Cor Pulmonale
Cor pulmonale — literally "lung heart" in Latin — is right ventricular dysfunction or failure caused by pulmonary hypertension arising from lung disease or hypoxemia. COPD is the leading cause in Western nations; supplemental oxygen is the only therapy proven to reduce mortality in the hypoxemic form; once established, it marks advanced underlying disease with poor prognosis.
Table of Contents
- Definition and Overview
- Causes and Underlying Conditions
- Pathophysiology
- Clinical Presentation
- Diagnosis: Imaging and Hemodynamics
- Acute Cor Pulmonale (Massive PE)
- Treatment: Targeting Underlying Disease
- Treatment: Volume Management and Vasodilators
- Prognosis
- Patient Self-Management and Monitoring
- References & Research
- Featured Videos
Definition and Overview
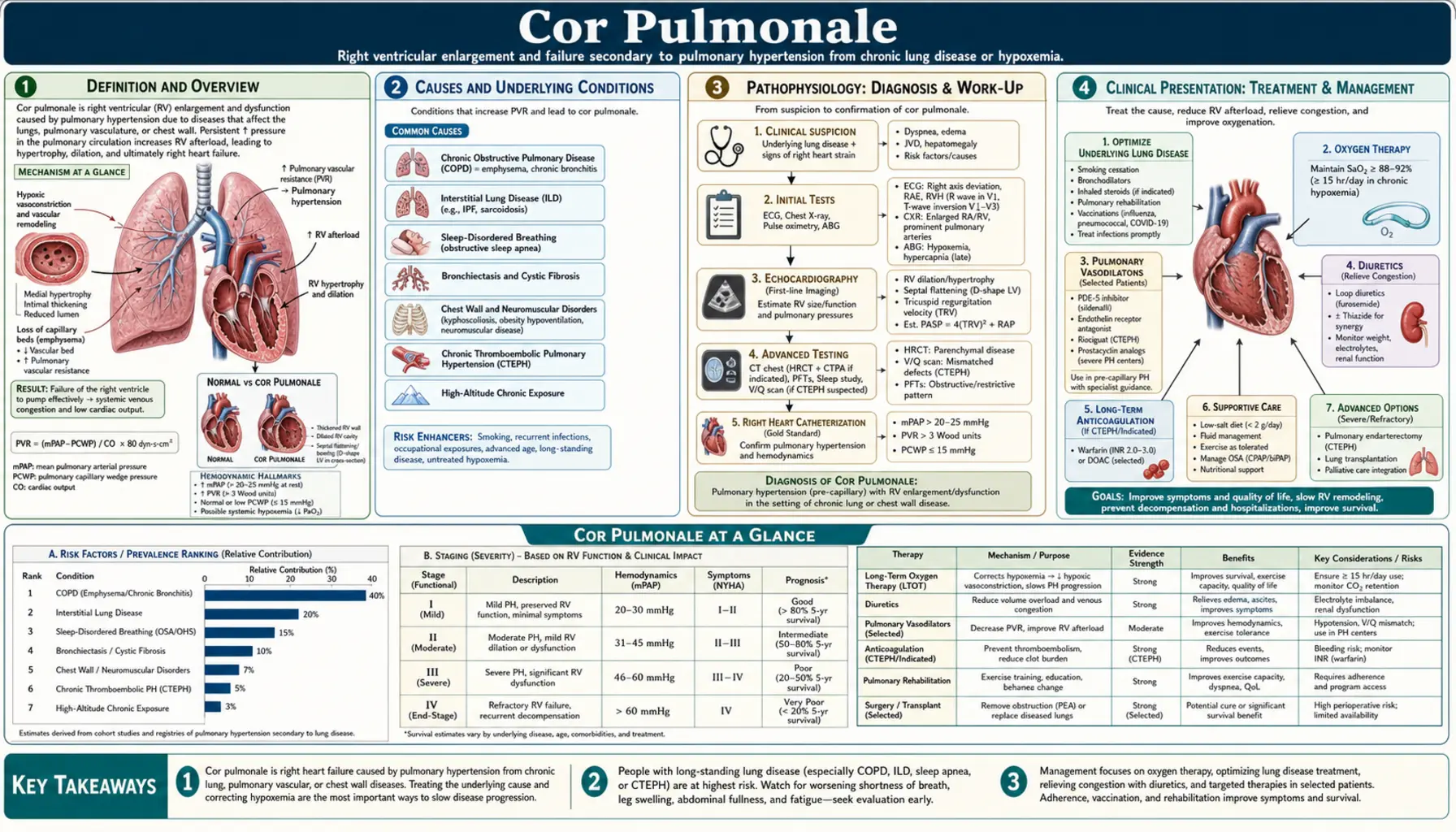
Cor pulmonale is right ventricular (RV) dysfunction or failure caused by pulmonary hypertension (PH) due to lung disease or hypoxemia. The definition strictly excludes RV failure that arises from left ventricular disease: when LV failure produces PH that then overloads the RV, the mechanism is "left heart disease" (WHO Group 2 PH), a categorically distinct entity. Only when the primary driver originates in the lungs or pulmonary vasculature — not the left heart — does the diagnosis of cor pulmonale apply.
