Berylliosis (Chronic Beryllium Disease)
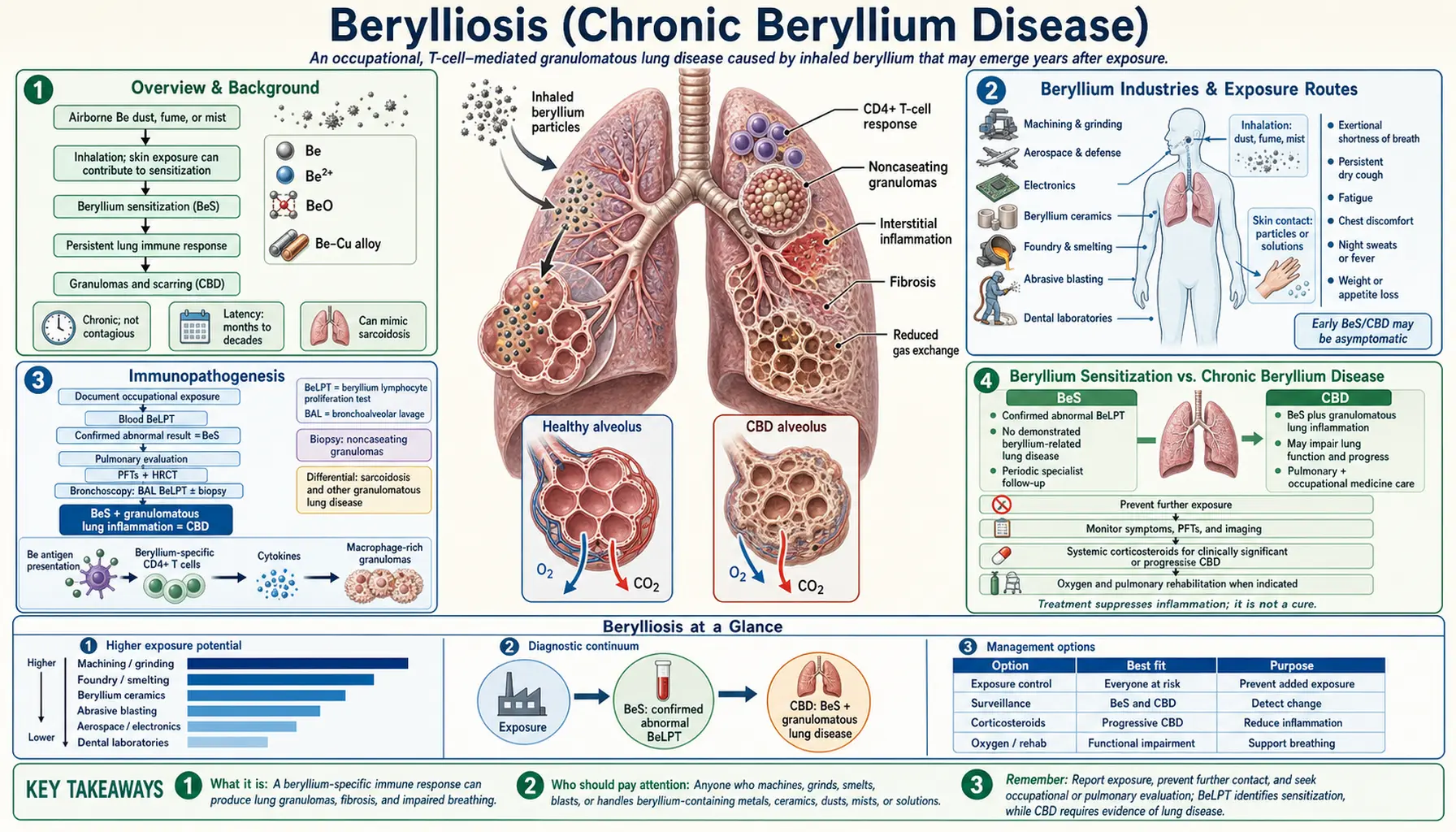
Berylliosis — formally called Chronic Beryllium Disease (CBD) — is an immune-mediated granulomatous lung disease caused by inhalation of or skin contact with beryllium metal, its alloys, or its compounds. Unlike most other occupational lung diseases, CBD is not a simple toxicity reaction but a T cell-mediated hypersensitivity triggered in genetically susceptible individuals. Beryllium (Be, atomic number 4) is the lightest alkaline earth metal and a strategically critical material used in aerospace alloys, nuclear reactors, defense electronics, and ceramics — industries where workers face ongoing exposure risk today. CBD closely resembles sarcoidosis on histology and imaging, making occupational history and the beryllium lymphocyte proliferation test (BeLPT) essential for accurate diagnosis. First recognized in the 1940s among workers in the early nuclear weapons and fluorescent lamp industries, CBD remains an important occupational disease wherever beryllium is processed, machined, or handled.
