Carbon Monoxide Poisoning
Carbon monoxide (CO) poisoning is the most common cause of unintentional poisoning death in the United States — and among the most treatable, when recognized in time. Its danger lies precisely in the fact that CO is colorless, odorless, and tasteless: it provokes no warning sensation. People exposed to building up CO levels feel progressively unwell and often have no idea why. This page explains how CO kills, why routine pulse oximetry misses it entirely, how to treat it, and how to prevent it.
- What is Carbon Monoxide Poisoning?
- Sources of Carbon Monoxide: The Silent Killer
- Pathophysiology: How CO Kills
- Clinical Presentation: The Diagnostic Challenge
- Diagnosis: CO-Oximetry and Why Pulse Oximetry Fails
- Severity Assessment and COHb Levels
- Treatment: Oxygen Therapy and Hyperbaric Oxygen
- Delayed Neurological Sequelae
- Prevention: Detectors and Safety Rules
- Research Papers
- Connections
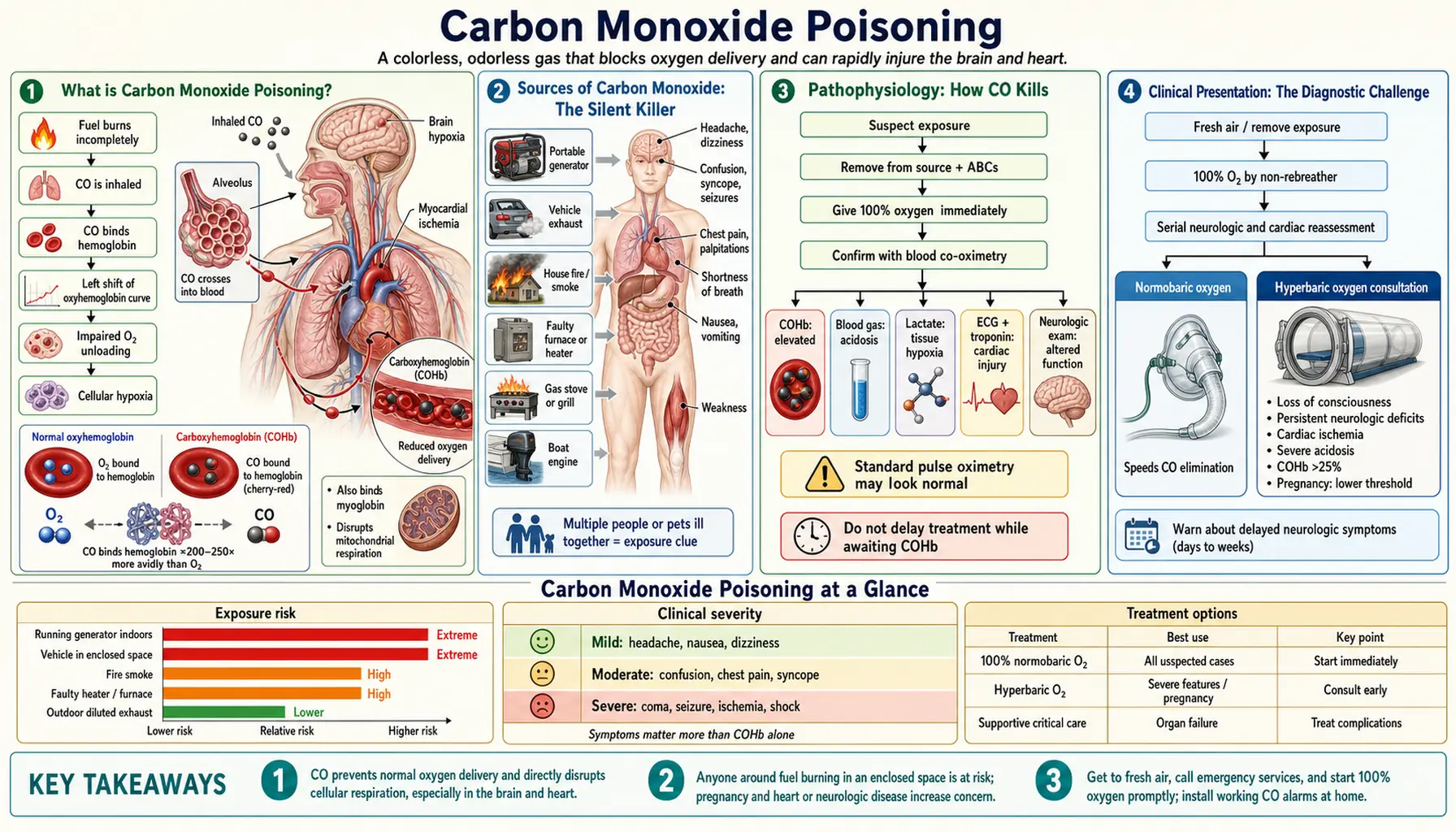
What is Carbon Monoxide Poisoning?
