Herniated Disc: History and Discovery
A herniated disc — also called a ruptured, prolapsed, or "slipped" disc — occurs when the soft inner core of an intervertebral disc pushes through a tear in its tougher outer ring and presses on a nearby spinal nerve root, producing back pain and the radiating leg pain known as sciatica. For most of medical history this everyday cause of suffering was completely misunderstood: such masses, when found at all, were taken for tumours of cartilage. The turning point came on 2 August 1934, when the Boston surgeons William Jason Mixter and Joseph S. Barr published a paper in the New England Journal of Medicine showing that a ruptured disc could compress the nerves of the spinal canal and that removing it could relieve sciatica. It was a genuine paradigm shift — and a modern caution follows it, because we now know that a great many disc herniations cause no pain at all. This page traces that story honestly, naming a discoverer or a date only where the historical record supports it.
Table of Contents
- What a Herniated Disc Is
- Before the Disc: Sciatica as an Ancient Mystery
- Schmorl and the Pathology of the Disc
- Early Surgeons: Kocher, Oppenheim, Krause, Goldthwait
- The 1934 Landmark: Mixter and Barr
- Why It Was a Paradigm Shift
- After 1934: Discectomy, MRI, and Microsurgery
- The Honest Nuance: Many Herniations Are Painless
- Legacy and Modern Understanding
- Research Papers and References
- Connections
- Featured Videos
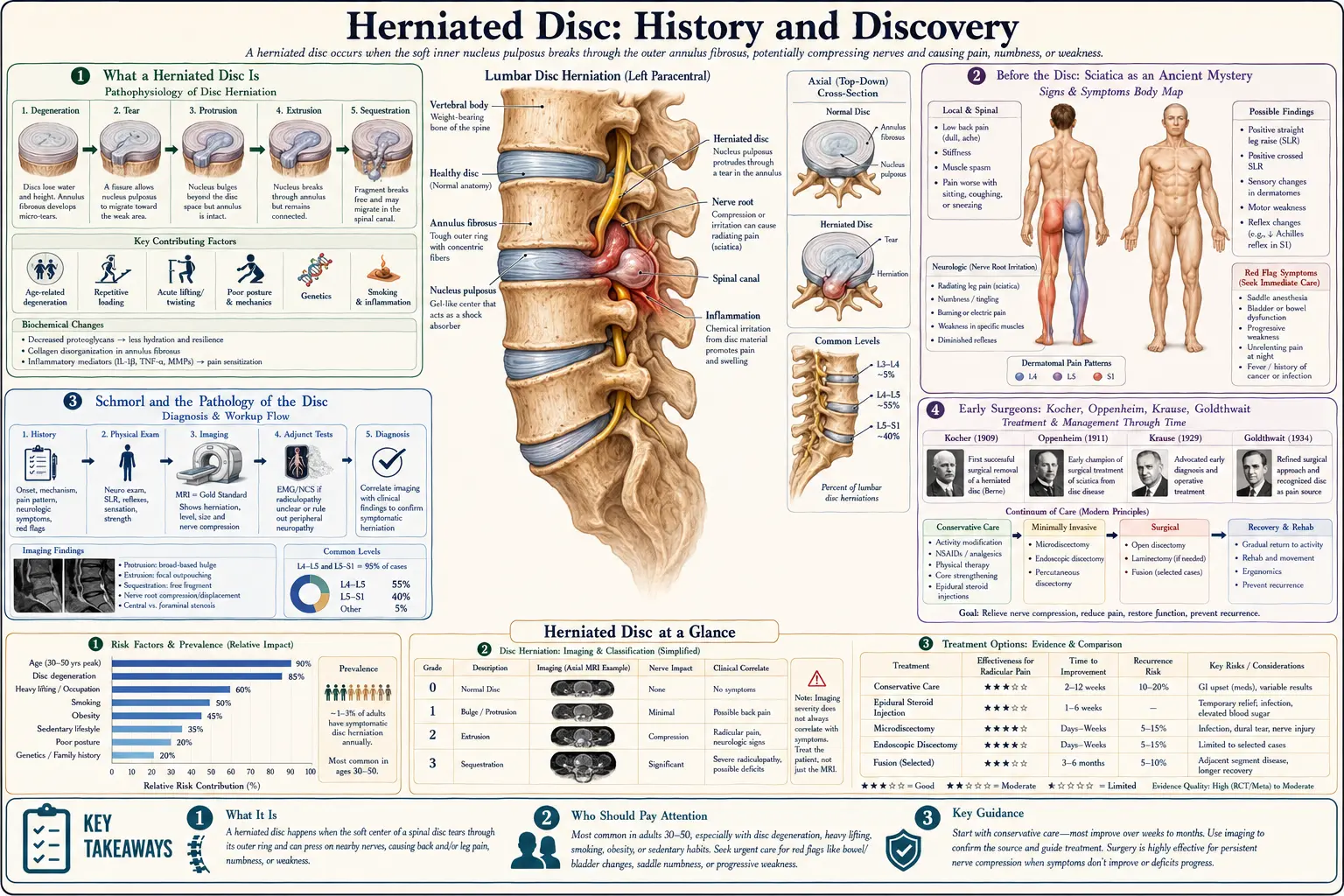
What a Herniated Disc Is
Between each pair of vertebrae in the spine sits an intervertebral disc, a small shock-absorbing cushion built like a jelly doughnut. The tough, layered outer ring is the annulus fibrosus; the soft, gel-like centre is the nucleus pulposus. When the annulus weakens or tears, the nucleus can bulge or squeeze out through the gap. If that displaced material presses on a spinal nerve root or on the spinal cord, it can cause pain, numbness, tingling, or weakness — classically pain that shoots down a leg (lumbar herniation, causing sciatica) or down an arm (cervical herniation).
The popular phrase "slipped disc" is anatomically misleading: the disc does not slip out of place like a coin from a stack. Instead, its inner material herniates — ruptures or protrudes — through the surrounding ring while the disc stays anchored to the vertebrae above and below. Understanding this simple mechanical picture is exactly what took medicine so long to achieve, because the disc is small, deeply buried, and was for centuries regarded as an inert spacer of no clinical importance.
This history matters because the modern names tell a story. "Rupture of the intervertebral disc," the phrase Mixter and Barr put in their 1934 title, was a deliberately mechanical description meant to displace the older, mistaken label of "tumour." Recovering how that re-description happened — and who saw pieces of the picture before it came together — is the subject of this page.