Table of Contents
- Overview & Background
- Beryllium Industries & Exposure Routes
- Immunopathogenesis
- Beryllium Sensitization vs. Chronic Beryllium Disease
- Clinical Features
- Diagnosis
- Treatment
- OSHA Regulations & Workers' Rights
- References
- Connections
- Featured Videos
Overview & Background
Chronic Beryllium Disease is classified among the pneumoconioses — occupational lung diseases caused by inhalation of dusts — but its mechanism sets it apart fundamentally from silicosis or coal workers' pneumoconiosis. Those diseases result from the direct toxic and inflammasome-activating properties of inorganic mineral particles depositing in lung tissue. CBD, by contrast, is a delayed-type (type IV) hypersensitivity reaction: the disease occurs only in individuals whose immune system has been sensitized to beryllium and subsequently mounts a sustained CD4+ T cell response when re-exposed. This immune-mediated pathogenesis means that CBD is in principle preventable not only by reducing exposure but also by identifying susceptible individuals — though that approach raises difficult ethical questions about genetic screening and employment discrimination.
Beryllium itself is remarkable as an engineering material. As the lightest structural metal with a very high stiffness-to-weight ratio, beryllium alloys (most commonly copper-beryllium, containing 1.8–2% Be) are approximately six times stiffer than steel at one-third the weight. These properties make beryllium alloys indispensable in aerospace structural components, precision instruments, x-ray windows, defense electronics connectors and springs, and nuclear moderator/reflector applications. Beryllium oxide (BeO) ceramics offer exceptional thermal conductivity at high temperatures, making them valuable in microelectronics and specialized industrial applications. This industrial utility means that despite the known health hazards, beryllium production and use continues globally, with the United States, Kazakhstan, and China as primary producers.
The first cases of CBD were recognized in the 1940s at factories producing fluorescent lamp phosphors (which used beryllium silicate) and in workers at United States Atomic Energy Commission (USAEC) facilities during the Manhattan Project, where beryllium was used as a neutron moderator and reflector. The early nuclear weapons program produced the first large cohorts of beryllium-exposed workers, and the resulting disease clusters drove both the initial recognition of CBD as a distinct entity and early regulatory efforts. The Beryllium Case Registry, established in 1952, was among the first systematic occupational disease registries in the United States.
Beryllium Industries & Exposure Routes
Beryllium exposure occurs in a range of industries wherever beryllium metal, alloys, or compounds are extracted, processed, fabricated, or machined. The critical determinant of risk is the generation of fine beryllium-containing particles or fumes small enough to be inhaled into the lower respiratory tract.
Primary Exposure Industries
- Aerospace manufacturing: Beryllium-copper (Cu-Be) alloys are used for structural components, springs, electrical connectors, and precision instruments in aircraft and spacecraft. Machining, grinding, and finishing of Cu-Be alloy parts generates beryllium-containing metal dust. Cu-Be alloys containing 2% Be are approximately six times stiffer than steel — a property that justifies their widespread use despite the health hazard and high cost.
