Asbestosis
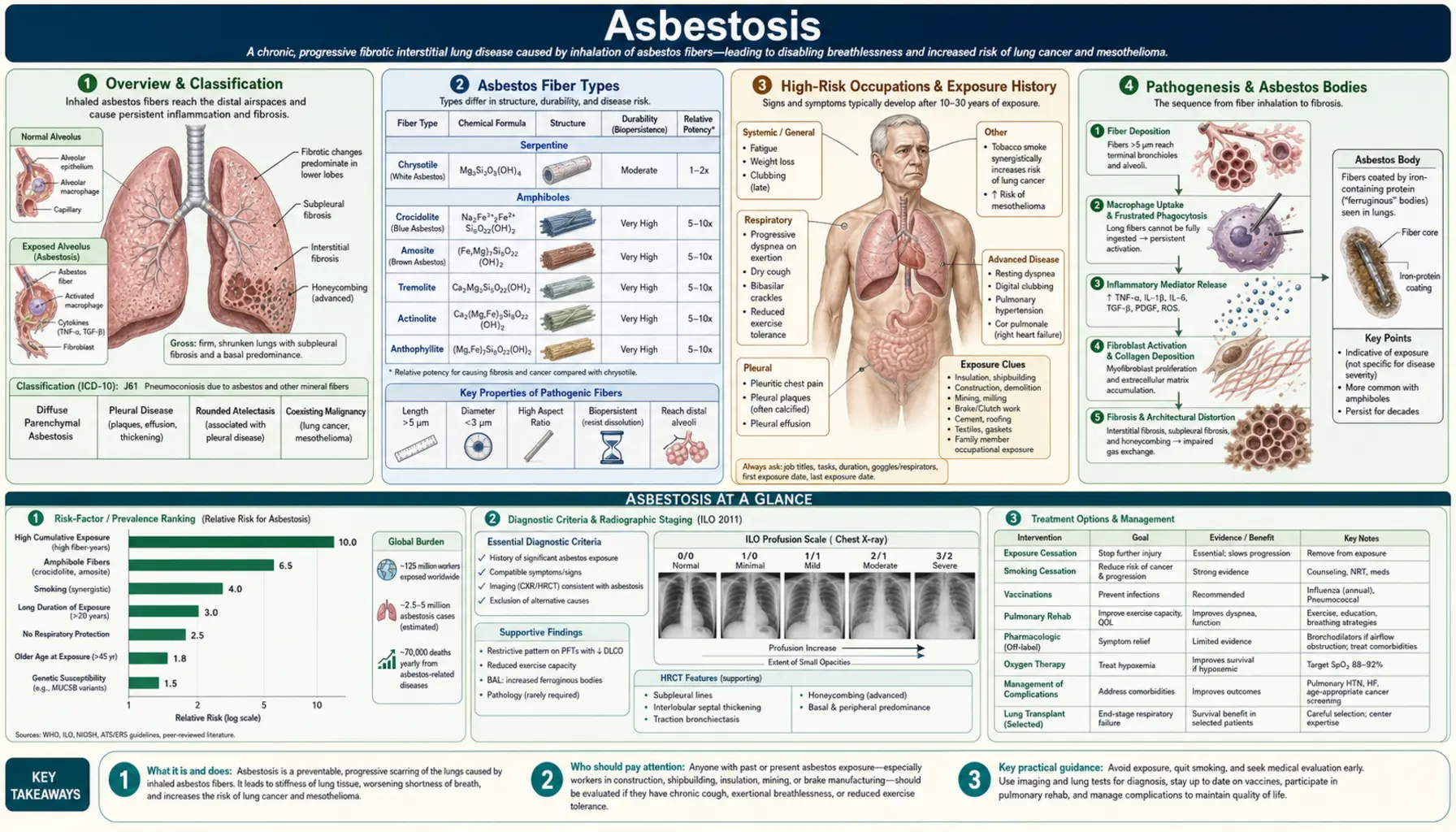
Asbestosis is a chronic, progressive, diffuse interstitial pulmonary fibrosis caused by prolonged inhalation of asbestos fibers. It develops after a latency period of 10–40 years following significant asbestos exposure and is characterized by bilateral lower-lobe fibrosis, restrictive lung physiology, and an elevated lifetime risk of lung cancer and malignant mesothelioma. Despite heavy restrictions on asbestos use in the United States since the 1980s, asbestosis and its related malignancies continue to cause tens of thousands of deaths annually worldwide due to the long latency and the ongoing legacy of decades of prior industrial and occupational exposure.