Carbon monoxide poisoning occurs when a person inhales sufficient quantities of CO gas to impair oxygen delivery to the body's tissues. Because CO is completely invisible and produces no smell or taste, there is no natural sensory warning — the gas accumulates silently while the victim's symptoms escalate from mild fatigue and headache to coma and death.
CO poisoning accounts for approximately 50,000 emergency department visits per year in the United States and causes roughly 400–500 unintentional, non-fire-related deaths annually. Many more deaths occur in the context of residential fires, where CO is a major contributor to mortality before the flames themselves cause injury. Globally, CO poisoning follows similar patterns, with a striking winter peak that mirrors the increased use of fuel-burning heating appliances as temperatures drop.
Poisoning can be unintentional — caused by a malfunctioning heating system, a portable generator running indoors, or a vehicle idling in an attached garage — or intentional, as CO inhalation is a common method in suicidal exposures. In both contexts, the physiology and treatment are identical.
One of the most clinically dangerous aspects of CO poisoning is its propensity to be misdiagnosed. The combination of headache, nausea, fatigue, and dizziness is indistinguishable from influenza, food poisoning, or migraine without a specific index of suspicion. Patients are sent home, return to the same environment, and worsen. Maintaining a high clinical suspicion — particularly when multiple household members are ill simultaneously — is the most important diagnostic step.
Sources of Carbon Monoxide: The Silent Killer
Carbon monoxide is a product of incomplete combustion — any time a carbon-based fuel (natural gas, propane, gasoline, wood, charcoal, kerosene) burns without sufficient oxygen, CO is produced alongside carbon dioxide. The most common and most dangerous sources are:
Gas Furnaces and Water Heaters
Cracked heat exchangers, blocked or disconnected flues, improper installation, and inadequate combustion air are the most common causes of CO accumulation in homes during winter months. A furnace may function normally for years before a developing crack in the heat exchanger begins leaking combustion gases into circulating household air. Annual professional inspection of all gas appliances and chimneys is the primary prevention strategy.
Portable Generators
Portable gasoline-powered generators are responsible for the largest number of CO deaths in the United States after natural disasters — power outages from hurricanes, ice storms, and blizzards prompt people to run generators indoors or in garages. A single generator can produce CO at concentrations 100 times higher than a car exhaust; CO can reach lethal levels in a closed garage within minutes. The rule is absolute: generators must operate outdoors only, at least 20 feet from any window, door, or vent. Over 400 people died from generator-related CO poisoning following Hurricanes Katrina, Sandy, and Irma/Maria combined.
Charcoal Grills and Hibachis
Charcoal combustion produces extremely high concentrations of CO. A charcoal grill should never be used indoors, in a garage, in a screened porch, or in a tent — even in rain. This rule applies equally to camping stoves burning propane or white gas in enclosed spaces.
