Compartment Syndrome
- Overview
- Pathophysiology — The Pressure-Ischemia Cycle
- Causes and Risk Factors
- Anatomy of the Four Lower Leg Compartments
- The Six Ps — Clinical Signs
- The Critical Importance of Passive Stretch
- Compartment Pressure Measurement
- Fasciotomy — Surgical Emergency
- Chronic Exertional Compartment Syndrome
- Complications of Missed or Delayed Diagnosis
- Key Research Papers
- PubMed Research Searches
- Connections
Overview
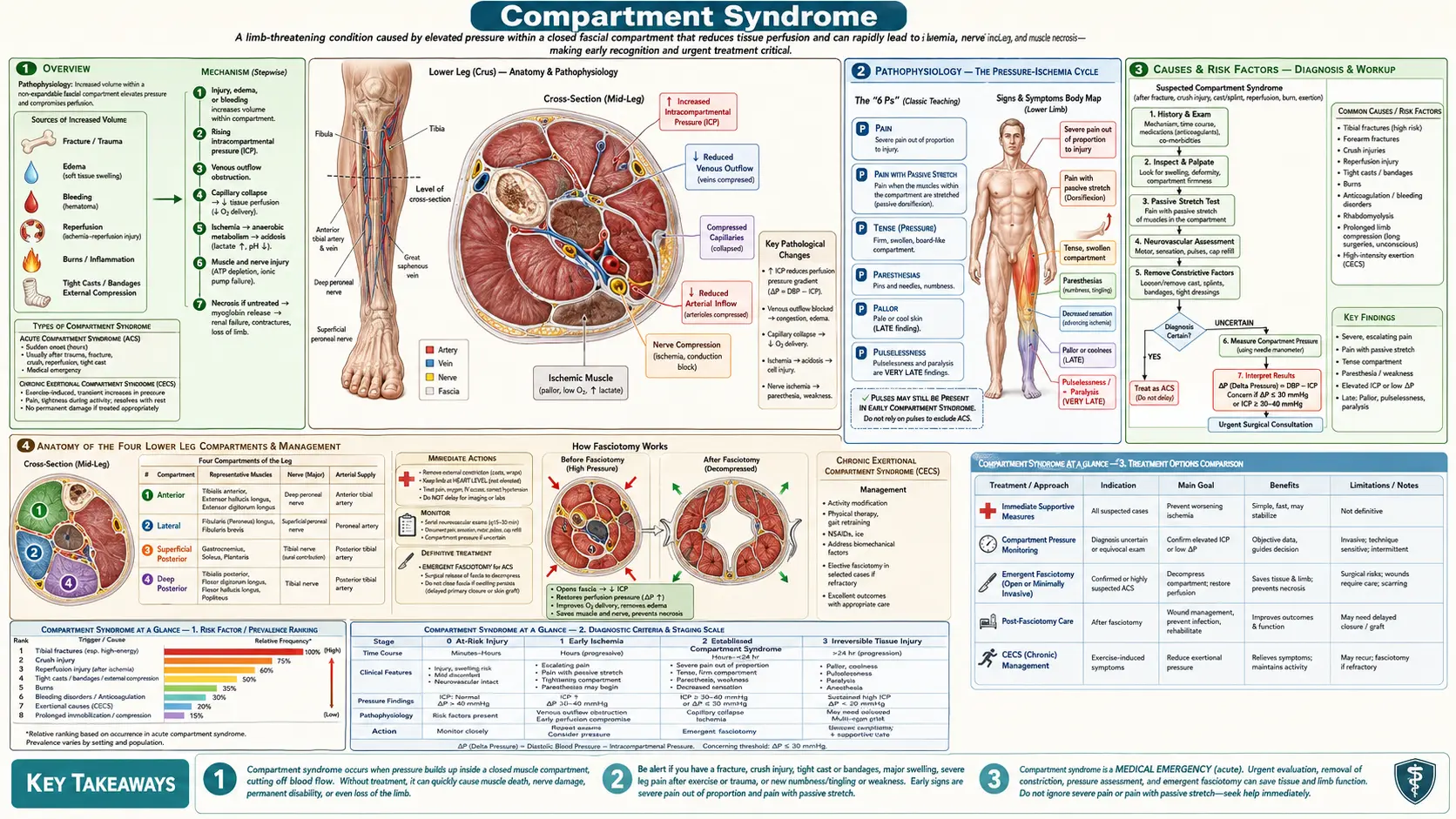
Compartment syndrome is one of the true surgical emergencies in orthopedics — a condition where elevated pressure within a closed fascial compartment compromises the circulation and perfusion of the tissues inside that compartment, leading to ischemia and ultimately irreversible muscle and nerve necrosis. The diagnosis is clinical, the window for limb-saving treatment is narrow (6–8 hours before permanent damage), and the treatment is unambiguous: immediate surgical decompression (fasciotomy).