Table of Contents
- Overview & Classification
- Asbestos Fiber Types
- High-Risk Occupations & Exposure History
- Pathogenesis & Asbestos Bodies
- Pleural Disease
- Clinical Features & Pulmonary Function
- Diagnosis: HRCT, BAL & Helsinki Criteria
- Cancer Risks: Lung Cancer & Mesothelioma
- Treatment & Management
- References & Research
- Featured Videos
Overview & Classification
Asbestosis is defined as diffuse interstitial pulmonary fibrosis resulting from the inhalation and retention of asbestos fibers. The term is restricted to parenchymal fibrosis and does not encompass pleural disease (plaques, thickening, mesothelioma) or asbestos-related lung cancer — though all three can coexist in the same individual. The 2004 American Thoracic Society (ATS) diagnostic criteria require: (1) a reliable history of significant asbestos exposure; (2) appropriate latency between first exposure and disease onset (generally exceeding ten years); and (3) radiographic or histologic evidence of diffuse interstitial fibrosis.
Epidemiology
Asbestosis incidence closely tracks the industrial history of asbestos use. Peak use in the United States occurred between the 1930s and 1970s, fueling a wave of asbestosis diagnoses that continues today because of the disease's long latency. The United States Environmental Protection Agency estimates that between 1999 and 2013, asbestosis was listed as an underlying or contributing cause on approximately 40,000 death certificates in the US — roughly 2,500–3,000 deaths per year. Globally, the International Labour Organization estimated in 2006 that 107,000 workers die annually from asbestos-related diseases, including asbestosis, lung cancer, and mesothelioma. Developing nations where asbestos remains in use — notably Russia, China, Brazil, Kazakhstan, and India — face a growing epidemic that has yet to fully manifest given the latency period.
Distinction from Other Asbestos-Related Diseases
Asbestos causes a spectrum of pulmonary and pleural diseases that must be carefully distinguished. Asbestosis (parenchymal fibrosis) is dose-dependent — it requires cumulative heavy exposure — and its severity correlates with the total fiber burden. Malignant mesothelioma, by contrast, appears to have no safe threshold; even brief or low-level asbestos exposure has been implicated in mesothelioma. Benign pleural plaques are common markers of past exposure and are not themselves premalignant. Asbestos-related lung cancer requires synergistic assessment with smoking history.
Asbestos Fiber Types
Asbestos is a group of naturally occurring silicate minerals that share the property of forming long, thin, separable fibers. They are divided into two mineralogical families — serpentine and amphibole — with profoundly different biopersistence and pathogenic potential.
Serpentine Asbestos: Chrysotile
Chrysotile (white asbestos) is the sole member of the serpentine family and has historically accounted for more than 90% of all commercial asbestos use worldwide. Chrysotile fibers are curly, flexible, and relatively soluble in biological fluids — they are cleared from lung tissue more rapidly than amphibole fibers, with a biopersistence half-life measured in weeks to months. The curly morphology also makes chrysotile fibers less likely to penetrate deep into alveolar tissue compared to the straight, needle-like amphiboles. While chrysotile definitively causes both asbestosis and lung cancer, epidemiological and experimental data consistently indicate that it carries substantially lower mesothelioma risk per fiber than amphiboles. This distinction has been exploited in the "chrysotile defense" — arguments by the asbestos industry that chrysotile is acceptably safe — a position rejected by the International Agency for Research on Cancer (IARC), which classifies all asbestos fiber types as Group 1 carcinogens causing mesothelioma.
Amphibole Asbestos: Amosite, Crocidolite, and Tremolite
Amphibole asbestos fibers are straight, rigid, and needle-like. Their linear geometry enables deep penetration into the distal airways and alveoli, and their chemical composition makes them highly biopersistent — amphibole fibers remain in lung tissue for decades, sustaining chronic inflammation and genotoxic stress. Three amphibole types are particularly important:
- Amosite (brown asbestos): widely used in insulation and building materials; intermediate mesothelioma risk; the dominant fiber in many US shipyard and construction exposures.
- Crocidolite (blue asbestos): considered the most carcinogenic asbestos fiber type; straight, thin fibers with a half-life in lung tissue of decades; disproportionately responsible for mesothelioma relative to its volume of use; has been banned in most countries.
- Tremolite, anthophyllite, and actinolite: minor commercial uses but important as contaminants — tremolite contamination of talc deposits has been implicated in mesothelioma clusters among talc miners; tremolite contamination of chrysotile ore was historically significant at some mine sites.