Before the Disc: Sciatica as an Ancient Mystery
The radiating leg pain we now call sciatica was described in antiquity — the term derives from the Greek ischias, referring to pain in the hip and thigh region — but its cause remained obscure for more than two millennia. Physicians from the classical era through the nineteenth century generally attributed sciatica to inflammation of the sciatic nerve itself ("sciatic neuritis"), to rheumatism, to gout, to "cold humours" settling in the hip, or to disorders of the hip joint. The idea that a small spinal cushion could be the culprit did not exist, because the disc was not yet understood as a structure that could fail mechanically and press on a nerve.
This long misattribution is an important part of the story, because it explains why the 1934 paper landed with such force. For centuries, treatment for sciatica targeted the wrong thing: the nerve was rubbed, blistered, stretched, rested, dosed, or operated on directly, because the prevailing theory said the problem lay in the nerve or the surrounding soft tissue rather than in a herniated disc compressing the nerve root at its origin in the spine. The historical record here is one of a persistent, well-described symptom without a correct mechanism — a gap that early disc researchers would slowly begin to close.
Nineteenth-century anatomists, including the towering German pathologist Rudolf Virchow, did observe and describe abnormal disc material in the spine. Virchow is often credited with an early-to-mid-nineteenth-century description of a traumatic disc protrusion, and a class of tumour-like cartilaginous masses came to be discussed under names such as "Virchow's tumour" in later literature. But these observations were framed pathologically — as growths or lesions — and were not connected to the living patient's sciatica or to the prospect of surgical relief. The clinical link was still missing.
Schmorl and the Pathology of the Disc
The most important pre-1934 figure in understanding disc pathology was the German pathologist Christian Georg Schmorl (1861–1932), who worked in Dresden and performed an enormous number of meticulous spinal autopsies and examinations. Through this systematic post-mortem work, Schmorl documented in unprecedented detail how intervertebral discs degenerate, fissure, and displace, and he described the now-eponymous Schmorl's nodes — protrusions of disc material vertically up or down through the cartilage endplate into the body of the adjacent vertebra, rather than backward toward the spinal canal. His characterisation of these nodes is generally dated to the late 1920s.