Gasoline-Powered Tools and Equipment
Chainsaws, pressure washers, lawn mowers, snow blowers, and other gas-powered tools generate large volumes of CO and must be operated outdoors. Using a pressure washer inside a warehouse, barn, or parking garage — even with the door open — has caused fatal poisonings.
Vehicle Exhaust in Attached Garages
Even briefly warming up a car in an attached garage, with the garage door open, can allow CO to accumulate inside the adjoining home at dangerous concentrations. The CO diffuses through gaps around the door connecting the garage to the living space. The garage door must be fully open and the car should be backed out immediately.
Gas Ranges and Ovens
Prolonged use, malfunction, or intentional misuse (running an oven as a space heater) can produce dangerous CO. Burner malfunctions that produce yellow-orange rather than blue flames signal incomplete combustion.
Boats and Marine Engines
Carbon monoxide from generator or engine exhaust can accumulate near swim platforms, in cockpits, and under bimini tops — a hazard called "generator backdraft" or "station wagon effect." Multiple deaths have occurred when swimmers rested on swim platforms near operating generators. A carbon monoxide detector is now required by the US Coast Guard on boats with enclosed spaces.
House Fires and Industrial Exposure
CO is a major cause of death in structural fires — often killing occupants before flames reach them. Industrial workers in foundries, steel mills, and chemical plants face occupational CO exposure. Firefighters are at particular risk when entering burning structures without self-contained breathing apparatus (SCBA).
Pathophysiology: How CO Kills
Carbon monoxide's toxicity operates through three simultaneous mechanisms, each capable of causing profound cellular injury independently. Together, they create a state of oxygen deprivation that standard oxygen measurements — including pulse oximetry — completely miss.
Carboxyhemoglobin Formation: Functional Anemia
Carbon monoxide binds to hemoglobin with approximately 240 times greater affinity than oxygen. When CO occupies a hemoglobin binding site, it forms carboxyhemoglobin (COHb) — a molecule that cannot carry oxygen. A patient with 40% COHb has effectively lost 40% of their oxygen-carrying capacity, producing the equivalent of severe anemia, but with a total hemoglobin level that appears entirely normal on routine blood tests.
The Haldane Effect: Impaired Oxygen Unloading
CO poisoning has a second, subtler effect on the remaining oxygenated hemoglobin. The presence of CO on some hemoglobin subunits shifts the oxyhemoglobin dissociation curve leftward — meaning the unaffected, oxygen-carrying hemoglobin molecules now hold onto their oxygen more tightly and release less of it to tissues. This is the Haldane effect. The combination of reduced oxygen loading (because CO occupies binding sites) and reduced oxygen unloading (because the remaining oxygenated Hb grips O2 more tightly) produces profound tissue hypoxia that is worse than either effect alone would predict.
Cytochrome c Oxidase Inhibition: Cellular Respiratory Arrest
Even if sufficient oxygen could somehow be delivered to a cell, CO would still be toxic at the cellular level. CO directly inhibits cytochrome c oxidase (Complex IV), the final enzyme in the mitochondrial electron transport chain responsible for cellular ATP production. By blocking this enzyme, CO arrests cellular respiration at the tissue level — cells cannot use oxygen even when it is present. This mechanism explains why CO poisoning produces a lactic acidosis (anaerobic metabolism) and why symptoms can persist even after COHb levels normalize with treatment.
Myocardial and Muscle Injury
Cardiac myocytes have among the highest oxygen demands of any tissue and are particularly vulnerable to CO-mediated hypoxia and cytochrome inhibition. ECG changes, ST-segment elevation mimicking myocardial infarction, troponin elevation, and arrhythmias are common at moderate-to-severe exposures. CO also binds myoglobin in skeletal and cardiac muscle, adding direct muscle toxicity and contributing to rhabdomyolysis at high exposures.