- Nuclear industry: Beryllium serves as both a neutron moderator (slowing fast neutrons) and a neutron reflector (bouncing neutrons back into a reactor core) due to its very low neutron absorption cross-section — one of the lowest of any element. US Department of Energy weapons facilities (Los Alamos, Y-12, Rocky Flats, Hanford) employed large beryllium workforces; former DOE contractor workers with CBD may qualify for compensation under the Energy Employees Occupational Illness Compensation Program Act (EEOICPA).
- Defense electronics: Beryllium-copper alloys for precision springs, connectors, relay blades, and other small components in military and aerospace electronics. Secondary exposures occur during electronics assembly and repair.
- Ceramics and advanced materials: Beryllium oxide (beryllia, BeO) ceramics have exceptionally high thermal conductivity combined with electrical insulation, making them valuable as heat-sink substrates in power electronics and laser components. BeO dust from ceramic machining is highly toxic.
- Dental prosthetics: An under-recognized exposure source — beryllium-containing metal alloys (typically nickel-beryllium or cobalt-beryllium) have been used for cast crowns, bridges, and partial denture frameworks. Dental laboratory technicians who grind and polish these prosthetics face beryllium dust inhalation. CBD in dental laboratory workers has been documented but remains incompletely characterized epidemiologically.
- Beryllium mining and ore processing: Extraction of beryllium from its primary ore bertrandite (in Utah, the primary US source) and beryl involves crushing, milling, and hydrometallurgical processing steps that generate beryllium-containing dust and aerosols.
- Recycling and secondary processing: Recycling beryllium-containing scrap, especially Cu-Be alloys, at metal recycling facilities where workers may be unaware of beryllium content.
Exposure Routes
Inhalation is the primary route of concern for CBD. Fine beryllium particles and fumes generated during machining, grinding, melting, or abrasive finishing are the principal hazard. Particle size is critical: particles under 10 µm in aerodynamic diameter reach the lower airways; particles under 2.5 µm deposit in the alveoli where sensitization occurs.
Skin contact with beryllium-containing materials causes two distinct dermatological problems: contact dermatitis (an allergic reaction to soluble beryllium salts) and beryllium ulcers, which occur when soluble beryllium compounds penetrate abraded or cut skin, producing chronic non-healing granulomatous ulcers. Beryllium ulcers can develop from relatively minor skin punctures with beryllium-contaminated splinters or metal fragments.
Community (non-occupational) exposure has been documented near beryllium processing facilities. Residents living within several miles of beryllium plants have been found to have elevated rates of beryllium sensitization on BeLPT testing, suggesting that environmental contamination of soil and household dust can cause sensitization even without direct occupational contact.
Immunopathogenesis
The immunopathogenesis of CBD is unique among occupational lung diseases and has been studied intensively as a model of metal-induced immune activation. The central mechanism is an HLA class II-restricted, CD4+ T cell-mediated response to beryllium ions presented on antigen-presenting cells in the lung.
Beryllium as an Immune Antigen
Beryllium ions (Be2+) are not classical protein antigens but are extremely small inorganic ions. They can act either as a hapten — binding to self-proteins and generating novel antigenic epitopes — or, according to more recent structural studies, by directly inserting into the MHC class II peptide-binding groove and altering the groove's conformation to stimulate TCR binding. Crystallographic studies of HLA-DPB1 demonstrate that Be2+ ions coordinate with acidic amino acid residues (particularly glutamate at position 69, Glu69) within the antigen-binding cleft, physically deforming the groove and enabling TCR recognition of what is effectively a Be2+-modified self-peptide complex.