The term translates literally as "lung heart" from Latin, reflecting this causal chain. Classification divides into two fundamentally different syndromes:
- Acute cor pulmonale: Massive pulmonary embolism is the most common cause. Sudden obstruction of more than 50% of the pulmonary vascular bed imposes acute RV pressure overload, causing rapid RV dilation and hemodynamic collapse. Treated as a PE emergency, not as chronic disease management.
- Chronic cor pulmonale: COPD accounts for approximately 50% of cases in Western nations. Progressive hypoxic vasoconstriction, vascular remodeling, and destruction of the pulmonary capillary bed over months to years cause sustained elevation in pulmonary vascular resistance, with gradual RV hypertrophy, dilation, and eventual failure.
Epidemiologically, cor pulmonale affects roughly 6–7% of all US adults with chronic heart disease. Its prevalence is rising in parallel with the growing burden of COPD and interstitial lung disease. Importantly, the development of cor pulmonale is a marker of advanced underlying lung disease — it signals that cardiopulmonary reserve is nearly exhausted and carries a poor prognosis independent of the specific underlying condition.
Causes and Underlying Conditions
Any condition that chronically elevates pulmonary vascular resistance through hypoxemia, vascular destruction, or mechanical obstruction can lead to cor pulmonale. The major cause categories are:
Obstructive Lung Diseases
This is the most common cause group in the United States and Europe. COPD is the single leading cause, driving cor pulmonale through a combination of chronic hypoxic pulmonary vasoconstriction, fixed vascular remodeling from tobacco-related endothelial injury, and destruction of the alveolar capillary bed in emphysema. Severe asthma and cystic fibrosis (late stage) also fall in this category.
Parenchymal Lung Diseases
Interstitial lung diseases obliterate the pulmonary vasculature through two mechanisms: fibrotic tissue physically encases and collapses small vessels, and hypoxemia from poor gas exchange triggers vasoconstriction. Idiopathic pulmonary fibrosis (IPF) carries particularly high PH prevalence (30–50% of patients). Other relevant conditions include sarcoidosis (WHO Group 5 PH), hypersensitivity pneumonitis, connective tissue disease-related ILD, silicosis, and coal workers' pneumoconiosis.
Pulmonary Vascular Diseases
Chronic thromboembolic pulmonary hypertension (CTEPH) arises when organized, fibrotic thrombus fails to resolve after pulmonary embolism, mechanically obstructing the pulmonary arterial tree. It affects approximately 3–5% of PE survivors and is uniquely important because surgical pulmonary endarterectomy can be curative. Pulmonary arterial hypertension (Group 1 PH) produces cor pulmonale when untreated or inadequately treated, through primary obliterative vasculopathy of the small pulmonary arteries.
Hypoventilation Disorders
Obesity hypoventilation syndrome (OHS), historically called "Pickwickian syndrome," causes chronic hypercapnia and hypoxemia through blunted respiratory drive and chest wall restriction from excess weight. Recurrent nocturnal hypoxemia triggers sustained pulmonary vasoconstriction. Obstructive sleep apnea (OSA) produces repetitive nocturnal hypoxemia and hypercapnia; chronic exposure elevates baseline pulmonary artery pressure. Neuromuscular disease (respiratory muscle weakness causing hypoventilation) and kyphoscoliosis (restrictive chest wall physiology) operate through the same hypoxemia-vasoconstriction pathway. High altitude and chronic mountain sickness (Monge's disease) represent the environmental extreme of the same mechanism.