Clinical Presentation: The Diagnostic Challenge
The central clinical challenge in CO poisoning is that its symptoms are completely nonspecific. There is no pathognomonic sign that — by itself — confirms the diagnosis. The presentation perfectly mimics dozens of common conditions, and the most dangerous aspect of CO poisoning is not the physiology but the diagnostic delay it causes.
The Classic Presentation: Flu Without Fever
The most common initial symptom is headache — typically described as dull, frontal, and progressively worsening. Nausea and vomiting, fatigue, malaise, and dizziness accompany the headache in most cases. The key distinguishing feature is the absence of fever: CO poisoning does not cause elevated body temperature, while genuine influenza almost always does. Despite this, CO poisoning is among the most commonly misdiagnosed conditions seen in emergency departments during winter months.
The Household Clue: Multiple Victims Including Pets
A critically important clinical observation: if multiple people in the same enclosed space are ill simultaneously, CO poisoning must be immediately considered. Dogs and other pets, with their higher respiratory rates and smaller body mass, often show symptoms — lethargy, ataxia, collapse — before humans reach dangerous COHb levels. Pets acting abnormally alongside a sick household should prompt immediate evacuation and emergency services.
The Hallmark History: Symptoms That Improve on Leaving the Building
Perhaps the single most diagnostically useful question is: "Did your symptoms improve when you left home or work — and then return when you went back?" This pattern of location-linked symptom fluctuation is highly characteristic of CO poisoning and is the history that should always be sought in patients presenting with nonspecific headache and nausea during winter months.
The Myth of Cherry-Red Skin
Medical textbooks traditionally describe cherry-red lips and skin as a hallmark of CO poisoning. In clinical practice, this finding is rare and unreliable — it is seen only at very high COHb concentrations and is most commonly observed post-mortem. Its absence absolutely does not exclude CO poisoning. Clinicians who wait for cherry-red skin before testing for COHb will miss the majority of cases.
Neurological and Cardiac Symptoms at Higher Exposures
As COHb levels rise, symptoms escalate from the nonspecific flu-like presentation toward frank neurological and cardiovascular impairment: confusion, slowed mentation, syncope, ataxia, and seizures. Chest pain, palpitations, and dyspnea reflect myocardial ischemia. At the highest exposures: coma, respiratory failure, and cardiac arrest.
Diagnosis: CO-Oximetry and Why Pulse Oximetry Fails
Understanding the diagnostic limitations of routine monitoring equipment is essential — a failure to grasp this point leads directly to missed diagnoses and patient deaths.
Standard Pulse Oximetry Falsely Reads Normal in CO Poisoning
The standard bedside pulse oximeter used in virtually every clinical setting measures oxygen saturation using two wavelengths of light (660 nm red and 940 nm infrared). It detects the optical difference between oxyhemoglobin and deoxyhemoglobin — but it cannot distinguish between oxyhemoglobin and carboxyhemoglobin. Carboxyhemoglobin absorbs light at wavelengths very similar to oxyhemoglobin and is read by the pulse oximeter as oxygenated hemoglobin. A patient with 50% COHb will display a pulse oximetry reading of 98–99% — appearing completely normal — while in reality half of their hemoglobin is nonfunctional. This is one of the most clinically important limitations of routine pulse oximetry.
CO-Oximetry: The Required Test
The correct diagnostic test is CO-oximetry, performed on an arterial blood gas (ABG) sample analyzed on a laboratory co-oximeter. Unlike a standard blood gas analyzer, a co-oximeter uses four or more wavelengths of light and can directly and accurately measure COHb%, methemoglobin (MetHb%), and other dyshemoglobins. This is the definitive test. Venous blood can also be used — venous COHb runs approximately 2–3% lower than arterial, but both are acceptable for diagnosis and management decisions.
Point-of-Care Non-Invasive CO-Oximetry
The Masimo Rad-57 pulse CO-oximeter is a non-invasive device that measures COHb transcutaneously using eight wavelengths of light. It is increasingly used for rapid screening in emergency department triage, enabling identification of CO-poisoned patients without waiting for an ABG. Its accuracy is somewhat lower than laboratory co-oximetry (particularly at low-to-moderate COHb levels), but it reliably avoids the critical pitfall of the standard two-wavelength pulse oximeter.