Delays in diagnosis — whether from inadequate examination, over-reliance on absent pulses as a late sign, sedation, or the false reassurance of a cast that seemed tight "but not that tight" — are the most common source of catastrophic outcomes, including permanent foot drop, Volkmann's contracture of the forearm, amputation, and multi-organ failure from rhabdomyolysis. Acute compartment syndrome is a time-sensitive emergency every bit as urgent as myocardial infarction or stroke: the window between early ischemia and irreversible necrosis is measured in hours, not days.
It is important to understand both acute compartment syndrome (a true surgical emergency following trauma or reperfusion injury) and chronic exertional compartment syndrome (a separate, benign, exercise-induced condition that resolves with rest and is managed conservatively or with elective surgery). These two conditions share a name and a mechanism but have completely different urgency profiles, prognoses, and management pathways.
The limbs most commonly affected are the lower leg (four compartments, with the anterior and deep posterior compartments most vulnerable) and the forearm (two compartments, where missed diagnosis leads to Volkmann's contracture). Children are at special risk following supracondylar humeral fractures — the small forearm compartments can develop ischemia rapidly after brachial artery injury. Adults most commonly develop compartment syndrome after tibial shaft fractures, crush injuries, or reperfusion following arterial surgery. Any clinician who manages traumatic injuries must maintain a very high index of suspicion and act decisively when the clinical picture is suggestive.
Pathophysiology — The Pressure-Ischemia Cycle
The fascial compartments of the limbs are anatomically closed spaces — bounded by the relatively inelastic fascia with fixed bony boundaries at their base. Unlike subcutaneous tissue or abdominal organs that can expand outward when swelling occurs, the contents of a fascial compartment have nowhere to go. Within these compartments, pressure rises when either (a) the volume of contents increases — from edema, bleeding, inflammation, or the physiological muscle swelling of intense exercise — or (b) the compartment becomes externally compressed, as occurs with a tight circumferential cast, circumferential burns, or military antishock trousers (MAST).
As intracompartmental pressure rises, it first compresses thin-walled veins, which have the lowest intraluminal pressure of any vessel. Venous outflow obstruction causes capillary back-pressure to rise, which causes fluid to transude further into the compartment, which raises pressure still further. This is a rapidly self-reinforcing vicious cycle: edema begets pressure, pressure begets more edema, and the process escalates toward critical ischemia within hours.
The key physiological formula that guides clinical thinking is: PERFUSION PRESSURE = Diastolic Blood Pressure − Compartment Pressure. This difference is called the "delta pressure" (ΔP). When ΔP falls below approximately 30 mmHg, capillary perfusion pressure is insufficient to sustain tissue oxygenation and ischemia begins. This formula explains a critical and frequently misunderstood point: a hypotensive patient (diastolic BP 40 mmHg) can develop critical tissue ischemia with a compartment pressure of only 20 mmHg (ΔP = 20), while a healthy normotensive patient (diastolic 80 mmHg) might tolerate a compartment pressure of 40 mmHg (ΔP = 40) with only borderline ischemia.
The sequence of tissue vulnerability from ischemia follows a predictable pattern: nerve function deteriorates first (paresthesias appear within 30 minutes of ischemia), followed by muscle ischemia (pain and weakness), and finally irreversible muscle necrosis (within 4–8 hours of complete ischemia). The critical clinical implication is that arterial pulses remain palpable until compartment pressure approaches systemic arterial systolic pressure — which is very late in the disease course. By the time distal pulses are absent, irreversible muscle necrosis has typically been underway for one to two hours. Relying on the absence of pulses as a trigger for intervention is a potentially catastrophic error that remains one of the most common causes of missed compartment syndrome lawsuits.
Causes and Risk Factors
Fractures are the dominant precipitating cause of acute compartment syndrome overall. Tibial shaft fractures are the most common single precipitant — approximately 2–9% of closed tibial fractures develop compartment syndrome, and open fractures carry a similar (not lower) risk; the presence of an open fracture wound provides a false sense of security since the skin opening does not adequately decompress the underlying fascial compartments. Radius and ulna fractures can precipitate forearm compartment syndrome, and supracondylar humeral fractures in children — particularly those with anterior interosseous artery injury — can lead to Volkmann's ischemic contracture of the forearm if not recognized promptly.