HLA-DPB1 Genetic Susceptibility
The critical genetic risk factor for beryllium sensitization and CBD is the presence of glutamic acid at position 69 of the HLA-DPB1 beta chain (HLA-DPB1 Glu69). Specific HLA-DPB1 alleles that carry this substitution — most importantly HLA-DPB1*0201 and HLA-DPB1*0401 — are present in approximately 30–50% of the general population and confer a 5- to 30-fold increased risk of beryllium sensitization upon exposure compared to individuals without Glu69. This association was first reported by Richeldi et al. in 1993 and subsequently confirmed in multiple independent cohorts across different beryllium industries.
Importantly, HLA-DPB1 Glu69 is necessary but not sufficient for CBD: many Glu69-positive individuals exposed to beryllium do not become sensitized, and a small minority of sensitized or CBD-confirmed individuals lack the Glu69 allele. Additional genetic modifiers (other HLA alleles, innate immune gene variants, TCR gene usage) and dose-response relationships with beryllium exposure level modify individual risk.
Granuloma Formation
Once a sensitized individual is re-exposed to beryllium-containing particles:
- Alveolar macrophages and dendritic cells phagocytose beryllium particles and present Be2+-modified peptide complexes on HLA-DPB1 to CD4+ T helper cells in the lung interstitium and bronchoalveolar space.
- Beryllium-specific CD4+ T cells are activated, producing IL-2 (T cell proliferation signal — the cellular basis of the BeLPT assay), IFN-γ, and TNF-α.
- IFN-γ activates macrophages into an M1-like pro-inflammatory state, driving secretion of additional TNF-α, IL-12, and reactive oxygen species.
- The sustained macrophage and T cell co-activation leads to the formation of non-caseating granulomas — organized aggregates of epithelioid macrophages, multinucleate giant cells, and T lymphocytes — indistinguishable from sarcoidosis granulomas on hematoxylin-eosin staining.
The granulomas of CBD are non-caseating (no central necrosis, in contrast to tuberculosis granulomas), but they progressively distort and fibrosis lung architecture over years to decades, leading to restrictive physiology, impaired gas exchange, and ultimately respiratory failure in severe cases. Beryllium particles can be detected within granuloma tissue using atomic absorption spectroscopy or energy-dispersive x-ray spectroscopy — a distinguishing feature when the diagnosis is uncertain.
Beryllium Sensitization vs. Chronic Beryllium Disease
Understanding the two-stage natural history of CBD is essential for clinical management and workplace surveillance programs.
Beryllium Sensitization (BeS)
Beryllium sensitization (BeS) is defined as a positive BeLPT result in a worker with no symptoms and no radiographic or pulmonary function abnormalities consistent with CBD. BeS indicates that the immune system has been primed to respond to beryllium — CD4+ T cells specific for beryllium-HLA complexes are present in circulating blood — but overt lung disease has not yet developed.
In beryllium-exposed workforces, approximately 10–15% of workers develop sensitization. Of sensitized individuals, an estimated 6–20% progress to CBD annually. This means that a sensitized worker has a meaningful and ongoing risk of developing overt disease each year, and cumulative conversion rates over a decade can be substantial. However, some sensitized individuals remain in the BeS state for many years or decades without progressing — current science cannot reliably predict who will progress.
Chronic Beryllium Disease (CBD)
CBD is defined by the combination of: (1) a documented history of beryllium exposure; (2) a positive BeLPT (blood or BAL); and (3) evidence of granulomatous inflammation on lung biopsy. Symptoms, radiographic findings, and pulmonary function abnormalities typically accompany CBD but are not required in all diagnostic frameworks — some cases are diagnosed at a subclinical stage through active surveillance.
Management Decisions at the BeS Stage
Whether to remove a sensitized but asymptomatic worker from beryllium exposure is one of the most contested questions in CBD occupational medicine. Arguments for removal: reducing ongoing antigenic stimulation may slow or prevent progression to CBD; arguments against: removal causes job loss and financial hardship, may not reliably prevent progression, and exposes the employer and occupational physician to difficult liability questions. Current US OSHA 2017 beryllium standards do not mandate removal of sensitized workers but do require enhanced surveillance and employer notification. Medical removal protection provisions apply only when a physician recommends removal based on individual clinical assessment.