Supporting Laboratory and Electrocardiographic Studies
An ECG should be obtained in all cases — ST-segment changes (including ST elevation that can mimic STEMI), sinus tachycardia, and ventricular arrhythmias are common at moderate-severe exposures and guide both risk stratification and disposition decisions. Troponin elevation is found in a substantial proportion of significant CO exposures and carries prognostic weight: troponin I above 0.4 ng/mL has been associated with adverse neurological outcomes. Serum lactate is elevated due to impaired mitochondrial respiration, correlating roughly with severity, though it is not CO-specific. Head CT or MRI is indicated for patients with altered mental status or neurological signs — characteristic basal ganglia lesions (particularly in the globus pallidus) are visible on MRI and may appear on initial imaging or develop over the subsequent weeks as part of delayed neurological syndrome.
Severity Assessment and COHb Levels
Carboxyhemoglobin levels provide a useful but imperfect guide to clinical severity. An important caveat: COHb levels correlate poorly with clinical severity on an individual basis. Individuals with chronic exposure (such as heavy smokers, who may run baseline COHb of 5–10%) or those with significant comorbidities may be more or less symptomatic than their COHb level predicts. Duration of exposure matters as much as peak level. Clinical symptoms, cardiac findings, and neurological status must always be interpreted alongside the COHb measurement.
COHb Level Reference Ranges
- Less than 10%: Minimal or no symptoms. Note that heavy smokers can have baseline COHb of 5–10% from cigarette combustion alone.
- 10–20%: Throbbing headache, dizziness, nausea, mild cognitive impairment. Most patients are symptomatic.
- 20–40%: Severe headache, nausea and vomiting, confusion, weakness, palpitations, visual changes. Neurological function begins to deteriorate.
- 40–60%: Syncope, seizures, tachycardia, hypotension, chest pain, ST changes. Potentially fatal without treatment.
- Greater than 60%: Coma, respiratory failure, cardiovascular collapse, death.
Severity Classification for Treatment Decisions
The determination of whether to pursue hyperbaric oxygen (HBO) therapy is based on a severity classification that integrates COHb level with clinical features:
- Mild: No loss of consciousness; COHb less than 25%; no cardiac involvement; no significant neurological symptoms.
- Moderate to Severe (HBO indicated): Any loss of consciousness or syncope; COHb 25% or greater; cardiac involvement (troponin elevation, ECG changes); focal neurological deficits; seizures; pregnancy (any symptomatic exposure — the threshold for HBO is much lower due to increased fetal susceptibility).
Treatment: Oxygen Therapy and Hyperbaric Oxygen
Treatment of CO poisoning follows a clear stepwise approach, with urgency calibrated to severity. The fundamental principle is removing CO from the body and reversing the tissue hypoxia it has caused — and doing so as rapidly as possible to prevent irreversible neurological injury.
Step 1: Immediate Removal from Exposure
Remove the patient from the CO-containing environment immediately. Emergency responders must not enter an enclosed CO-contaminated space without self-contained breathing apparatus (SCBA) — multiple rescuers have been incapacitated or killed attempting to rescue CO victims without proper respiratory protection. Call emergency services; evacuate everyone in the building.
Step 2: 100% Normobaric Oxygen
Administer 100% oxygen via a tight-fitting non-rebreather mask as the first and most universally available treatment. Supplemental oxygen works by mass action: at very high inspired oxygen concentrations, the partial pressure of O2 dramatically exceeds that of CO, accelerating displacement of CO from hemoglobin binding sites. The COHb half-life on room air is approximately 4–5 hours. On 100% normobaric oxygen (NBO), this falls to approximately 60–90 minutes. Continue 100% O2 until COHb is below 5% and the patient is clinically asymptomatic. Nasal cannula alone is inadequate — a properly fitted non-rebreather mask is required to achieve near-100% FiO2.