Pathophysiology
The sequence linking lung disease to RV failure passes through several identifiable steps: underlying lung disease → pulmonary hypertension → RV pressure overload → RV hypertrophy → RV dilation → RV failure.
Mechanisms of Pulmonary Hypertension in Lung Disease
Hypoxic pulmonary vasoconstriction (HPV) is the most important acute mechanism. When alveolar oxygen tension falls, smooth muscle cells in pulmonary arterioles contract, diverting blood away from poorly ventilated alveoli. In localized disease, this is actually beneficial — it reduces V/Q mismatch. In generalized lung disease with global hypoxemia, HPV affects the entire pulmonary vasculature, raising resistance throughout. Critically, HPV is largely reversible with supplemental oxygen in early disease — this is the basis for long-term oxygen therapy (LTOT) as the cornerstone of cor pulmonale management.
Vascular remodeling is the chronic, fixed mechanism. Sustained HPV drives smooth muscle cell proliferation, intimal thickening, and adventitial fibrosis in pulmonary arterioles. Once structural remodeling is established, PVR elevation is no longer fully reversible by supplemental oxygen — even optimal oxygenation cannot undo fixed anatomical narrowing.
Polycythemia compounds the hemodynamic burden. Chronic hypoxemia stimulates erythropoietin secretion, raising red blood cell mass and blood viscosity. Higher viscosity increases the work required to propel blood through the pulmonary vasculature, raising effective PVR further. Phlebotomy can reduce viscosity in symptomatic secondary erythrocytosis.
Mechanical destruction operates in emphysema (capillary bed destruction by alveolar wall loss) and fibrosis (vascular obliteration by scar tissue), reducing the total cross-sectional area of the pulmonary vasculature. With fewer parallel pathways for blood to traverse, resistance rises according to Poiseuille's law even at normal blood viscosity and flow.
Right Ventricular Adaptation and Failure
The RV responds to chronically elevated afterload through concentric hypertrophy — adding sarcomeres in parallel to increase wall thickness and normalize wall stress. Initially this is adaptive: RV output is maintained at the cost of increased oxygen demand. As PVR continues rising, the RV reaches a tipping point. Dilation begins (eccentric remodeling), the tricuspid annulus stretches producing regurgitation, and the interventricular septum shifts leftward (D-shaped LV on echocardiogram). Once RV wall tension consistently exceeds coronary perfusion pressure during systole, subendocardial ischemia develops — the RV cannot meet its own oxygen demand — and contractile failure follows. Ventricular interdependence means RV dilation impairs LV filling by leftward septal shift, further reducing cardiac output and systemic perfusion even when LV function itself is preserved.
Clinical Presentation
Symptoms of cor pulmonale are often masked by or intertwined with those of the underlying lung disease. The key clinical clue is deterioration beyond what the known lung disease should explain — worsening dyspnea that outpaces the pace of lung disease progression, or new fluid retention.
Symptoms
Dyspnea is universal but its change in character is the diagnostic clue: previously exertional dyspnea becoming dyspnea at rest, or dyspnea worsening faster than the lung disease alone would predict, signals that RV failure is developing. Peripheral edema — bilateral pitting edema of the ankles, calves, and in severe cases the thighs and sacrum — is the most visible manifestation of elevated venous pressure from RV failure. Ascites reflects third-spacing from hepatic venous congestion; right upper quadrant discomfort from hepatomegaly and capsular stretch may accompany it. Fatigue and severely reduced exercise tolerance result from a fixed, low cardiac output that cannot augment with exertion. Syncope with exertion indicates that cardiac output cannot meet the metabolic demand of exercise, causing cerebral hypoperfusion — a serious sign requiring urgent assessment.