Fiber Biopersistence and Pathogenic Potency
The single most important determinant of amphibole pathogenicity — particularly mesothelioma risk — is biopersistence: the ability to remain in lung and pleural tissue undegraded for years to decades. Amphibole fibers resist biodegradation by macrophage lysosomal enzymes, accumulating over time and providing a sustained source of reactive oxygen species (ROS), DNA strand breaks, and inflammatory signaling. The fiber dimensions (length >5 μm, diameter <3 μm) are critical — only fibers long enough to prevent complete engulfment by a single macrophage, yet thin enough to reach the pleura, drive the most severe pathology including mesothelioma.
High-Risk Occupations & Exposure History
Asbestosis is an occupational disease whose epidemiology mirrors the history of asbestos-using industries. Identifying a relevant occupational exposure history is essential to diagnosis — asbestosis does not develop from ambient environmental exposure at typical community levels.
Historically Highest-Risk Trades
The occupations carrying the highest historical asbestos exposure were those involving direct handling of raw asbestos or asbestos-containing insulation materials in enclosed spaces:
- Insulation workers: Among the highest-exposure groups; applied asbestos insulation to pipes, boilers, and ship compartments; cohort studies showed dramatically elevated asbestosis mortality.
- Shipyard workers: US naval shipyards from World War II through the Vietnam era were heavily asbestos-laden environments; workers in engine rooms and below-deck spaces received enormous cumulative exposures. Veterans who served aboard asbestos-insulated naval vessels also face elevated risk.
- Construction and demolition workers: Asbestos was used in floor tiles, ceiling tiles, spray-applied fireproofing, roofing materials, drywall joint compound, and pipe insulation from the 1940s through the 1970s. Renovation and demolition of pre-1980 buildings continues to generate asbestos exposure today.
- Pipe fitters and plumbers: Worked with asbestos-wrapped pipes and asbestos gasket materials.
- Electricians: Frequently worked in the same spaces as insulation workers and encountered asbestos-containing insulation boards and wiring conduit wrapping.
- Automobile mechanics: Historically handled asbestos-containing brake pads, clutch facings, and gaskets; brake drum grinding generated respirable asbestos dust. Chrysotile was the predominant fiber in friction materials, reducing but not eliminating risk.
- Asbestos miners and millers: The highest fiber-burden exposures occurred in mining and milling operations; workers at chrysotile mines in Quebec and crocidolite mines in Western Australia have been the subjects of landmark epidemiological cohort studies.
Regulatory History in the United States
OSHA established the first permissible exposure limit (PEL) for asbestos in 1972 and tightened it progressively thereafter — from 5 fibers/cm³ (1972) to 2 f/cm³ (1976) to the current 0.1 f/cm³ (1994). The EPA banned spray-applied asbestos-containing materials in 1973 and attempted a comprehensive ban in 1989, but the US Court of Appeals vacated most of the ban in 1991 (Corrosion Proof Fittings v. EPA). As a result, asbestos is not fully banned in the US; it remains permitted in specific uses including chlor-alkali diaphragms. The US is among a small minority of developed nations that has not enacted a comprehensive asbestos ban, though commercial use is now negligible.
Para-Occupational (Household) Exposure
Family members of asbestos workers — most often wives and children — were exposed to fibers brought home on work clothing. "Take-home" or para-occupational exposure has caused mesothelioma in household contacts and may be sufficient to cause asbestosis in heavily exposed individuals, particularly when the index worker handled raw asbestos or loose insulation. This represents a distinct epidemiological cohort that must be identified by careful social history when evaluating potential asbestos-related disease.
Pathogenesis & Asbestos Bodies
The pathogenesis of asbestosis involves a well-characterized sequence beginning with fiber deposition and culminating in progressive fibrogenesis, mediated by persistent macrophage activation and pro-fibrotic cytokine release.
Fiber Deposition and Macrophage Response
Inhaled asbestos fibers penetrate the mucociliary clearance system and deposit at alveolar duct bifurcations — the points of maximum impaction for long, rigid particles. Alveolar macrophages migrate to engulf the fibers in the process of phagocytosis. However, long asbestos fibers (particularly those exceeding 20 μm) exceed the macrophage's phagocytic capacity, resulting in "frustrated phagocytosis" — the macrophage cannot fully engulf the fiber and instead degranulates, releasing lysosomal enzymes, reactive oxygen species (superoxide, hydroxyl radical), and inflammatory cytokines directly into the surrounding alveolar tissue. This process is continuous as long as non-degradable fibers persist in the tissue, generating a state of chronic sterile inflammation.