Clinical Features
CBD is characterized by an insidious onset — patients often cannot identify a specific event triggering symptoms, and the disease may be discovered incidentally during workplace surveillance before symptoms develop.
Pulmonary Symptoms
The cardinal symptoms of symptomatic CBD are:
- Progressive dyspnea on exertion: typically the first and most prominent symptom; initially on significant exertion, gradually worsening to dyspnea at minimal activity in advanced disease
- Dry, nonproductive cough
- Chest tightness
- Fatigue and reduced exercise tolerance
- Weight loss: in more advanced disease
Long Latency
One of CBD's most clinically important features is its prolonged and variable latency period. Symptoms may first appear anywhere from a few years to 40 years after initial beryllium exposure. This means that workers who left beryllium-containing industries decades earlier may develop CBD long after they — and their physicians — have stopped associating their health with occupational exposures. A thorough lifetime occupational history asking specifically about beryllium-using industries is essential in any patient presenting with an idiopathic granulomatous lung disease.
Extrapulmonary Manifestations
Because CBD is a systemic immune-mediated granulomatous disease, extrapulmonary involvement can occur, mirroring the systemic manifestations of sarcoidosis:
- Bilateral hilar lymphadenopathy: common on chest imaging; reflects mediastinal granulomatous involvement
- Peripheral lymphadenopathy: less common than in sarcoidosis
- Hepatosplenomegaly: from hepatic and splenic granulomas; liver function tests may be mildly elevated
- Skin lesions: contact dermatitis from ongoing beryllium skin contact; subcutaneous nodules from granulomatous infiltration; beryllium ulcers — chronic non-healing granulomatous ulcerations at sites of skin penetration by beryllium-contaminated metal fragments
- Hypercalciuria and nephrolithiasis: granulomas produce 1,25-dihydroxyvitamin D (calcitriol) autonomously, leading to elevated intestinal calcium absorption and urinary calcium excretion; kidney stones may occur, mirroring this sarcoidosis complication
Prognosis and Disease Course
The natural history of CBD is highly variable and not reliably predictable from initial presentation. Some patients remain clinically and radiographically stable for many years after diagnosis. Others experience insidious but relentless progression to advanced fibrosis, severe restriction, hypoxemia, pulmonary hypertension, and cor pulmonale over one to two decades. No validated biomarker or clinical parameter at diagnosis reliably predicts which course an individual will follow. The granuloma burden on biopsy (number and size of granulomas) has been proposed as a prognostic marker but has not been prospectively validated.
Diagnosis
The diagnosis of CBD rests on three pillars: a history of beryllium exposure, a positive BeLPT, and demonstration of granulomatous inflammation. The key differential — sarcoidosis — produces clinically and histologically identical disease and can only be excluded by the first two pillars.
Beryllium Lymphocyte Proliferation Test (BeLPT)
The BeLPT is the cornerstone diagnostic and surveillance tool for beryllium sensitization and CBD:
- Blood BeLPT: Peripheral blood mononuclear cells (PBMCs) are isolated and incubated in culture wells with beryllium sulfate or beryllium fluoride at several concentrations. After several days, 3H-thymidine (radioactive thymidine) is added; proliferating T cells incorporate it into newly synthesized DNA. A stimulation index (SI) comparing beryllium-stimulated wells to unstimulated control wells is calculated. An SI ≥ 3.0 (or meeting laboratory-specific criteria for abnormal proliferation) is considered positive. Sensitivity for CBD is approximately 60–70%; specificity approximately 95%. False-negative blood BeLPTs occur because beryllium-specific T cells may be preferentially sequestered in the lung rather than circulating in blood.
