
Osler borrowed and re-aimed that metaphor. In his enormously influential textbook The Principles and Practice of Medicine — first published in 1892 and revised through many editions — Osler reflected on pneumonia’s staggering toll. In the 1901 edition he wrote that pneumonia had become “the Captain of the Men of Death,” the title Bunyan had once given consumption, because by the turn of the twentieth century pneumonia rivalled or surpassed tuberculosis as a cause of death in many cities. (In earlier passages Osler had ranked pneumonia just behind tuberculosis — a “lieutenant” or close second in the mortality bills — before its rising death rate, in his view, promoted it to captain.) The honest historical point is that the phrase originated with Bunyan for tuberculosis and was deliberately transferred by Osler to pneumonia; this page repeats it as Osler’s well-attested description, not as a claim that he coined it.
Osler is also remembered for calling pneumonia “the old man’s friend,” a phrase capturing the bleak comfort that, in an age without antibiotics, a swift pneumonia often brought a relatively quick and merciful end to the frail and the suffering elderly who might otherwise linger. Together these two phrases — captain of the men of death and the old man’s friend — convey exactly what pneumonia meant in the pre-antibiotic world: a leading and frequently unstoppable cause of death, feared by the young and strong yet sometimes a release for the very old. It is precisely this fearsome reputation that the discoveries of the following decades would overturn.
The Cure: Sulfa Drugs, Penicillin, and Vaccines
For all of recorded history up to the 1930s, a physician could name pneumonia, hear it through a stethoscope, and even identify the bacterium under a microscope — yet could offer the patient essentially no specific treatment beyond rest, nursing, fluids, and hope. That changed with breathtaking speed in the span of a single generation. The first real chemical weapon was the sulfonamide class of antibacterial drugs. In particular sulfapyridine, introduced in the late 1930s (around 1938), was shown to be effective against pneumococcal pneumonia and was used with dramatic results — most famously in the treatment of British Prime Minister Winston Churchill’s bacterial pneumonia in 1942. For the first time, the natural course of a deadly pneumonia could be interrupted by a drug.
The sulfa drugs were quickly eclipsed by an even greater advance: penicillin. Discovered by Alexander Fleming in 1928 and developed into a usable medicine by Howard Florey, Ernst Chain, and their colleagues in the early 1940s, penicillin proved extraordinarily effective against the pneumococcus and rapidly became the treatment of choice for bacterial pneumonia. The disease that Osler had crowned the Captain of the Men of Death — a frequent and feared killer of the young and the strong — became, for most patients with the common bacterial forms, a curable illness. The transformation in survival was so profound that it ranks among the central medical triumphs of the twentieth century. (Antibiotics act only against bacteria; the many viral pneumonias, including those caused by influenza, are not cured by them — a distinction that remains clinically vital today.)
Even cure, however, was not the whole answer, because some patients still died early in the illness before antibiotics could take hold. This drove the third great advance: prevention by vaccination. Building on decades of work on the pneumococcus’s protective polysaccharide capsule, a 14-valent pneumococcal polysaccharide vaccine was licensed in 1977, followed by the broader 23-valent polysaccharide vaccine (PPSV23) in 1983, which protects against the most common disease-causing strains. Because the plain polysaccharide vaccines work poorly in young children, a 7-valent pneumococcal conjugate vaccine (PCV7) was licensed for children in 2000; it was later expanded to cover thirteen strains (PCV13) in 2010, with still-broader conjugate vaccines following. Together, antibiotics and vaccines turned pneumonia from an untreatable and often fatal mystery into a disease that can, in most cases, be both prevented and cured — even as it remains a serious illness, and a leading infectious cause of death worldwide, especially among young children, the elderly, and those with weakened immune systems.
Research Papers and References
The references below combine peer-reviewed historical and review articles with curated PubMed topic-search links into the history of pneumonia, the pneumococcus, and the development of its treatments and vaccines. Historical primary texts — the Hippocratic Corpus, Laennec’s De l’Auscultation Médiate (1819), Bunyan’s The Life and Death of Mr. Badman (1680), and Osler’s The Principles and Practice of Medicine (1892–1901 editions) — are named in the article as historical sources rather than as modern citations. Each link opens in a new tab.
- Karamanou M, Androutsos G, et al. Hippocratic concepts of acute and urgent respiratory diseases still relevant to contemporary medical thinking and practice: a scoping review. — PMC: Hippocratic concepts of acute respiratory disease
- Watson DA, Musher DM, et al. A brief history of the pneumococcus in biomedical research. Seminars in Respiratory Infections. 1993. — PubMed: a brief history of the pneumococcus
- The ‘captain of the men of death’, Streptococcus pneumoniae — review of the pneumococcus and its disease. — PMC: the ‘captain of the men of death’, S. pneumoniae
- Biological puzzles solved by using Streptococcus pneumoniae: a historical review of the pneumococcal studies that shaped molecular bacteriology. Journal of Bacteriology. 2024. — doi:10.1128/jb.00059-24
- Roguin A. Rene Theophile Hyacinthe Laënnec (1781–1826): the man behind the stethoscope. Clinical Medicine & Research. 2006;4(3):230–235. — doi:10.3121/cmr.4.3.230
- Laennec, the stethoscope, and the history of auscultation and mediate auscultation. — PubMed: Laennec, the stethoscope, and auscultation
- The remarkable history of pneumococcal vaccination: an ongoing challenge. Pneumonia. 2022. — PMC: the remarkable history of pneumococcal vaccination
- The changing fate of pneumonia as a public health concern in 20th-century America and beyond. — PMC: the changing fate of pneumonia in 20th-century America
- Carl Friedländer, Friedländer’s bacillus, and the discovery of Klebsiella pneumoniae. — PubMed: Friedländer and Klebsiella pneumoniae history
- Albert Fraenkel and the establishment of the pneumococcus as a cause of lobar pneumonia. — PubMed: Fraenkel and the pneumococcus
- Hans Christian Gram and the history and development of the Gram stain. — PubMed: the history of the Gram stain
- Sulfonamides, sulfapyridine, and the early chemotherapy of pneumococcal pneumonia. — PubMed: sulfonamides and pneumococcal pneumonia
- Penicillin and the treatment of bacterial pneumonia: historical perspective. — PubMed: penicillin and the treatment of pneumonia
- Streptococcus pneumoniae reclassification and nomenclature (Diplococcus to Streptococcus, 1974). — PubMed: pneumococcus nomenclature and reclassification
External Authoritative Resources
- CDC — Pneumococcal Disease
- NHLBI (NIH) — Pneumonia
- PubMed — History of pneumonia and the pneumococcus
Connections
- Pneumonia (overview)
- All Conditions
- Tuberculosis
- Influenza
- COPD
- Asthma
- Acute Respiratory Distress Syndrome