Pro-Fibrotic Signaling Cascade
Activated macrophages and damaged epithelial cells elaborate a cascade of pro-fibrotic mediators. Transforming growth factor-beta 1 (TGF-β1) is the central fibrogenic cytokine — it activates lung fibroblasts and myofibroblasts, driving collagen synthesis and extracellular matrix deposition. Interleukin-13 (IL-13) amplifies the TGF-β1 response and promotes alternative macrophage activation, reinforcing the fibrotic phenotype. Tumor necrosis factor-alpha (TNF-α), platelet-derived growth factor (PDGF), and insulin-like growth factor-1 (IGF-1) contribute additional mitogenic and fibrogenic signals. The result is progressive replacement of alveolar architecture by fibrous tissue, beginning in the subpleural lower lobes and advancing centrally over years to decades.
Asbestos Bodies: The Pathognomonic Marker
Asbestos bodies are the histological hallmark of asbestos exposure. They form when a macrophage coats an asbestos fiber with a protein-iron complex (ferritin) in an unsuccessful attempt at neutralization. The resulting structure is a golden-brown, dumbbell- or drumstick-shaped body with a translucent central fiber core surrounded by beaded iron-protein deposits. Under light microscopy, asbestos bodies are visible in BAL fluid, sputum, and lung biopsy specimens. Key points:
- Asbestos bodies are pathognomonic of asbestos exposure — their presence confirms that the patient has inhaled asbestos fibers at some point.
- They are not pathognomonic of asbestosis — asbestos bodies are found in BAL fluid of people with past asbestos exposure who have no fibrosis. Their concentration does, however, correlate roughly with cumulative fiber burden.
- BAL asbestos body counts exceeding 1 body per mL of BAL fluid are considered indicative of significant asbestos exposure; counts exceeding 5/mL are strongly supportive.
- The vast majority of asbestos bodies form on amphibole fibers (particularly amosite and crocidolite), not on chrysotile, because the smaller, more biodegradable chrysotile fibers are cleared before coating is complete — a critical point in fiber-type attribution analyses.
Histopathology
The histological pattern of asbestosis is similar to usual interstitial pneumonia (UIP) — patchy subpleural fibrosis, honeycombing in advanced cases, fibroblastic foci — but is distinguished from idiopathic pulmonary fibrosis (IPF/UIP) by the presence of asbestos bodies, the characteristic lower-lobe subpleural distribution, and the clinical history. The Helsinki criteria (2014) formalized diagnostic thresholds for asbestos body counting in tissue sections required to attribute UIP-pattern fibrosis to asbestos exposure.
Pleural Disease
Pleural abnormalities are actually more common than parenchymal fibrosis among individuals with significant asbestos exposure and can appear at lower cumulative doses. Understanding benign pleural disease is critical for distinguishing it from malignant mesothelioma — a distinction with major prognostic and medicolegal implications.
Pleural Plaques: The Exposure Marker
Pleural plaques are discrete, well-demarcated areas of fibrous thickening on the parietal pleura (the lining of the chest wall and diaphragm, as opposed to the visceral pleura covering the lung surface). They are the most common manifestation of asbestos exposure, developing in 20–60% of heavily exposed workers with a latency of 20–30 years. Characteristic features on CT include:
- Bilateral distribution — unilateral plaques are uncommon with asbestos and more suspicious for other causes.
- Diaphragmatic plaques — involvement of the diaphragmatic pleura is highly characteristic of asbestos.
- Calcification — plaques frequently calcify over time, appearing as dense white opacities on chest radiograph or CT.
- Parietal pleural location — they arise from the chest wall lining, not the lung surface.
Pleural plaques are benign and not premalignant — they do not transform into mesothelioma and do not significantly impair lung function as isolated findings. They serve as a reliable marker of significant past asbestos exposure and their presence should prompt a thorough clinical evaluation for coexisting asbestosis and lung cancer surveillance.
Benign Asbestos Pleuritis
Some asbestos-exposed individuals develop an acute exudative pleural effusion — benign asbestos pleuritis — typically within the first 10–15 years after exposure onset, earlier than other asbestos-related diseases. The effusion is exudative, may be blood-tinged, and resolves spontaneously or with drainage, though it can recur. Its clinical importance lies in the differential diagnosis: a pleural effusion in a person with known asbestos exposure must be distinguished from malignant mesothelioma by appropriate cytological analysis and, if necessary, thoracoscopic biopsy.