Step 3: Hyperbaric Oxygen Therapy (HBO)
Hyperbaric oxygen involves breathing 100% oxygen inside a pressurized chamber at 2–3 atmospheres absolute (ATA). This treatment offers mechanistic advantages beyond simple acceleration of CO elimination:
- Faster CO elimination: The COHb half-life falls to approximately 20–30 minutes in the hyperbaric chamber — three to four times faster than NBO.
- Plasma-dissolved oxygen: At 3 ATA breathing 100% O2, enough oxygen dissolves directly in plasma to meet resting tissue oxygen requirements without any hemoglobin contribution — effectively bypassing the carboxyhemoglobin problem entirely.
- Cytochrome c oxidase recovery: HBO has been shown to displace CO from cytochrome c oxidase and restore mitochondrial respiratory function — addressing the cellular level of toxicity that NBO does not directly reverse.
- Reduction of lipid peroxidation and neuroinflammation: HBO inhibits neutrophil-mediated oxidative damage in the brain — the mechanism believed to underlie delayed neurological syndrome.
The landmark randomized controlled trial by Weaver et al. (2002, PMID 12362006) compared three sessions of HBO versus NBO in moderate-to-severe CO poisoning and demonstrated a significantly lower rate of cognitive sequelae at 6 weeks in the HBO group — providing the strongest prospective evidence for HBO's benefit beyond simple CO elimination.
Indications for HBO (Weaver criteria) include: any loss of consciousness or syncope; neurological signs or symptoms; COHb 25% or greater; cardiac involvement; and any symptomatic pregnant patient. Practical limitations — HBO chambers are not universally available, and transport time must be weighed against the clinical urgency and the time-sensitivity of the HBO benefit — require individualized judgment.
Supportive Care
Cardiac monitoring for arrhythmias and ischemia should be continuous in moderate-to-severe cases. Vasopressors are indicated for persistent hypotension after volume resuscitation. Benzodiazepines are first-line for seizures. Intravenous fluids are generally needed. Following apparent recovery, patients who had significant exposures must be observed and counseled regarding delayed neurological syndrome — they should not be discharged with the assumption that normal COHb levels mean they are safe from further neurological injury.
Delayed Neurological Sequelae
Delayed neurological sequelae (DNS) is one of the most distinctive and feared complications of CO poisoning — a neuropsychiatric syndrome that appears days to weeks after the patient has apparently recovered from the acute poisoning and been discharged home.
Definition and Incidence
DNS is defined as the emergence or re-emergence of neuropsychiatric symptoms occurring 2 to 28 days after an apparent clinical recovery from acute CO poisoning. Its incidence varies with exposure severity: it is rare after mild poisoning and occurs in 30–50% of patients with moderate-to-severe exposures who do not receive hyperbaric oxygen therapy. This makes it one of the most common serious late complications in emergency medicine.
Mechanism: Oxidative White Matter Injury
The pathophysiology involves a delayed inflammatory and oxidative cascade that injures cerebral white matter. CO exposure triggers lipid peroxidation in myelin-rich white matter, platelet activation, and neutrophil adhesion to brain microvascular endothelium — processes that continue after CO has been eliminated from the body. The result is a delayed demyelination of white matter tracts, with the globus pallidus being particularly vulnerable due to its high metabolic demand and vascular anatomy.
Clinical Features
DNS presents as a deterioration in neurological and cognitive function days to weeks after the patient appeared to have recovered. Common manifestations include: cognitive impairment (memory loss, confusion, difficulty concentrating, impaired executive function); personality changes (apathy, irritability, emotional lability); parkinsonian features (masked facies, shuffling gait, rigidity, tremor); urinary or fecal incontinence; and psychosis or frank dementia in severe cases. These deficits range from subtle and transient to severe and permanent.