Physical Examination Signs
Jugular venous distension (JVD) from elevated central venous pressure is a cardinal sign; cannon A-waves may appear in the setting of tricuspid regurgitation. Hepatojugular reflux (HJR) is positive — sustained abdominal pressure raises JVP as the failing RV cannot accommodate the increased venous return. Parasternal heave (a palpable sustained systolic impulse along the left lower sternal border) indicates RV enlargement. Loud P2 (accentuated pulmonic component of S2, audible across the precordium) is the auscultatory hallmark of pulmonary hypertension. A tricuspid regurgitation murmur — holosystolic at the left sternal border, increasing with inspiration (Carvallo's sign) — reflects annular dilation from RV enlargement. Hepatomegaly with potential for pulsatile liver (from TR) and peripheral or central cyanosis from desaturation complete the picture in advanced disease.
Diagnosis: Imaging and Hemodynamics
No single test diagnoses cor pulmonale; the workup confirms RV dysfunction, quantifies pulmonary pressures, and characterizes the underlying lung disease. Echocardiography is the gateway non-invasive test; right heart catheterization provides definitive hemodynamic confirmation.
Electrocardiogram
The ECG shows several signs of right heart strain, though no single finding is highly sensitive. P pulmonale (peaked P waves >2.5 mm in leads II, III, aVF) indicates right atrial enlargement. Right axis deviation (axis beyond +90°) reflects RV dominance. RV strain pattern (ST depression and T-wave inversion in V1–V4) indicates RV pressure overload. Right bundle branch block (RBBB), complete or incomplete, and S1Q3T3 pattern (particularly in acute cor pulmonale from massive PE) round out the ECG profile.
Echocardiography
Transthoracic echocardiography is the first-line non-invasive assessment. Key measurements include: RVSP estimated from the tricuspid regurgitation jet velocity; RV size and function (TAPSE <16 mm or tissue Doppler S′ <10 cm/s indicate RV dysfunction); interventricular septal flattening (D-shaped LV in systole indicates pressure overload; flattening in both systole and diastole indicates combined pressure and volume overload); and pericardial effusion, which carries a poor prognostic significance. Echocardiography also evaluates LV function to exclude Group 2 PH from left heart disease.
Chest Radiograph and Pulmonary Function Tests
The chest X-ray reveals enlarged central pulmonary arteries (PA diameter >29 mm), peripheral vascular pruning (absent markings in the outer third of the lung fields), and cardiomegaly with RV prominence. Signs of the underlying disease — hyperinflation and flat diaphragms in COPD, honeycombing and reticulation in IPF — provide etiologic context. Pulmonary function tests characterize the underlying disease pattern: obstructive (COPD, asthma) or restrictive (IPF, kyphoscoliosis).
Right Heart Catheterization
Right heart catheterization is the definitive test. Per the 2022 ESC/ERS guidelines, pulmonary hypertension is now defined as mean PA pressure (mPAP) >20 mmHg (the prior threshold was >25 mmHg). Pre-capillary PH — the hemodynamic pattern of cor pulmonale from lung disease — requires mPAP >20 mmHg, PVR >2 Wood units, and pulmonary capillary wedge pressure (PCWP) ≤15 mmHg. The PCWP threshold distinguishes cor pulmonale (pre-capillary; PCWP ≤15 mmHg; driven by lung disease) from PH due to left heart disease (post-capillary; PCWP >15 mmHg) — a critical distinction with major therapeutic implications.
Acute Cor Pulmonale (Massive PE)
Acute cor pulmonale from massive pulmonary embolism is a distinct clinical emergency with different pathophysiology, time course, and treatment from the chronic form.
Mechanism and Recognition
When a massive clot burden suddenly obstructs more than 50% of the pulmonary vascular bed, the RV faces acute pressure overload it has no time to adapt to (unlike the chronic form, where slow remodeling allows partial compensation). Acute RV dilation develops within hours, producing hemodynamic collapse. The key echocardiographic findings that distinguish acute cor pulmonale from PE are the RV:LV ratio >0.9 and McConnell's sign — regional RV dysfunction with free wall akinesis but preserved apical motility — which is highly specific for massive PE rather than chronic RV failure.