Rounded Atelectasis
Rounded atelectasis (also called folded lung or Blesovsky syndrome) is a distinctive form of collapsed lung parenchyma associated with pleural fibrosis. Pleural thickening anchors and invaginates the adjacent lung, causing a rounded or wedge-shaped area of atelectasis with a characteristic "comet tail" sign on CT — the bronchovascular bundle curving toward the hilum. Rounded atelectasis can mimic a pulmonary mass on plain radiograph and must be distinguished from bronchogenic carcinoma. CT demonstration of the comet tail sign and pleural contact in an asbestos-exposed individual is usually diagnostic.
Diffuse Pleural Thickening
Diffuse pleural thickening (DPT) — continuous sheet-like fibrosis of the visceral or parietal pleura extending over a large area — is a more clinically significant form of pleural disease than discrete plaques. DPT can substantially restrict lung expansion, producing a restrictive ventilatory defect superimposed on any parenchymal fibrosis. When DPT fuses the visceral and parietal pleura (obliterating the pleural space), it may cause severe restriction and dyspnea disproportionate to any parenchymal changes. DPT does not transform into mesothelioma but must be distinguished from malignant pleural mesothelioma, which grows as a rind-like thickening of the pleura with a more nodular and irregular morphology on CT.
Clinical Features & Pulmonary Function
Asbestosis presents insidiously after a latency of typically 10–40 years from the onset of significant exposure. The severity of disease at presentation and its rate of progression correlate with cumulative fiber dose, fiber type, and individual susceptibility factors including smoking status.
Symptoms
Progressive exertional dyspnea is the cardinal symptom of asbestosis, reflecting the progressive restriction of lung expansion and impairment of gas exchange by advancing fibrosis. Dyspnea typically begins with strenuous exertion and advances to limitation with activities of daily living over years. Dry, non-productive cough is common. Unlike occupational asthma or hypersensitivity pneumonitis, asbestosis does not cause wheeze or episodic symptoms. Chest tightness may accompany exertion. In advanced disease, orthopnea and dyspnea at rest indicate severely compromised pulmonary reserve.
Physical Examination
The auscultatory hallmark of asbestosis is bilateral basilar inspiratory crackles, described as a "Velcro" quality — a fine, dry, end-inspiratory crackling sound, most prominent at the lung bases posteriorly. These crackles are indistinguishable from those of idiopathic pulmonary fibrosis. Digital clubbing — bulbous enlargement of the fingertips with loss of the normal angle between nail and nail bed — occurs in a minority of asbestosis patients (less commonly than in IPF) and when present indicates advanced fibrotic disease. Cyanosis at rest indicates end-stage disease with severe hypoxemia. Signs of pulmonary hypertension (loud P2, right ventricular heave, peripheral edema) may develop in advanced cases.
Pulmonary Function Tests
Pulmonary function testing in asbestosis characteristically shows a restrictive ventilatory pattern:
- Reduced FVC (forced vital capacity): the most sensitive functional marker of parenchymal fibrosis.
- Reduced TLC (total lung capacity): confirms true restriction rather than gas trapping.
- Normal or elevated FEV1/FVC ratio: preserved or supranormal ratio distinguishes restriction from obstruction. (Concurrent COPD from smoking can superimpose obstruction, producing a mixed pattern.)
- Reduced DLCO (diffusing capacity for carbon monoxide): impaired gas transfer across the thickened, fibrotic alveolar-capillary membrane; DLCO reduction is often the earliest functional abnormality and correlates with oxygen desaturation on exercise.
In some patients — particularly those with extensive pleural disease — the restrictive pattern may be more attributable to pleural thickening than parenchymal fibrosis; HRCT helps distinguish these contributions. Concurrent cigarette smoking may produce a superimposed obstructive defect, and asbestos-exposed workers with both smoking-related COPD and asbestosis may have a "near-normal" spirometry despite significant physiological impairment on exercise.
Distinguishing Asbestosis from Idiopathic Pulmonary Fibrosis
Asbestosis and IPF (idiopathic pulmonary fibrosis) share similar clinical presentations — bilateral basilar crackles, restrictive PFTs, similar HRCT patterns, and progressive decline. The critical distinguishing feature is the occupational history: asbestosis requires a history of significant asbestos exposure. HRCT may show pleural plaques in asbestosis, which are absent in IPF. On biopsy, asbestos bodies confirm asbestos exposure. In the absence of a clear occupational history and/or pleural plaques or asbestos bodies, the diagnosis of asbestosis cannot be made and IPF/UIP should be the working diagnosis.
Diagnosis: HRCT, BAL & Helsinki Criteria
The diagnosis of asbestosis is established through the integration of occupational exposure history, clinical findings, and radiological and, in selected cases, histological evaluation. No single test is pathognomonic; diagnosis requires synthesis across multiple domains.