Neuroimaging
MRI is the imaging modality of choice. Characteristic findings include bilateral symmetric T2/FLAIR hyperintensities in the white matter (periventricular and deep white matter) and basal ganglia lesions, particularly in the globus pallidus. These changes may be absent on MRI performed during acute poisoning and develop or become more pronounced in the weeks that follow — serial neuroimaging is often required for diagnosis.
The Role of Hyperbaric Oxygen in Prevention
The primary clinical argument for HBO therapy — beyond simply speeding CO elimination — is its evidence-based reduction in DNS incidence. The Weaver 2002 trial showed that HBO treatment reduced the rate of cognitive sequelae at 6 weeks from 46% (NBO group) to 25% (HBO group). This reflects HBO's mechanistic effect on interrupting the oxidative and inflammatory cascade responsible for delayed white matter injury, rather than simply removing CO faster. This is why HBO is recommended even for patients whose acute neurological symptoms have resolved with NBO, if their exposure qualifies by severity criteria.
Prognosis and Follow-Up
Most patients with DNS show partial improvement over months. Some patients make a full recovery; others are left with permanent cognitive deficits, personality changes, or movement disorder. Serial neuropsychological testing is important for documentation and management. Patients and families should be explicitly warned about DNS at the time of discharge and instructed to return immediately if new neurological or psychiatric symptoms develop.
Prevention: Detectors and Safety Rules
Carbon monoxide poisoning is almost entirely preventable. The interventions are straightforward, inexpensive, and highly effective — but they require education and consistent practice.
Carbon Monoxide Detectors
CO detectors are the most important single prevention tool for residential poisoning. They are now legally required in most US states for residential buildings, and their installation has measurably reduced CO mortality in jurisdictions that enforce detector laws. Best practices:
- Install on every level of the home, including the basement.
- Place detectors near sleeping areas — CO poisoning most often kills people in their sleep.
- Replace batteries annually; test monthly.
- Replace the detector unit every 5–7 years (electrochemical sensors degrade with age).
- If the detector alarm sounds: evacuate immediately, leaving the door open. Do not investigate the source, do not re-enter. Call 911 from outside. Do not return until emergency responders confirm it is safe.
Generator Safety
Portable generator misuse is the single most preventable cause of CO death in the United States. Never operate a generator indoors, in a garage, in a carport, in a porch, or near any window, door, or vent opening — even with the space ventilated. The minimum safe distance from any building opening is 20 feet. Before using a generator during an emergency, review this rule with every household member. The label "portable" does not mean "indoor-safe" — it means nothing about where it can be operated safely.
Annual Heating System Maintenance
All fuel-burning heating appliances — gas furnaces, boilers, oil furnaces, wood stoves, fireplaces — should be inspected annually by a licensed professional. Heat exchangers in gas furnaces crack with age and can leak combustion gases into circulating air. Chimney flues can become blocked by bird nests, debris, or ice, preventing combustion gases from venting. An annual service call before heating season begins is inexpensive insurance.
Garage Safety
Never idle a car in an attached garage, even briefly and even with the garage door fully open. CO diffuses through door frames and shared walls into the living space. Back the car out immediately before starting it. If the garage is directly connected to the home, installing a CO detector inside the home adjacent to the connecting door provides early warning of CO entry.
Grill Safety
Charcoal and propane grills must be used outdoors only — never in a garage, carport, screened porch, or tent, including during rain. Charcoal grills are particularly dangerous because they continue producing CO long after visible flames subside and charcoal appears spent.
Boat Safety
The US Coast Guard requires CO detectors on boats with enclosed spaces. Generator exhaust ports must be positioned and directed away from swim platforms, cockpits, and any area where people congregate. Never allow swimmers or passengers to loiter near generator exhaust ports while the generator is running.
Occupational Safety
Firefighters must use SCBA when entering any potentially CO-containing atmosphere. Workers in foundries, parking structures, metal-working facilities, and other high-exposure workplaces should have continuous ambient CO monitoring with audible alarms. Post-exposure COHb testing should be part of occupational health protocols for symptomatic workers.