Treatment of Massive PE
Systemic thrombolysis (tPA 100 mg over 2 hours) is indicated for hemodynamically unstable massive PE; randomized data demonstrate a 65% absolute reduction in mortality compared to heparin alone in this setting. Catheter-directed therapy (CDT) — including ultrasound-assisted thrombolysis (EKOS/acoustic pulse thrombolysis) — is used for submassive PE with RV dysfunction without overt hemodynamic collapse; the PE-COPE and SEATTLE II trials demonstrated significant RV strain reduction at 48 hours. Surgical embolectomy on cardiopulmonary bypass is reserved for cases where thrombolysis is contraindicated or has failed. Anticoagulation alone (unfractionated heparin immediately) is appropriate for submassive PE without hemodynamic compromise, where the RV is stressed but not yet failing.
Treatment: Targeting Underlying Disease
The primary therapeutic strategy in chronic cor pulmonale is aggressive management of the underlying pulmonary disease. Treating the cause of the elevated PVR — not just the RV failure — is what offers the best opportunity to slow progression and improve prognosis.
COPD
Optimize bronchodilator therapy (long-acting muscarinic antagonists [LAMA], long-acting beta agonists [LABA], inhaled corticosteroids as appropriate per GOLD guidelines), enroll in pulmonary rehabilitation, and most importantly, address smoking cessation — the only intervention that slows FEV1 decline in COPD. Lung volume reduction surgery (LVRS) improves exercise capacity and survival in selected emphysema patients with upper-lobe predominant disease and low exercise capacity (NETT trial).
IPF and Other ILD
Antifibrotic drugs (nintedanib, pirfenidone) slow IPF progression by approximately 50% in trials (INPULSIS, ASCEND) but do not reverse established pulmonary hypertension. Treating the fibrotic process limits further vascular obliteration.
Sleep Apnea and Hypoventilation Syndromes
CPAP for OSA is among the most actionable interventions in this category: eliminating nocturnal hypoxemic episodes reduces repetitive pulmonary vasoconstriction, and longitudinal data show measurable reduction in pulmonary artery pressures over months. Bilevel PAP (BPAP or AVAPS) for obesity hypoventilation syndrome addresses both nocturnal hypercapnia and hypoxemia; combined with substantial weight loss, dramatic improvement in PH and cor pulmonale is possible — unlike most other causes, this is potentially reversible.
CTEPH
Pulmonary endarterectomy (PEA) is potentially curative for operable CTEPH, removing organized thrombus from the proximal pulmonary arteries and normalizing pressures in many patients. For inoperable CTEPH, riociguat (a soluble guanylate cyclase stimulator) is FDA-approved and reduces PVR and improves functional capacity.
Supplemental Oxygen
Long-term oxygen therapy (LTOT) is the most important evidence-based intervention for hypoxic cor pulmonale. The landmark MRC Trial (1981) and Nocturnal Oxygen Therapy Trial (NOTT, 1980) established that continuous supplemental oxygen (>15–18 hours/day, target SpO2 88–92%) reduces mortality and slows PVR progression in hypoxemic COPD. Oxygen reverses the reversible component of HPV — it cannot undo established vascular remodeling, but it removes the ongoing vasoconstriction stimulus. In hypercapnic COPD patients, target SpO2 88–92% (not higher) to avoid suppressing the hypoxic respiratory drive and worsening CO2 retention.
Treatment: Volume Management and Vasodilators
Beyond targeting the underlying disease, symptomatic management of RV failure focuses on fluid balance optimization and careful consideration of vasoactive agents.
Diuretics
Loop diuretics (furosemide, torsemide) are the primary treatment for fluid overload, peripheral edema, and ascites. The therapeutic goal is euvolemia — resolution of peripheral edema without inducing intravascular volume depletion, which can reduce RV preload and precipitate hemodynamic deterioration. The RV in cor pulmonale is preload-dependent; excessive diuresis is a common cause of acute decompensation. Careful titration with monitoring of electrolytes (particularly potassium and magnesium) is essential. Aldosterone antagonists (spironolactone) reduce aldosterone-driven sodium retention but require caution in renal insufficiency due to hyperkalemia risk.