Schmorl's contribution was to establish, on a firm pathological footing, that disc material genuinely herniates — that the nucleus pulposus can and does escape its normal boundaries. This mattered enormously, because before this kind of careful disc pathology, masses found in or near the spinal canal had routinely been labelled and treated as tumours: enchondromas, chordomas, fibrochondromas, or osteochondritis. Schmorl's work helped reframe such material as displaced normal tissue rather than neoplasm, supplying the pathological foundation that the clinical breakthrough would later stand upon.
What Schmorl did not do — and this is the honest boundary of his contribution — was forge the clinical connection between a posteriorly herniated disc and the syndrome of sciatica in a living patient who could be cured by surgery. His genius was anatomical and pathological. He showed the medical world what a herniated disc is; it would fall to clinicians and surgeons to show what it does to a patient and what could be done about it. Schmorl's nodes themselves, it is worth noting, are usually symptomless incidental findings — an early hint of the painless-herniation theme that runs through this whole subject.
Early Surgeons: Kocher, Oppenheim, Krause, Goldthwait
Several clinicians glimpsed parts of the picture in the decades before 1934, and they deserve credit even though none assembled the full clinical synthesis. As early as 1896, the celebrated Swiss surgeon Emil Theodor Kocher (a future Nobel laureate) described, on post-mortem examination, the displacement of a lumbar disc in a man who had fallen from a height — an early documented link between trauma and disc rupture, observed at autopsy rather than treated in life.
In 1909, the German neurologist Hermann Oppenheim and the neurosurgeon Fedor Krause reported the surgical removal of what is now, in historical hindsight, recognised as a ruptured lumbar disc compressing the cauda equina. Crucially, however, Oppenheim and Krause did not understand it as a herniated disc: at the time they regarded the offending mass as a tumour-like growth (an enchondroma). Their operation is sometimes cited as the first removal of disc material, but it was performed under the old, mistaken conceptual framework — vivid proof that surgeons were physically encountering herniated discs decades before anyone correctly named what they were seeing.
On the clinical side, the Boston orthopaedic surgeon Joseph Goldthwait came strikingly close to the truth. In 1911, in the Boston Medical and Surgical Journal (the forerunner of the New England Journal of Medicine), Goldthwait discussed the lumbosacral region as an explanation for many cases of "lumbago," sciatica, and paraplegia, and is often credited with proposing that displacement of disc/annular tissue at the lumbosacral junction could compress nerve structures. He pointed at the mechanism, but the idea did not yet take hold in routine practice. Other figures, including the American neurosurgeon Charles Elsberg, also encountered and described such intraspinal masses in the years before 1934, often still under the tumour interpretation.
The pattern across all of these forerunners is consistent and worth stating plainly: the herniated disc was being seen, cut out, and even occasionally suspected as a cause of sciatica — but it was not yet correctly understood, named, and acted upon as a routine, surgically treatable entity. That final, decisive integration is what makes the 1934 paper a landmark rather than just one more case report.
The 1934 Landmark: Mixter and Barr
The decisive moment came at the Massachusetts General Hospital in Boston. William Jason Mixter, a leading neurosurgeon (and the hospital's first chief of neurosurgery), and Joseph S. Barr, an orthopaedic surgeon, collaborated across their two specialties — a combination that proved essential, pairing surgical access to the spinal canal with orthopaedic insight into the mechanics of the back. On 2 August 1934 they published "Rupture of the Intervertebral Disc with Involvement of the Spinal Canal" in the New England Journal of Medicine (volume 211, pages 210–215).
Their central argument was twofold and revolutionary. First, they contended that many masses in the spinal canal that had been diagnosed and treated as tumours — chondromas and the like — were in fact ruptured intervertebral discs: displaced normal disc tissue, not neoplasm. Second, and clinically most important, they established that such a ruptured disc could compress a spinal nerve root and so produce sciatica, and that surgically removing the herniated disc material relieved the pain. They supported the thesis with a surgical case series, demonstrating that the operation worked. The very title of the paper — "Rupture of the Intervertebral Disc" — was itself the corrective: a mechanical name to replace a mistaken oncological one.
The effect was immediate and lasting. Mixter is generally credited by his contemporaries as the person who best clarified the relationship between the intervertebral disc and sciatica, and the 1934 paper is repeatedly described in the modern surgical and neurosurgical literature as the work that fundamentally changed medicine's understanding of sciatica's cause. It launched what later authors have called "the dynasty of the disc" — an era in which the herniated disc became the leading explanation, and the operative target, for back-and-leg pain.