- BAL BeLPT: Bronchoalveolar lavage lymphocytes are tested identically. BAL BeLPT has substantially higher sensitivity (~90%) for CBD than blood BeLPT because beryllium-specific T cells are concentrated in the bronchoalveolar compartment. A positive BAL BeLPT in the setting of granulomas on transbronchial biopsy confirms CBD diagnosis.
Bronchoscopy and Biopsy
Flexible bronchoscopy with transbronchial biopsy is performed in symptomatic patients or those with radiographic abnormalities to obtain tissue for histology. Findings in CBD include non-caseating epithelioid granulomas — compact clusters of activated macrophages (epithelioid cells), multinucleate giant cells (Langhans or foreign-body type), and a cuff of lymphocytes. These granulomas are histologically identical to sarcoidosis; beryllium cannot be identified on standard H&E staining. Atomic absorption spectroscopy or energy-dispersive x-ray analysis of biopsy tissue can detect beryllium directly, but these specialized analyses are available only at reference laboratories.
High-Resolution CT (HRCT)
HRCT findings in CBD overlap substantially with sarcoidosis:
- Bilateral hilar and mediastinal lymphadenopathy
- Perilymphatic nodules along bronchovascular bundles, interlobular septa, and subpleural regions
- Ground-glass opacity and consolidation in active inflammatory disease
- Septal thickening and architectural distortion in established fibrosis
- Upper lobe predominance typical of both CBD and sarcoidosis stage III/IV
Pulmonary Function Tests
Spirometry and diffusing capacity (DLCO) measurement assess functional impairment:
- Restriction: reduced TLC and FVC from fibrotic lung parenchyma
- Reduced DLCO: reflects impaired alveolar-capillary gas transfer; correlates with exercise desaturation and functional disability
- Mixed or obstructive pattern: may occur in patients with coexistent smoking-related obstructive disease
Key Differential: Sarcoidosis
Distinguishing CBD from sarcoidosis is one of the most important — and most commonly missed — diagnostic challenges in pulmonary medicine. The two diseases are clinically, radiographically, and histologically identical. The only reliable way to exclude CBD and confirm sarcoidosis is to demonstrate the absence of any history of beryllium exposure AND a negative BeLPT. Any patient diagnosed with sarcoidosis should be explicitly asked about occupational history in beryllium industries. Misdiagnosis of CBD as sarcoidosis removes the worker from workers' compensation eligibility, employer liability, and OSHA protections.
Treatment
Corticosteroids
Systemic corticosteroids are the mainstay of pharmacological treatment for symptomatic CBD with confirmed granulomatous inflammation. Prednisolone is typically started at 40 mg/day and tapered over months based on clinical, radiographic, and physiological response. Corticosteroids reduce granuloma burden, improve symptoms, and can stabilize or modestly improve pulmonary function test results. However, they do not cure CBD — granulomas and beryllium-specific T cells persist, and disease typically returns if corticosteroids are withdrawn. Side effects of long-term corticosteroid therapy (osteoporosis, diabetes, immunosuppression, adrenal suppression) must be carefully managed, particularly in older patients.
Steroid-Sparing Immunosuppressants
By analogy with sarcoidosis management, methotrexate (7.5–15 mg weekly) and azathioprine are used as steroid-sparing maintenance agents in patients who cannot tolerate adequate corticosteroid doses or who require prolonged treatment. These agents are used off-label in CBD based on sarcoidosis evidence; there are no large randomized trials specifically in CBD populations.
Beryllium Exposure Cessation
Upon diagnosis of CBD, cessation of all further beryllium exposure is mandatory. This may require job reassignment or — when reassignment within the facility is impossible — departure from a beryllium-using industry. Exposure cessation removes the antigenic trigger but does not reliably halt disease progression, particularly when established fibrosis is present. For workers with BeS only (no clinical CBD), the decision about removal is more complex and is discussed above.