Crush injuries from motor vehicle accidents, industrial presses, heavy falling objects, or prolonged limb compression (such as a person found unconscious lying on their own limb) cause direct muscle trauma, massive edema, and often concurrent rhabdomyolysis — all of which raise compartment pressure simultaneously from multiple mechanisms.
Circumferential compressive dressings or casts represent one of the most preventable causes of iatrogenic compartment syndrome. Any circumferential compressive dressing or cast applied after trauma in a swollen extremity can compress the underlying compartments as swelling progresses over the subsequent 24–48 hours. Standard of care requires that circumferential casts in the acute post-injury period either be applied with adequate padding and with patient education to return immediately for any escalating pain, or be bivalved (split longitudinally from top to bottom on both sides) and spread apart if escalating pain develops.
Burns — circumferential full-thickness burns cause the eschar (burned skin and subcutaneous tissue) to become inelastic and compressive as the underlying tissues swell; the procedure required is escharotomy (longitudinal incision through the eschar) rather than fasciotomy, though severe burns may require both.
Rhabdomyolysis from any cause can produce sufficient muscle swelling to precipitate compartment syndrome. Sources include prolonged limb compression (a drug-overdose patient found after hours on a hard surface), seizures (sustained muscle contraction), hyperthermia (heat stroke, neuroleptic malignant syndrome, malignant hyperthermia), extreme exertion (ultra-marathon runners, military trainees), and direct myotoxins (statins in rare cases, alcohol in high doses).
Reperfusion injury after arterial surgery or thromboembolism is a high-risk scenario. When blood flow is restored to a limb that has been ischemic for more than 4–6 hours, the sudden influx of oxygen-rich blood to metabolically stressed muscle causes massive reactive hyperemia and edema — the reperfusion syndrome. Prophylactic fasciotomy at the time of arterial reconstruction is standard when ischemia time is prolonged.
Bleeding disorders and anticoagulation — patients on warfarin, direct oral anticoagulants, or with hemophilia can develop spontaneous or traumatic compartment syndrome from hemarthrosis or intramuscular hematoma expansion. The iliopsoas compartment is the most common site of spontaneous compartment syndrome in patients on anticoagulation.
Positional compartment syndrome — "well-leg compartment syndrome" occurs in patients placed in prolonged lithotomy position (common in gynecological, colorectal, and urological surgeries lasting 4+ hours). The lateral compartment of the leg bears the brunt of compression. Surgeons and anesthesiologists must monitor operative time and leg position carefully in these cases.
Anatomy of the Four Lower Leg Compartments
The lower leg has four fascial compartments, each bounded by the tibia, fibula, interosseous membrane, and surrounding fascia. Understanding which nerve and which vessels traverse each compartment is essential for predicting the clinical neurological deficit that will result from ischemia and for planning the correct surgical approach.
Anterior Compartment — the most frequently involved compartment in acute compartment syndrome. Contains the tibialis anterior (dorsiflexes ankle), extensor hallucis longus (extends big toe), extensor digitorum longus (extends toes 2–5), and peroneus tertius. The anterior tibial artery and deep peroneal nerve run through this compartment. Ischemia of the deep peroneal nerve causes loss of sensation in the first web space of the dorsum of the foot (between the first and second toes) — this is the earliest and most reliable sensory finding. Motor ischemia causes progressive weakness of ankle dorsiflexion and toe extension, culminating in the irreversible foot drop of missed compartment syndrome. On examination, pain in the anterior shin on passive plantarflexion of the ankle is the key test.
Lateral Compartment — contains the peroneus longus and peroneus brevis (both evert the foot and plantarflex the ankle). The superficial peroneal nerve traverses this compartment, providing motor supply to the peroneal muscles and sensory supply to most of the dorsum of the foot. Isolated lateral compartment syndrome is less common than anterior; it most often occurs in conjunction with anterior compartment involvement. Sensory loss on the dorsum of the foot (aside from the first web space) suggests superficial peroneal nerve involvement.