High-Resolution CT (HRCT)
HRCT of the chest is the most sensitive imaging modality for detecting asbestosis and is preferred over plain chest radiography. The characteristic HRCT findings of asbestosis are:
- Bilateral lower-lobe reticular opacities: irregular linear densities, predominating in the subpleural posterior basal segments.
- Subpleural curvilinear lines: arcs of increased density paralleling the pleura within 1 cm of the pleural surface.
- Traction bronchiectasis: irregular bronchial dilatation caused by surrounding fibrotic traction — indicates established, irreversible fibrosis.
- Honeycombing: clustered cystic airspaces with thick fibrous walls in the subpleural lower lobes — indicates advanced disease.
- Pleural plaques: bilateral calcified parietal pleural plaques, particularly on the diaphragm — their presence markedly increases diagnostic confidence that the parenchymal changes represent asbestosis rather than IPF.
- Ground-glass opacities: may be present but are not a dominant feature; their presence can indicate an acute alveolitis superimposed on fibrosis or concurrent hypersensitivity pneumonitis.
All CT findings are characteristically most prominent below the level of the carina (hilum level), reflecting the lower-lobe predilection of asbestosis from fiber deposition physics.
Bronchoalveolar Lavage (BAL)
BAL can be performed to quantify asbestos body concentration as a measure of parenchymal asbestos burden. An asbestos body count exceeding 1 body/mL of recovered BAL fluid is considered indicative of significant asbestos exposure; counts of 5 or more per mL provide strong support. BAL can also reveal a lymphocytic or mixed alveolitis. BAL is not routinely required for diagnosis when HRCT findings and occupational history are concordant, but is useful in atypical cases or medicolegal contexts.
Helsinki Criteria (2014)
The updated Helsinki criteria (2014) provide a framework for causally attributing pulmonary fibrosis to asbestos exposure in both clinical and medicolegal contexts. Key thresholds include:
- Asbestos bodies in BAL: ≥1 asbestos body/mL (consistent with) or ≥5/mL (strong support).
- Asbestos bodies in tissue sections: ≥2 per cm² on iron-stained sections (consistent with), or ferruginous bodies with confirmed asbestos core.
- Uncoated asbestos fibers by analytical electron microscopy in tissue: amphibole fiber counts exceeding background laboratory levels.
- Occupational or para-occupational exposure history consistent with significant asbestos exposure.
The Helsinki criteria require that the observed lung fibrosis be of a UIP or asbestosis histological pattern, and that the fiber burden meets at least one of the quantitative thresholds. They also provide attribution guidance for lung cancer causation, requiring a combined exposure-fibrosis analysis.
Lung Biopsy
Surgical lung biopsy (VATS) is rarely required for asbestosis diagnosis when HRCT findings, occupational history, and BAL are concordant. It is indicated when the diagnosis is genuinely uncertain — for example, an atypical HRCT pattern without pleural plaques in a worker with uncertain exposure history, or when an alternative diagnosis (hypersensitivity pneumonitis, sarcoidosis, connective tissue disease-associated ILD) needs to be excluded. Biopsy shows the UIP or asbestosis histological pattern with asbestos bodies in tissue sections.
Cancer Risks: Lung Cancer & Mesothelioma
Asbestos is a potent carcinogen. Its most important oncological consequences are bronchogenic carcinoma (lung cancer) and malignant pleural mesothelioma — two of the most lethal thoracic malignancies. Understanding the distinct epidemiology and attribution of each is essential for clinicians managing asbestos-exposed patients.
Lung Cancer: Synergistic Risk with Smoking
Asbestos exposure significantly increases the risk of bronchogenic carcinoma across all major histological types (adenocarcinoma, squamous cell, small cell, large cell). The relative risk of lung cancer attributable to asbestos exposure alone (in non-smokers) is approximately 2-fold above background. However, the interaction between asbestos exposure and cigarette smoking is not merely additive — it is multiplicative (synergistic). A worker with significant asbestos exposure who smokes carries approximately 50-fold the lung cancer risk of a non-exposed, non-smoking individual, compared to roughly 10-fold for smoking alone and 2-fold for asbestos exposure alone. This synergism — formalized in the Helsinki criteria for attribution — means that smoking cessation in asbestos-exposed workers is among the most impactful preventive interventions possible. The mechanism involves asbestos-mediated impairment of mucociliary clearance, increased fiber retention with tobacco co-carcinogens, and direct genotoxic interactions between asbestos fibers and DNA.