Why It Was a Paradigm Shift
It is worth pausing on why 1934 counts as a paradigm shift rather than an incremental advance, because the distinction is instructive. Before Mixter and Barr, two separate errors were entrenched. Pathologically, herniated disc material was misclassified as tumour — enchondroma, chondroma, chordoma — which framed it as a growth to be excised as a neoplasm rather than as a mechanical displacement. Clinically, sciatica was blamed on neuritis, rheumatism, or hip disease, which directed treatment toward the nerve, the joint, or the constitution rather than toward the disc compressing the nerve root.
Mixter and Barr corrected both errors at once and joined them into a single, actionable picture: a normal disc ruptures → the displaced material compresses a nerve root in the spinal canal → the patient feels sciatica → removing the material relieves the pain. By unifying pathology, clinical syndrome, and treatment in one causal chain, they did what none of the forerunners had managed. Kocher had the trauma link, Schmorl had the pathology of herniation, Goldthwait had the clinical suspicion, and Oppenheim and Krause had the surgery — but no one had put all four together correctly and demonstrated the cure. That synthesis is the essence of the breakthrough.
The change in mindset was so complete that, within a few years, "ruptured disc" went from a near-unknown concept to one of the most common explanations offered to patients with back and leg pain. As later historians of spine surgery have noted, the pendulum may even have swung too far, with the disc blamed for more pain than it actually causes — a corrective nuance that modern imaging would eventually supply, and which the final sections of this page address directly.
After 1934: Discectomy, MRI, and Microsurgery
After 1934, surgery to remove herniated disc material — discectomy — became an increasingly common operation for sciatica and for cervical disc disease, as surgeons developed approaches and instruments to reach the disc space and decompress the affected nerve root. For several decades the diagnosis rested on the clinical examination supplemented by myelography (injecting contrast dye into the spinal canal and taking X-rays to reveal a filling defect where a disc bulged in). Myelography was useful but invasive and imperfect.
The next great leaps were technical and refining. In the later twentieth century the operation was made far less destructive: the microdiscectomy, performed with an operating microscope through a small incision, allowed surgeons to remove only the offending fragment while sparing surrounding tissue, reducing the trauma of the older open laminectomy approach. Around the same era, chemonucleolysis (dissolving disc material by injecting an enzyme) was tried as a less-invasive alternative, with mixed long-term acceptance, and minimally invasive endoscopic techniques were later developed.
The most transformative diagnostic advance was magnetic resonance imaging (MRI), which became widely available in the 1980s. For the first time, clinicians could see the soft disc, the nucleus pulposus, the nerve roots, and a herniation directly, non-invasively, and in exquisite detail, without dye or radiation. MRI confirmed the reality of disc herniation in the living patient on a scale Mixter and Barr could only have dreamed of — and, almost immediately, it also delivered a humbling surprise that reshaped the whole field.
The Honest Nuance: Many Herniations Are Painless
Here is the part of the story that integrity demands be told plainly, because it directly affects how patients should interpret their own scans. When researchers used the new MRI technology to image the spines of people with no back pain at all, they found disc abnormalities — including frank herniations — in a startling proportion of perfectly comfortable individuals. A landmark 1990 study by Boden and colleagues found that roughly one in five asymptomatic people under sixty had a herniated nucleus pulposus on MRI, with abnormal findings far more common in older subjects. A widely cited 1994 study by Jensen and colleagues, examining people without back pain, reported that disc bulges or protrusions were present in a majority of them.
The implication is profound and is now mainstream in spine medicine: a herniated disc seen on imaging is not, by itself, proof of the cause of a person's pain. Herniations are common, often painless, and frequently shrink or resolve on their own over weeks to months as the body reabsorbs the displaced material. Many people walk around with disc herniations and never know it. This does not mean herniated discs never cause pain — when displaced material genuinely compresses or inflames a nerve root, the resulting sciatica is very real and sometimes severe. It means that the relationship between what a scan shows and what a patient feels is looser than the post-1934 enthusiasm assumed.