Supportive and Rehabilitative Care
- Supplemental oxygen: for patients with resting hypoxemia (SpO2 <88% at rest) or significant exertional desaturation, per standard chronic lung disease guidelines
- Pulmonary rehabilitation: exercise training, dyspnea management techniques, and education to maintain functional capacity and quality of life
- Bronchodilators: for patients with coexistent obstructive physiology; no primary role in pure restrictive CBD
- Pneumococcal and influenza vaccination: to reduce risk of bacterial pneumonia in the setting of structural lung disease
Lung Transplantation
Bilateral lung transplantation is an option for patients with end-stage CBD who meet standard transplant eligibility criteria. Post-transplant outcomes appear comparable to transplantation for other forms of end-stage fibrotic lung disease. Beryllium particles may persist in mediastinal lymph nodes and residual macrophages after transplantation, but recurrence of granulomatous disease in the transplanted lungs has not been systematically documented.
Workplace Surveillance Programs
Secondary prevention through periodic BeLPT surveillance of beryllium-exposed workers is the most effective strategy for identifying sensitization before overt CBD develops. The US OSHA 2017 beryllium standard mandates BeLPT surveillance as part of the medical surveillance program for workers exposed at or above the action level. Annual BeLPT surveillance allows early detection of sensitization and informed decision-making about continued exposure before irreversible granulomatous fibrosis occurs.
OSHA Regulations & Workers' Rights
2017 OSHA Beryllium Standard
In January 2017, OSHA issued a comprehensive Beryllium Standard that substantially strengthened worker protections in three separate rules:
- 29 CFR 1910.1024: General industry (manufacturing, processing, ceramics, dental laboratories)
- 29 CFR 1926.1124: Construction
- 29 CFR 1915.1024: Shipyards
Key provisions of the 2017 standard:
- New Permissible Exposure Limit (PEL): 0.2 µg/m³ as an 8-hour time-weighted average (TWA) — reduced tenfold from the prior PEL of 2.0 µg/m³ that had been in place since 1971. The action level is 0.1 µg/m³ (8-hr TWA), triggering medical surveillance requirements.
- Short-Term Exposure Limit (STEL): 2.0 µg/m³ as a 15-minute TWA
- Mandatory medical surveillance: BeLPT offered to workers exposed at or above the action level for 30 or more days per year; periodic surveillance at least every 2 years; baseline spirometry and chest X-ray
- Employer-funded medical removal protection: when a physician recommends removal based on medical surveillance findings, the employer must transfer the worker to a non-beryllium work area while preserving earnings, seniority, and benefits for up to 6 months
- Beryllium work areas: designated areas with regulated access, decontamination facilities, and hygiene requirements
- Written exposure control plan: required for all workplaces where workers are or may be exposed to beryllium
NIOSH and ACGIH Exposure Limits
The NIOSH Recommended Exposure Limit (REL) for beryllium is 0.05 µg/m³ as a 10-hour TWA — substantially more stringent than the OSHA PEL, reflecting NIOSH's assessment that the 0.2 µg/m³ PEL does not eliminate CBD risk. The ACGIH Threshold Limit Value (TLV) for beryllium is 0.00005 mg/m³ (0.05 µg/m³), consistent with the NIOSH REL.
DOE EEOICPA Compensation
Former workers at US Department of Energy nuclear weapons facilities (and their survivors) who developed CBD may be eligible for compensation under the Energy Employees Occupational Illness Compensation Program Act (EEOICPA), which provides lump-sum cash benefits and medical coverage. The program recognizes CBD caused by DOE beryllium exposure as a covered occupational illness. Many former DOE contractor workers with long latency CBD were first diagnosed years or decades after leaving weapons facilities; EEOICPA provides a dedicated compensation pathway that does not require proving employer negligence.