Malignant Mesothelioma
Malignant pleural mesothelioma (MPM) is a highly aggressive cancer arising from mesothelial cells lining the pleura. Asbestos exposure — particularly to amphibole fibers — is the dominant causative factor in more than 80% of mesothelioma cases. Critically, mesothelioma has no established safe exposure threshold: even brief or low-level exposure to crocidolite or amosite has caused mesothelioma. The latency period from first exposure to clinical mesothelioma diagnosis is characteristically long — typically 20–50 years — meaning that workers exposed in the 1960s and 1970s continue to be diagnosed today. Mesothelioma's median survival from diagnosis was historically less than 12 months, though the combination of surgery (in selected patients), chemotherapy (cisplatin + pemetrexed), and newer immunotherapy agents (nivolumab + ipilimumab, FDA-approved 2020) has extended survival in a subset of patients.
Peritoneal Mesothelioma and Other IARC Group 1 Cancers
Peritoneal mesothelioma — arising from the lining of the abdominal cavity — accounts for approximately 20–30% of all mesotheliomas and is also causally linked to asbestos exposure. IARC's 2012 review classified all forms of asbestos as Group 1 carcinogens and identified sufficient evidence for causal associations with cancers of the larynx and ovary, in addition to the lung and pleura/peritoneum. The mechanism for ovarian mesothelioma may involve retrograde transport of inhaled or ingested asbestos fibers through the fallopian tubes to the peritoneal surface. These broader malignancy associations reinforce the importance of comprehensive cancer surveillance in heavily exposed individuals.
Lung Cancer Surveillance Considerations
Current low-dose CT (LDCT) lung cancer screening guidelines (USPSTF 2021) recommend annual LDCT for individuals aged 50–80 with a 20-pack-year smoking history who currently smoke or quit within the past 15 years. Asbestos-exposed workers meeting separate high-risk criteria may benefit from inclusion in surveillance programs, though no dedicated asbestos-exposure screening guideline has been universally adopted. Clinical practice guidelines from thoracic societies generally support offering LDCT surveillance to significantly asbestos-exposed individuals — particularly those with concurrent smoking history — given the multiplicative risk elevation.
Treatment & Management
There is currently no disease-modifying pharmacological therapy proven to halt or reverse asbestosis fibrosis. Management therefore focuses on preventing further exposure, managing symptoms, treating complications, and cancer surveillance — with smoking cessation as the single highest-yield intervention.
Exposure Cessation
Further asbestos exposure must cease immediately upon diagnosis. While the disease may continue to progress even after exposure ends — due to retained fibers sustaining chronic inflammation — continued exposure accelerates fibrosis and cancer risk. Workers should be removed from all asbestos-containing environments and assisted with occupational retraining or disability assessment. Employers are legally required under OSHA regulations to offer medical surveillance to workers with known significant asbestos exposure, including periodic chest radiography and spirometry.
Smoking Cessation
Smoking cessation is the most impactful intervention in asbestosis management, given the multiplicative increase in lung cancer risk conferred by the asbestos-smoking interaction. Every clinical encounter with an asbestos-exposed smoker should include brief cessation counseling and pharmacotherapy referral (varenicline, bupropion, nicotine replacement therapy). Cessation dramatically reduces but does not fully eliminate the residual lung cancer risk from asbestos exposure.
Symptom Management and Oxygen Therapy
Supplemental oxygen is indicated when resting arterial oxygen saturation falls below 88–90% or exercise oximetry demonstrates significant desaturation impairing functional capacity. Long-term oxygen therapy has been shown in COPD to improve survival and quality of life; while no asbestosis-specific trial exists, the physiological rationale and clinical practice guidelines support its use by analogy. Pulmonary rehabilitation — structured exercise training, breathing strategies, and nutritional support — improves exercise tolerance and quality of life, as demonstrated in IPF and other interstitial lung diseases. Opiates (low-dose oral morphine) may palliate refractory dyspnea in end-stage disease.
Vaccination
Respiratory infections are poorly tolerated in patients with asbestosis due to their limited pulmonary reserve. Current recommendations include annual influenza vaccination, pneumococcal vaccination (PCV15 or PCV20, plus PPSV23 per ACIP schedule), and COVID-19 vaccination with boosters per current guidance.
Surveillance Imaging and Monitoring
Serial pulmonary function tests every 6–12 months document disease progression and functional decline. Annual or biennial chest CT is appropriate for detecting new or progressive fibrosis, emerging malignancy, and pleural disease changes. Any new or enlarging pleural effusion or mass in an asbestos-exposed patient demands prompt thoracoscopic evaluation to exclude mesothelioma. LDCT lung cancer screening should be offered to eligible patients per smoking history criteria.