Deep Posterior Compartment — arguably the most clinically consequential compartment because it contains the posterior tibial vessels (a major blood supply to the foot) and, critically, the tibial nerve. The tibial nerve provides motor supply to the foot intrinsics and the long toe flexors, and sensory supply to the entire plantar (sole) surface of the foot. It also contains the flexor hallucis longus, flexor digitorum longus, and tibialis posterior. Ischemia here causes paresthesias or numbness on the plantar foot — a finding that must never be dismissed as "normal post-fracture discomfort." To test this compartment clinically, passive dorsiflexion of the ankle and extension of the toes stretches the flexors and produces exquisite pain in the deep posterior calf.
Superficial Posterior Compartment — the largest and most tolerant compartment, containing the gastrocnemius (two heads) and soleus (the dominant plantarflexors of the ankle) plus the plantaris. The sural nerve (sensory to the lateral foot and heel) traverses this compartment. Because of the large muscle bulk and more compliant fascia here, this compartment tends to tolerate pressure rises better than the other three; isolated superficial posterior compartment syndrome is uncommon except in severe crush injuries.
In the forearm, the two clinically critical compartments are the volar (flexor) compartment — containing the finger and wrist flexors plus the median and ulnar nerves — and the dorsal (extensor) compartment. The volar compartment is almost always the one at risk; missed volar compartment syndrome leads to Volkmann's ischemic contracture, with fixed flexion of the fingers and wrist from fibrosis of the ischemic flexor muscle bellies. Carpal tunnel release is often performed simultaneously with forearm fasciotomy because the median nerve at the wrist is at added risk from venous hypertension transmitted distally. The hand contains ten individual compartments (four dorsal interossei, three palmar interossei, thenar, hypothenar, and adductor pollicis), all of which may require individual release in severe crush injuries to the hand.
The Six Ps — Clinical Signs
The classical teaching framework for the clinical features of acute compartment syndrome is the "6 Ps." However, these signs are not of equal reliability or equal timing — the first two (Pain and Pressure) are early and universally present, paresthesias are the most important early neurological sign, while pallor and pulselessness are dangerously late. Understanding the hierarchy of these signs prevents the cognitive trap of waiting for a "complete" clinical picture before acting.
Pain — the cardinal symptom and the first to appear. The pain of compartment syndrome is severe, burning, or deep aching in quality, located in the compartment itself (not just at the fracture site), disproportionate to the apparent severity of the injury, and — critically — escalating over time. In a patient whose pain should be decreasing as the fracture is stabilized and swelling is managed, any escalation of pain demands immediate reassessment for compartment syndrome. Pain that is unresponsive to normal therapeutic doses of intravenous opioid analgesia is a particularly alarming sign: the pain of ischemia is neurogenic and does not respond to peripheral opioid receptors the way nociceptive fracture pain does. Requesting escalating opioid doses and attributing the ongoing pain to "undertreated fracture pain" is one of the recognized delay patterns in missed compartment syndrome.
Pressure — the compartment feels tense, indurated, "woody," or tight on palpation. In a normal limb, the anterior compartment of the lower leg can be gently compressed between the examiner's thumb and the tibial cortex; in compartment syndrome, the compartment feels like a drum. This physical finding is one of the earliest and most reliable bedside indicators and should be elicited systematically in all patients at risk.
Paresthesias — tingling, pins and needles, or numbness in the distribution of the nerve running through the affected compartment. First web space numbness indicates deep peroneal nerve ischemia (anterior compartment); plantar foot numbness indicates tibial nerve ischemia (deep posterior compartment). These paresthesias represent nerve ischemia — neurons are exquisitely sensitive to oxygen deprivation — and may appear within 30 minutes of critical ischemia onset. They are the earliest reliable neurological sign and must never be dismissed or attributed to "swelling around the fracture." Any new neurological symptom in a traumatized limb should prompt immediate reassessment of compartment pressure.
Paresis — weakness of muscles within the ischemic compartment. By the time muscle weakness is clinically detectable, significant muscle ischemia has already occurred. Testing active dorsiflexion against resistance (anterior compartment), toe extension (anterior compartment), plantarflexion and toe flexion (posterior compartments), and foot eversion (lateral compartment) should be part of the neurovascular examination. Weakness is a late sign relative to paresthesias and pain, but it remains important because it quantifies the degree of ischemic insult and signals urgency.
Pallor — pallor or dusky coloration of the distal extremity occurs when arterial inflow to the foot or hand is compromised. This is a significantly later finding than pain, pressure, or paresthesias. The skin of the foot or hand may look mottled, pale, or gray in comparison to the contralateral limb.