Digoxin
Digoxin has limited and inconsistent evidence in cor pulmonale. It is a weak positive inotrope and can be considered in refractory RV failure, but hypoxemia and hypokalemia both sensitize the myocardium to digoxin toxicity — common conditions in cor pulmonale patients — requiring careful dosing and electrolyte monitoring.
Pulmonary Vasodilators: A Cautionary Note
PAH-specific vasodilators (phosphodiesterase-5 inhibitors, endothelin receptor antagonists, prostacyclin analogues, riociguat) are not routinely recommended for cor pulmonale arising from COPD or ILD (WHO Group 3 PH). Unlike Group 1 PAH, where the vascular obliteration is the primary problem, Group 3 cor pulmonale involves ventilated but poorly perfused lung areas. Pulmonary vasodilators increase flow to these poorly ventilated areas, worsening ventilation-perfusion (V/Q) mismatch and arterial hypoxemia. No survival benefit has been proven in randomized trials for this indication, and potential harm from worsened oxygenation is real. The exception is CTEPH and Group 1 PAH, where these drugs are specifically indicated and the mechanism is different.
Phlebotomy
For symptomatic secondary polycythemia with hematocrit consistently above 55%, phlebotomy to a target hematocrit of 45–50% reduces blood viscosity and effective PVR. This does not improve prognosis but can relieve symptoms of hyperviscosity (headache, plethora, impaired cognition) in selected patients.
Prognosis
Cor pulmonale signals that underlying lung disease has consumed most of the available cardiopulmonary reserve. Prognosis is primarily determined by the underlying condition and its responsiveness to treatment, but the development of RV failure universally worsens the trajectory.
COPD with Cor Pulmonale
Five-year survival is approximately 30% once RV failure is established. The MRC Trial (1981) demonstrated that long-term oxygen therapy doubled survival at five years in hypoxemic COPD, with a 36% reduction in mortality. The NOTT Trial (1980) confirmed that continuous oxygen (>18 hours per day) was superior to nocturnal oxygen alone, establishing the current standard of LTOT >15–18 hours daily.
IPF with Cor Pulmonale
Pulmonary hypertension in IPF carries particularly grim prognosis: median survival is approximately 2.8 years in IPF-PH compared to 4.8 years in IPF without PH. PH is an independent predictor of mortality in IPF independent of lung function parameters.
Prognostic Markers
Key prognostic indicators include echocardiographic TAPSE <16 mm, RV:LV ratio >1, elevated BNP or NT-proBNP, reduced six-minute walk distance, reduced DLCO, and low resting PaO2. Pericardial effusion on echocardiography is a particularly ominous finding.
Lung Transplantation
Bilateral sequential lung transplantation is the definitive treatment for refractory end-stage lung disease with cor pulmonale. Patients with CTEPH who have undergone successful pulmonary endarterectomy can experience dramatic, near-complete recovery of RV function — one of the most gratifying outcomes in pulmonary medicine. For IPF and COPD with cor pulmonale, early referral to a transplant center (while still in a functional window that permits candidacy) is critical, as median post-transplant survival of 5–7 years compares favorably to the trajectory of advanced cor pulmonale on medical therapy.
Patient Self-Management and Monitoring
Living with cor pulmonale requires active daily monitoring and adherence to therapies that have proven mortality benefit. The following practices are central to maintaining stability and catching decompensation early.
Oxygen Therapy Adherence
If prescribed long-term oxygen therapy, use it for at least 15–18 hours every day — this is the only pharmacological intervention proven to extend life in hypoxemic cor pulmonale. Nighttime use alone is insufficient. Check equipment regularly (flow settings, tubing integrity, concentrator function). Make travel arrangements well in advance: commercial aircraft cabin pressure is equivalent to approximately 6,000–8,000 feet altitude; high-risk patients require in-flight supplemental oxygen arranged through the airline. High-altitude destinations worsen hypoxic vasoconstriction acutely and can precipitate decompensation even in stable patients.
Daily Weight and Edema Monitoring
Weigh yourself at the same time each morning after urinating. A gain of more than 2 pounds in a single day or 5 pounds in a week indicates fluid retention requiring prompt contact with your provider or activation of a pre-established diuretic action plan. Photograph ankle edema weekly to track changes objectively. Any worsening beyond your individual baseline warrants prompt medical contact before the next scheduled appointment.