Workers' Rights and Advocacy
Beyond OSHA and EEOICPA, beryllium-exposed workers have several important rights:
- The right to request OSHA inspection of a workplace with suspected beryllium hazards, on a confidential basis
- Access to industrial hygiene monitoring results and medical surveillance records kept by the employer
- Workers' compensation claims in all US states for medical expenses and wage replacement due to CBD
- The right to refuse removal from beryllium work without loss of employment protections when removal is medically recommended under the OSHA standard's medical removal protection provision
- In cases of employer negligence (failure to implement required controls, inadequate surveillance), civil litigation has produced substantial settlements for CBD victims and their families
Community Exposure and Environmental Regulation
The US Environmental Protection Agency (EPA) regulates beryllium as a hazardous air pollutant under the National Emission Standards for Hazardous Air Pollutants (NESHAP), with a beryllium air emission standard of 10 grams per 24-hour period for beryllium processing facilities. Community members living near beryllium processing plants can request EPA air monitoring data and participate in public comment processes for facility operating permits under the Clean Air Act.
References
- Henneberger PK, Cumro D, Deubner DD, et al. Beryllium sensitization and disease among long-term and short-term workers in a beryllium ceramics plant. Int Arch Occup Environ Health. 2001;74(3):167–176 — Search PubMed
- Newman LS, Mroz MM, Balkissoon R, Maier LA. Beryllium sensitization progresses to chronic beryllium disease: a longitudinal study of disease risk. Am J Respir Crit Care Med. 2005;171(1):54–60. PMID: 15976379
- Mroz MM, Kreiss K, Lezotte DC, Campbell PA, Newman LS. Reexamination of the blood lymphocyte transformation test in the diagnosis of chronic beryllium disease. J Allergy Clin Immunol. 1991;88(1):54–60 — Search PubMed
- Richeldi L, Sorrentino R, Saltini C. HLA-DPB1 glutamate 69: a genetic marker of beryllium disease. Science. 1993;262(5131):242–244 — Search PubMed
- Maier LA, Martyny JW, Liang J, Mroz MM. Recent chronic beryllium disease in residents surrounding a beryllium facility. Am J Respir Crit Care Med. 2008;177(9):1012–1017 — Search PubMed
- Kreiss K, Mroz MM, Newman LS, Martyny J, Zhen B. Machining risk of beryllium disease and sensitization with median exposures below 2 micrograms/m3. Am J Ind Med. 1996;30(1):16–25 — Search PubMed
- Stange AW, Furman FJ, Hilmas DE. The beryllium lymphocyte proliferation test: relevant issues in beryllium health surveillance. Am J Ind Med. 1996;30(4):453–463 — Search PubMed
- Fireman E, Kramer MR, Priel I, et al. Chronic beryllium disease among dental technicians in Israel. Isr Med Assoc J. 2006;8(7):461–463 — Search PubMed
- Fontenot AP, Falta MT, Savage AK, et al. Identification of pathogenic T cells in patients with beryllium-induced hypersensitivity. J Immunol. 2003;171(12):6996–7004 — Search PubMed
- Newman LS, Kreiss K, King TE Jr, Seay S, Campbell PA. Pathologic and immunologic alterations in early stages of beryllium disease. Am Rev Respir Dis. 1989;139(6):1479–1486 — Search PubMed
- Tinkle SS, Antonini JM, Rich BA, et al. Skin as a route of exposure and sensitization in chronic beryllium disease. Environ Health Perspect. 1997;105(10):1202–1203 — Search PubMed
- Cummings KJ, Stefaniak AB, Virji MA, Kreiss K. A reconsideration of acute beryllium disease. Environ Health Perspect. 2009;117(8):1250–1256 — Search PubMed
Connections
- Pulmonology
- Silicosis
- Asbestosis
- Hypersensitivity Pneumonitis
- Sarcoidosis
- Coal Workers' Pneumoconiosis
- Interstitial Lung Disease
- Rheumatoid Arthritis