Pulselessness — the absence of palpable dorsalis pedis or posterior tibial pulses is a very late sign that indicates compartment pressure has risen to near or above systemic arterial systolic pressure. By the time pulses disappear, irreversible muscle necrosis has typically been present for one to two hours. A limb with absent pulses and compartment syndrome may already be unsalvageable, or may require not just fasciotomy but also arterial reconstruction. The irreducible clinical lesson is this: do not wait for absent pulses before diagnosing compartment syndrome. The diagnosis must be made earlier, on the basis of escalating pain, a tense compartment, and early neurological changes.
The Critical Importance of Passive Stretch
Among all bedside clinical tests for acute compartment syndrome, pain on passive stretch of the muscles within the suspected compartment is the single most useful maneuver for early detection. It is more sensitive than any of the classical "6 Ps" except spontaneous pain itself, and it is positive earlier in the disease course than paresis or pallor. Every clinician managing traumatic extremity injuries should incorporate this test systematically into their neurovascular examination.
The physiological basis of the test is straightforward: an ischemic, swollen muscle within a tight compartment has exhausted its mechanical reserve. Any further demand placed on it — even passive lengthening without any active muscle contraction — triggers immediate, severe pain because the muscle fibers are already at the edge of ischemic tolerance. This is categorically different from the discomfort of a normal muscle being stretched, which is mild and well tolerated.
Technique for the anterior compartment of the lower leg: with the patient supine and the ankle relaxed, the examiner grasps the foot and passively plantarflexes the ankle (pointing the foot downward). This movement stretches the tibialis anterior and extensor muscles within the anterior compartment. A positive result is excruciating, burning pain in the anterior shin — the patient will often involuntarily withdraw the foot and describe the pain as much worse than the fracture itself. Mild discomfort at the limit of motion is not positive; the response must be clearly disproportionate.
Technique for the deep posterior compartment: the examiner passively dorsiflexes the ankle (toes toward shin) and simultaneously extends the toes. This stretches the flexor hallucis longus, flexor digitorum longus, and tibialis posterior. Severe pain in the deep calf or a burning sensation on the plantar foot constitutes a positive result.
Technique for the forearm volar compartment: the examiner passively extends the fingers at the metacarpophalangeal joints and extends the wrist simultaneously. Severe pain in the volar forearm is a positive result, indicating volar compartment ischemia.
The passive stretch test should be performed early and repeated serially in any patient with a mechanism or clinical picture consistent with developing compartment syndrome. Serial examinations every one to two hours are appropriate in high-risk patients (tibial fracture patients in the first 24 hours post-injury, crush injury patients, reperfusion patients) and any change in the examination findings should prompt immediate formal pressure measurement or surgical consultation. Documenting the result of the passive stretch test (positive or negative, with description) in the medical record is important both for patient safety and for medicolegal accountability.
Compartment Pressure Measurement
When the clinical examination is equivocal, or when the patient cannot provide reliable pain reports due to sedation, intubation, altered mental status, or a regional nerve block, direct measurement of intracompartmental pressure provides an objective threshold for surgical decision-making. Pressure measurement does not replace clinical judgment and should not be used to defer a clinical diagnosis when the examination is clearly positive — but it is an essential adjunct in the scenarios where subjective pain assessment is unreliable.
Technique: the most widely used commercial device is the Stryker Intracompartmental Pressure Monitor System, which uses a syringe, saline-filled tubing, and a pressure transducer attached to a needle inserted directly into the compartment. Alternatively, an arterial line pressure transducer connected to a side-port needle can be used. The needle should be inserted perpendicular to the skin at the level of maximum tenderness or firmness, at the mid-point of the compartment, away from major neurovascular structures. For the four-compartment lower leg, each compartment should be individually measured. Normal compartment pressure is less than 10–15 mmHg.
Absolute pressure threshold: a widely cited absolute threshold for fasciotomy is a compartment pressure greater than 30 mmHg. Some authorities use 20 mmHg in hypotensive patients. However, absolute thresholds are imperfect because they do not account for the patient's own blood pressure.
Delta pressure (ΔP) threshold: the physiologically superior criterion is ΔP = diastolic blood pressure minus compartment pressure. A ΔP less than 30 mmHg is the threshold most strongly supported by clinical evidence and is the criterion recommended by McQueen and Court-Brown based on prospective tibial fracture data (PMID 8898137). Consider the clinical scenario: a trauma patient with a blood pressure of 70/40 mmHg (hypotensive) and a compartment pressure of 20 mmHg has a ΔP of 20 mmHg — critical ischemia despite a compartment pressure that would be acceptable in a normotensive patient. Conversely, a well-hydrated athlete with a blood pressure of 140/90 mmHg and a compartment pressure of 45 mmHg has a ΔP of 45 mmHg — concerning but not immediately critical. Always apply the ΔP criterion in hemodynamically unstable patients.