Activity Pacing and Pulmonary Rehabilitation
Energy conservation strategies — planning activities for times of day when energy is highest, spacing tasks with rest periods, using assistive devices — help maintain function within the limits of a fixed cardiac output. Supervised pulmonary rehabilitation programs improve functional status, dyspnea, and six-minute walk distance in COPD-related cor pulmonale through supervised exercise training, education, and psychosocial support.
Vaccination and Infection Prevention
Annual influenza vaccination and pneumococcal vaccination (PCV20 or PPSV23 per current CDC recommendations) are essential. Respiratory infections are among the most common precipitants of acute cor pulmonale decompensation in patients with chronic lung disease.
Smoking Cessation and Sodium Restriction
Smoking cessation is the single most impactful modifiable intervention in COPD-related cor pulmonale — it is the only strategy proven to slow the underlying FEV1 decline that drives disease progression. Nicotine replacement, varenicline, and behavioral support all improve quit rates. For patients with recurrent fluid overload, sodium restriction to less than 2 grams per day reduces the kidney's tendency to retain fluid and may allow lower diuretic doses.
References & Research
Key Research Papers
- Medical Research Council Working Party. Long term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis and emphysema (MRC Trial). Lancet. 1981;1(8222):681–686. PMID 6110912
- Nocturnal Oxygen Therapy Trial Group. Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease (NOTT). Ann Intern Med. 1980;93(3):391–398. PMID 6776858
- Weitzenblum E, Sautegeau A, Ehrhart M, et al. Long-term oxygen therapy can reverse the progression of pulmonary hypertension in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis. 1985;131(4):493–498. — Search PubMed
- Seeger W, Adir Y, Barbera JA, et al. Pulmonary hypertension in chronic lung diseases. J Am Coll Cardiol. 2013;62(25 Suppl):D109–116. PMID 24355634
- Vonk-Noordegraaf A, Haddad F, Chin KM, et al. Right heart adaptation to pulmonary arterial hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D22–33. PMID 24355634
- Benza RL, Park MH, Keogh A, Girgis RE. Management of pulmonary arterial hypertension with a focus on combination therapies. J Heart Lung Transplant. 2007;26(5):437–446. PMID 17449411
- Strange G, Playford D, Stewart S, et al. Pulmonary hypertension: prevalence and mortality in the Armadale echocardiography cohort. Heart. 2012;98(24):1805–1811. — Search PubMed
- Simonneau G, Montani D, Celermajer DS, et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J. 2019;53(1):1801913. PMID 30545968
- Humbert M, Kovacs G, Hoeper MM, et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022;43(38):3618–3731. PMID 36017548
- McLaughlin VV, Archer SL, Badesch DB, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension. J Am Coll Cardiol. 2009;53(17):1573–1619. PMID 19389575
- Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (GOLD 2013). Am J Respir Crit Care Med. 2013;187(4):347–365. PMID 22878278
- Barst RJ, Gibbs JS, Ghofrani HA, et al. Updated evidence-based treatment algorithm in pulmonary arterial hypertension. J Am Coll Cardiol. 2009;54(1 Suppl):S78–84. PMID 19555865
Research Papers
The following PubMed topic searches retrieve current peer-reviewed literature on Cor Pulmonale. Each link opens a live PubMed query.
- Cor pulmonale COPD pulmonary hypertension treatment
- Right ventricular failure chronic lung disease
- Hypoxic pulmonary vasoconstriction oxygen therapy
- Cor pulmonale echocardiography right heart function
- Cor pulmonale COPD prognosis survival
- Long term oxygen therapy hypoxemic COPD
- Obesity hypoventilation cor pulmonale CPAP
- Acute cor pulmonale massive pulmonary embolism
- Pulmonary hypertension lung disease diagnosis
- Right ventricular dysfunction pulmonary fibrosis
Connections
- Pulmonology
- COPD
- Pulmonary Hypertension
- Pulmonary Arterial Hypertension
- Pulmonary Embolism
- Idiopathic Pulmonary Fibrosis
- Obstructive Sleep Apnea
- Respiratory Failure
- Alpha-1 Antitrypsin Deficiency
- Heart Failure