Compensation, Litigation, and Asbestos Trust Funds
Asbestos litigation represents one of the longest-running mass tort proceedings in US legal history, with billions of dollars paid through the courts and through pre-established asbestos bankruptcy trusts. More than 60 asbestos defendant companies have filed for bankruptcy and established federally supervised asbestos trust funds to compensate current and future claimants. Workers diagnosed with asbestosis or asbestos-related cancer may be entitled to workers' compensation through their state system, to Social Security Disability benefits, and/or to tort compensation through trust fund claims or lawsuits against product manufacturers. Clinical documentation — including a detailed occupational history, HRCT with findings consistent with asbestosis, and pulmonary function testing — is essential for legal proceedings and workers' compensation filings. Clinicians should refer patients to experienced occupational medicine specialists and plaintiff-side attorneys familiar with asbestos trust fund claim procedures.
Investigational Approaches
Because asbestosis shares its histopathological pattern (UIP/IPF) with idiopathic pulmonary fibrosis, anti-fibrotic therapies proven effective in IPF — nintedanib (a tyrosine kinase inhibitor targeting TGF-β, PDGF, and VEGF receptors) and pirfenidone (a TGF-β inhibitor with pleiotropic anti-fibrotic effects) — have been considered for asbestosis. No large randomized controlled trial has been completed specifically in asbestosis. Extrapolation from IPF data and the shared pathogenic mechanism have led some clinicians to offer these agents to patients with progressive asbestosis meeting IPF-analogous criteria, though regulatory approval specifically for asbestosis is lacking.
References & Research
- American Thoracic Society. Diagnosis and initial management of nonmalignant diseases related to asbestos. Am J Respir Crit Care Med. 2004;170(6):691–715 — Search PubMed
- Wolff H, Vehmas T, Oksa P, Rantanen J, Vainio H. Asbestos, asbestosis, and cancer, the Helsinki criteria for diagnosis and attribution 2014: recommendations. Scand J Work Environ Health. 2015;41(1):5–15 — Search PubMed
- Roggli VL, Gibbs AR, Attanoos R, et al. Pathology of asbestosis — an update of the diagnostic criteria: report of the Asbestosis Committee of the College of American Pathologists and Pulmonary Pathology Society. Arch Pathol Lab Med. 2010;134(3):462–480 — Search PubMed
- Akira M, Yamamoto S, Inoue Y, Sakatani M. High-resolution CT of asbestosis and idiopathic pulmonary fibrosis. AJR Am J Roentgenol. 2003;181(1):163–169 — Search PubMed
- Copley SJ, Wells AU, Rubens MB, et al. Functional consequences of pleural disease evaluated with chest radiography and CT. Radiology. 2001;220(1):237–243 — Search PubMed
- De Vuyst P, Dumortier P, Swaen GM, Pairon JC, Brochard P. Respiratory health effects of man-made vitreous (mineral) fibres. Eur Respir J. 1995;8(12):2149–2173 — Search PubMed
- Lee PN. Relation between exposure to asbestos and smoking jointly and the risk of lung cancer. Occup Environ Med. 2001;58(3):145–153 — Search PubMed
- Liu G, Cheresh P, Kamp DW. Molecular basis of asbestos-induced lung disease. Annu Rev Pathol. 2013;8:161–187 — Search PubMed
- Park EK, Takahashi K, Hoshuyama T, et al. Global magnitude of reported and unreported mesothelioma. Environ Health Perspect. 2011;119(4):514–518 — Search PubMed
- Kuempel ED, Wheeler MW, Smith RJ, Vallyathan V, Green FH. Contributions of dust exposure and cigarette smoking to emphysema severity in coal miners in the United States. Am J Respir Crit Care Med. 2009;180(3):257–264 — Search PubMed
- Lacourt A, Gramond C, Rolland P, et al. Occupational and non-occupational attributable risk of asbestos exposure for malignant pleural mesothelioma. Thorax. 2014;69(6):532–539 — Search PubMed
- Stayner L, Welch LS, Lemen R. The worldwide pandemic of asbestos-related diseases. Annu Rev Public Health. 2013;34:205–216 — Search PubMed
Connections
- Pulmonology
- Mesothelioma
- Silicosis
- Interstitial Lung Disease
- Lung Cancer
- Pneumothorax
- Pulmonary Arterial Hypertension
- Asbestos