After Any Significant Exposure
After any CO poisoning event, the building must be professionally inspected and the CO source identified and corrected before anyone re-enters. Fire departments and utilities typically provide free CO source investigation following a poisoning incident. Do not return to the building based only on CO detector levels falling — the underlying cause must be found and fixed.
Research Papers
The following peer-reviewed studies underpin current understanding of CO poisoning pathophysiology, diagnosis, and treatment.
- Weaver LK, Hopkins RO, Chan KJ, et al. Hyperbaric oxygen for acute carbon monoxide poisoning. N Engl J Med. 2002;347(14):1057–1067. PMID: 12362006
- Raub JA, Mathieu-Nolf M, Hampson NB, Thom SR. Carbon monoxide poisoning — a public health perspective. Toxicology. 2000;145(1):1–14. — Search PubMed
- Thom SR. Hyperbaric oxygen: its mechanisms and efficacy. Plast Reconstr Surg. 2011;127 Suppl 1:131S–141S. PMID: 21200283
- Hampson NB, Piantadosi CA, Thom SR, Weaver LK. Practice recommendations in the diagnosis, management, and prevention of carbon monoxide poisoning. Am J Respir Crit Care Med. 2012;186(11):1095–1101. — Search PubMed
- Miro O, Casademont J, Barrientos A, Urbano-Márquez A, Cardellach F. Mitochondrial cytochrome c oxidase inhibition during acute carbon monoxide poisoning. Pharmacol Toxicol. 1998;82(4):199–202. — Search PubMed
- Kao LW, Nañagas KA. Carbon monoxide poisoning. Emerg Med Clin North Am. 2004;22(4):985–1018. PMID: 15474779
- Scheinkestel CD, Bailey M, Myles PS, et al. Hyperbaric or normobaric oxygen for acute carbon monoxide poisoning: a randomised controlled clinical trial. Med J Aust. 1999;170(5):203–210. — Search PubMed
- Hampson NB, Hauff NM. Carboxyhemoglobin levels in carbon monoxide poisoning: do they correlate with the clinical picture? Am J Emerg Med. 2008;26(6):665–669. — Search PubMed
- Rose JJ, Wang L, Xu Q, et al. Carbon monoxide poisoning: pathogenesis, management, and future directions of therapy. Am J Respir Crit Care Med. 2017;195(5):596–606. PMID: 27753502
- Annane D, Chadda K, Gajdos P, Jars-Guincestre MC, Chevret S, Raphael JC. Hyperbaric oxygen therapy for acute domestic carbon monoxide poisoning: two randomized controlled trials. Intensive Care Med. 2011;37(3):486–492. — Search PubMed
- Wolf SJ, Lavonas EJ, Sloan EP, Jagoda AS; American College of Emergency Physicians. Critical issues in the management of adult patients presenting to the emergency department with acute carbon monoxide poisoning. Ann Emerg Med. 2008;51(2):138–152. PMID: 18206551
- Hampson NB, Weaver LK. Carbon monoxide poisoning: a new incidence for an old disease. Undersea Hyperb Med. 2007;34(3):163–168. — Search PubMed
For additional literature, search PubMed: carbon monoxide poisoning hyperbaric oxygen carboxyhemoglobin delayed neurological sequelae carbon monoxide pulse oximetry diagnosis
Connections
- Pulmonology
- Acute Respiratory Distress Syndrome (ARDS)
- Cardiology: Cardiac Complications
- Neurology: Brain Injury and Neurological Disease
- Addiction and Overdose
- Carbon Monoxide — the toxin page: sources, detectors, exposure limits.
- Chemical and Environmental Toxins
- Air Pollution and Lung Disease
- Rhabdomyolysis (CO can trigger muscle breakdown)
- Laboratory Tests and Diagnostics