Continuous monitoring: in obtunded or sedated patients with high-risk tibial fractures (those undergoing intramedullary nailing, who cannot provide pain history), continuous compartment pressure monitoring using an indwelling wick catheter or slit catheter connected to a pressure transducer with an alarm set at ΔP = 30 mmHg is the standard of care at many trauma centers. Any sustained reading below the threshold triggers immediate orthopedic surgical review and, if confirmed, fasciotomy.
Importantly, a single normal pressure reading does not exclude developing compartment syndrome if the clinical picture is evolving. Pressure can rise rapidly over 30–60 minutes following a fracture reduction, cast application, or period of tourniquet ischemia. Any patient with a normal initial reading but continuing clinical deterioration should be re-measured and, if necessary, brought to the operating room without further delay.
Fasciotomy — Surgical Emergency
The only definitive treatment for acute compartment syndrome is immediate surgical fasciotomy — a longitudinal incision through the fascia of each affected compartment, physically releasing the pressure and allowing the trapped contents to decompress. This is a time-critical emergency: the interval between the onset of critical ischemia and irreversible muscle necrosis is approximately 4–8 hours, and the quality of functional recovery is directly proportional to how quickly the decision is made. Every hour of delay worsens outcomes.
Lower leg four-compartment fasciotomy: the standard technique uses two longitudinal skin incisions, each approximately 15–20 cm long. The lateral incision is placed over the fibula and is used to release both the anterior and lateral compartments — the incision is deepened through the fascia of each compartment in turn, and care is taken to identify and protect the superficial peroneal nerve as it exits the lateral compartment distally. The medial incision is placed approximately 2 cm posterior to the medial tibial border and is used to release the superficial and deep posterior compartments — the deep posterior compartment requires additional dissection through the soleus bridge to reach the plane containing the flexor muscles. Healthy compartments release with a visible "herniation" of pink, viable muscle. Pale, dark gray, or friable muscle indicates myonecrosis; necrotic muscle must be debrided at the time of fasciotomy and at subsequent washouts.
Wound management: fasciotomy wounds are left open at the initial procedure. Attempting primary closure under tension defeats the purpose of the decompression and risks re-elevation of compartment pressure. The wound edges are either left exposed (covered with moist dressings, a vacuum-assisted closure sponge, or Xeroform gauze) or bridged with vessel loops or temporary skin closure strips to approximate — but never close under tension — the skin edges. The patient returns to the operating room at 48–72 hours for a planned relook: viable muscle that has decompressed adequately allows either delayed primary closure or, if the wound edges cannot be approximated without tension, a split-thickness skin graft harvested from the thigh.
Forearm fasciotomy: the volar forearm is decompressed through a curvilinear incision that extends from the antecubital fossa, curves across the wrist flexion crease, and continues into the palm to release the carpal tunnel (median nerve decompression). The dorsal forearm is decompressed through a separate straight dorsal incision. Carpal tunnel release is performed routinely because the elevated venous pressure in the forearm transmits distally and the median nerve at the wrist is frequently compromised simultaneously.
Timing and outcomes: fasciotomy performed within 6 hours of the onset of ischemia is associated with near-complete recovery of neuromuscular function in the vast majority of patients. Fasciotomy performed between 6 and 12 hours yields variable outcomes — some patients recover fully, others are left with residual neurological deficit or partial muscle weakness. Fasciotomy performed after 12 hours carries a substantially higher rate of permanent motor deficit, chronic pain, and contracture. Fasciotomy after 24–36 hours in a limb with established extensive myonecrosis may be contraindicated because decompressing necrotic muscle provides no functional benefit but releases massive amounts of myoglobin and inflammatory mediators systemically, potentially precipitating acute kidney injury and sepsis — in these cases, primary amputation may be the safer option.
Complications of fasciotomy itself: include wound infection, the need for skin grafting (with associated donor-site morbidity), wound dehiscence, scar formation, superficial peroneal nerve injury during lateral incision, and the cosmetic and functional burden of a large lower leg scar. These complications are real but uniformly acceptable compared to the alternative of untreated compartment syndrome.