This nuance is the natural, honest endpoint of the history on this page. Mixter and Barr were right that ruptured discs can cause sciatica and that surgery can relieve it; that was a true and valuable discovery. But the pendulum swung so far that, for a time, the disc was over-blamed and over-operated. Modern, evidence-based practice restores the balance: it correlates imaging with the actual clinical picture, favours conservative care (time, activity, physical therapy, pain management) for most herniations because so many improve on their own, and reserves surgery for cases with clear, persistent nerve compression or serious neurological signs. The arc from "mysterious neuritis" to "everything is the disc" to "the disc, in context" is the real and continuing history of this condition.
Legacy and Modern Understanding
The legacy of the 1934 discovery is enormous and double-edged. On the one hand, Mixter and Barr opened a door that has relieved suffering for millions: the recognition that a herniated disc can be a surgically treatable cause of sciatica made effective, targeted relief possible for patients with genuine nerve compression, and it created the entire modern field of spinal surgery for disc disease. The collaboration between a neurosurgeon and an orthopaedic surgeon also foreshadowed today's multidisciplinary spine care.
On the other hand, the discovery's very success seeded the over-correction that MRI later exposed. Knowing both halves of the story — the genuine breakthrough and its limits — is what allows a patient today to read an MRI report mentioning a "disc herniation" without panic, and to ask the right question: not merely "is there a herniation?" but "does this herniation actually explain my symptoms, and what is the most conservative path to getting better?" The honest answer for most people is reassuring, because most herniations improve without surgery.
For the practical, patient-facing side of this condition — symptoms, causes, conservative treatment, when surgery is warranted, and recovery — see the main Herniated Disc article. The closely related leg-pain syndrome is covered in Sciatica, and the broader topic of living with persistent pain is addressed in Chronic Pain.
Research Papers and References
The list below combines the foundational primary papers in the history of the herniated disc with key modern studies on imaging and the asymptomatic-herniation nuance, plus curated PubMed topic-search links into the historical literature. The 1934 Mixter and Barr paper and the early-twentieth-century reports are named in the article as historical sources; where a confident DOI or PMID exists it is linked, and otherwise a PubMed topic search is provided. Each external link opens in a new tab.
- Mixter WJ, Barr JS. Rupture of the Intervertebral Disc with Involvement of the Spinal Canal. New England Journal of Medicine. 1934;211(5):210-215. — doi:10.1056/NEJM193408022110506
- Boden SD, Davis DO, Dina TS, Patronas NJ, Wiesel SW. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. Journal of Bone and Joint Surgery (American). 1990;72(3):403-408. — PMID: 2312537
- Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malkasian D, Ross JS. Magnetic resonance imaging of the lumbar spine in people without back pain. New England Journal of Medicine. 1994;331(2):69-73. — doi:10.1056/NEJM199407143310201
- Parisien RC, Ball PA. William Jason Mixter (1880-1958). Ushering in the "dynasty of the disc." Spine. 1998. — PubMed: Mixter and the dynasty of the disc
- Schmorl's nodes and the pathology of intervertebral disc herniation (Christian Georg Schmorl, 1861-1932) — PubMed: Schmorl disc pathology history
- Little-known Swiss contributions to lumbar disc disease before the Mixter and Barr era (Kocher; historical vignette) — PubMed: Swiss contributions before Mixter and Barr
- Oppenheim and Krause (1909) and the early surgical removal of disc material — PubMed: Oppenheim and Krause early disc surgery
- Goldthwait and the lumbosacral articulation as a cause of sciatica (1911) — PubMed: Goldthwait lumbosacral sciatica history
- A historical overview of sciatica — from antiquity to the disc — PubMed: history of sciatica and disc herniation
- History of the surgical management of herniated lumbar discs (discectomy to endoscopic surgery) — PubMed: history of lumbar discectomy
- Microdiscectomy and the evolution of minimally invasive lumbar disc surgery — PubMed: microdiscectomy history
- Natural history and spontaneous regression of lumbar disc herniation — PubMed: spontaneous regression of disc herniation
- Prevalence of asymptomatic disc abnormalities on spine imaging in the general population — PubMed: asymptomatic disc findings on MRI
- Rudolf Virchow and early descriptions of traumatic disc protrusion — PubMed: Virchow and early disc descriptions
External Authoritative Resources
- NINDS (National Institute of Neurological Disorders and Stroke) — Back Pain
- MedlinePlus — Herniated Disk
- PubMed — All research on intervertebral disc herniation
Connections
- Orthopedics
- Herniated Disc (Main Article)
- Sciatica
- Chronic Pain
- Carpal Tunnel Syndrome
- Tendinitis
- All Conditions