Chronic Exertional Compartment Syndrome
Chronic exertional compartment syndrome (CECS) is a fundamentally different condition from acute compartment syndrome — it shares only the name and the underlying mechanism of a tight fascial compartment. CECS is not a surgical emergency, does not cause permanent tissue damage, and presents an entirely different clinical picture. Conflating the two can cause both under-treatment of acute compartment syndrome and over-treatment of CECS.
CECS most commonly affects young, athletic individuals — runners and cyclists predominate, though it is seen in any sport involving repetitive lower leg loading. The anterior compartment of the lower leg is involved in the majority of cases; the deep posterior and lateral compartments are less commonly affected. The condition is bilateral in approximately 75–95% of cases, which is an important diagnostic clue.
Mechanism: during intense sustained exercise, muscle volume increases by approximately 20% due to vasodilation, capillary recruitment, and local edema of exercise. In most individuals, the fascia accommodates this volume increase without significant pressure rise. In patients with CECS, the fascia is relatively inelastic — whether due to congenital anatomy, repetitive training-induced fascial thickening, or simply variation in tissue compliance — and pressure rises to ischemic levels during exercise. No permanent injury occurs because the increased pressure is transient, resolving completely as exercise stops and muscle volume normalizes.
Clinical features: the hallmark of CECS is its reproducibility and its relief with rest. Patients describe a pressure, aching, or burning sensation in the anterior shin (or less commonly, the lateral leg or deep posterior calf) that begins after a consistent duration of exercise — "always starts about 15 minutes into my run." The pain escalates with continued activity, becomes severe enough to cause the patient to stop or significantly slow, and then resolves completely within 20–30 minutes of rest. There are no neurological symptoms at rest; mild tingling in the first web space (deep peroneal nerve) or dorsal foot (superficial peroneal) may occur during symptomatic exercise. Between episodes, the examination is entirely normal — there is no tenderness, no tense compartment, no weakness.
Diagnosis: the diagnosis is confirmed with compartment pressure measurement performed before and after a standardized provocative exercise protocol (typically running on a treadmill until symptoms reproduce). Diagnostic criteria (Pedowitz et al., 1990, PMID 2313528) include: resting pressure ≥15 mmHg, one-minute post-exercise pressure ≥30 mmHg, or five-minute post-exercise pressure ≥20 mmHg. The diagnosis requires both reproducible symptoms and abnormal pressures — isolated pressure elevation without symptoms (or symptoms without abnormal pressures) is not diagnostic.
Treatment: initial management includes activity modification, stretching, gait retraining, and a trial period of reduced training volume. Running gait modifications (increasing step rate, reducing step length) have shown promise in reducing anterior compartment pressure during running. Orthotic intervention and footwear modification may help in some patients. For athletes who require full return to competitive sport without activity restriction, elective fasciotomy is the definitive treatment. Unlike emergency fasciotomy, this is planned outpatient surgery through small incisions with primary closure — recovery allows return to full sport in 6–12 weeks in most cases. Outcomes are excellent: more than 80% of athletes return to full sport after fasciotomy for CECS.
CECS must be differentiated from other exercise-induced leg pain syndromes including medial tibial stress syndrome (shin splints), stress fractures, popliteal artery entrapment syndrome, and peripheral neuropathy. The reproducible onset-with-exercise and complete relief-with-rest pattern is the most reliable clinical discriminator.
Complications of Missed or Delayed Diagnosis
Volkmann's Ischemic Contracture — the eponymous complication of missed forearm compartment syndrome, first described by Richard von Volkmann in 1881. Progressive fibrosis and scarring of ischemic flexor muscle bellies produce a fixed flexion deformity of the fingers, wrist, and sometimes elbow that cannot be overcome by patient effort. In mild cases (Tsuge Grade I), only the finger flexors are involved and the deformity is mild and correctable with splinting and physiotherapy. In moderate cases (Grade II), the median nerve is involved, producing a combined motor-sensory deficit with intrinsic muscle wasting and clawing. In severe cases (Grade III), all flexors, extensors, and intrinsic muscles of the hand are involved, producing a globally dysfunctional limb. Reconstruction requires tendon-lengthening procedures, muscle slide operations, neurolysis, or — in severe cases — free functional muscle transfer from the gracilis or latissimus dorsi. The results of reconstruction are always inferior to what would have been achieved by timely fasciotomy.
Foot Drop — irreversible injury to the deep peroneal nerve and the anterior compartment muscles from untreated acute anterior compartment syndrome of the lower leg. The patient is permanently unable to dorsiflex the foot and loses the ability to clear the foot during the swing phase of walking, producing the characteristic high-stepping "steppage gait." The sensory deficit involves the first web space. Functional management requires a custom ankle-foot orthosis (AFO) for the rest of the patient's life. In selected cases, tendon transfer surgery — transferring the tibialis posterior tendon through the interosseous membrane to the dorsum of the foot — can partially restore active dorsiflexion, though the outcome is never equivalent to an intact anterior compartment.
Rhabdomyolysis and Acute Kidney Injury — massive muscle necrosis from any cause releases large quantities of myoglobin, creatine kinase, and other intracellular contents into the circulation. Myoglobin is directly nephrotoxic — it precipitates in renal tubules, particularly in the setting of aciduria and dehydration, causing myoglobinuric acute tubular necrosis. Serum creatine kinase levels in severe rhabdomyolysis can exceed 100,000 IU/L (normal <200). Initial urine is classically "tea-colored" or "cola-colored." Treatment requires aggressive intravenous fluid resuscitation (targeting urine output 200–300 mL/hour) to flush the tubules. Urinary alkalinization with sodium bicarbonate (to keep urine pH >6.5 and prevent myoglobin precipitation) and mannitol (to maintain tubular flow) are used at some centers. Persistent oliguria despite adequate resuscitation requires hemodialysis. Multi-organ failure can supervene in severe cases.
Infection and Gas Gangrene — necrotic muscle in a delayed-treatment compartment syndrome is a culture medium for anaerobic bacteria, particularly Clostridium species. Gas gangrene (clostridial myonecrosis) is a rapidly fatal infection characterized by crepitus on palpation (gas in tissues), spreading erythema with bullae, systemic toxicity out of proportion to the local wound, and a distinctive "dishwater" wound exudate. Surgical debridement, amputation, and high-dose penicillin are required immediately. Prevention is the only reliable strategy — prompt fasciotomy eliminates the necrotic muscle substrate.
Amputation — the ultimate consequence of severe, missed, or untreatable compartment syndrome. Amputation may be required acutely for gas gangrene or when the limb is clearly unsalvageable, or may be required late for a chronically painful, nonfunctional, infected contractured limb. Below-knee amputation with a well-fitted prosthesis typically provides better functional outcomes than a salvaged limb with severe Volkmann's contracture, permanent foot drop, chronic osteomyelitis, and neuropathic pain.
Medicolegal consequences — missed or delayed diagnosis of acute compartment syndrome is one of the most litigated clinical events in orthopedic and emergency medicine malpractice cases. The elements of negligence are typically straightforward: there was a duty of care, the presentation was clinically recognizable, a timely examination would have revealed diagnostic signs, fasciotomy would have prevented the harm, and permanent disability resulted from the delay. Documentation of serial neurovascular examinations — including the passive stretch test, compartment firmness, and distal sensory findings — is both good clinical practice and essential medicolegal protection.
Key Research Papers
- Mubarak SJ, et al. Acute compartment syndromes. Surg Gynecol Obstet. 1978;147(6):943–9. — Search PubMed — Foundational description of the pathophysiology, diagnosis, and surgical management of acute compartment syndrome; established the pressure-measurement framework still in use today.
- McQueen MM, Court-Brown CM. Compartment monitoring in tibial fractures. J Bone Joint Surg Br. 1996;78(1):99–104. PMID: 8898137 — Prospective study establishing the delta pressure (ΔP <30 mmHg) criterion as the most reliable threshold for fasciotomy, reducing unnecessary surgery while preventing ischemic damage.
- Whitesides TE, et al. Tissue pressure measurements as a determinant for the need of fasciotomy. Clin Orthop Relat Res. 1975;113:43–51. PMID: 1192678 — Early paper introducing the concept of comparing compartment pressure to diastolic blood pressure to determine fasciotomy need.
- Boody AR, Wongworawat MD. Accuracy in the measurement of compartment pressures. J Bone Joint Surg Am. 2005;87(11):2415–22. — Search PubMed — Comparative evaluation of different pressure measurement devices (Stryker, arterial line, mercury manometer), demonstrating differences in accuracy and technique-dependence.
- Perron AD, et al. Orthopedic pitfalls in the ED: acute compartment syndrome. Am J Emerg Med. 2002;20(1):36–8. — Search PubMed — Emergency medicine perspective on the common diagnostic pitfalls, including over-reliance on absent pulses and pain managed with opioids masking the diagnosis.
- Elliott KG, Johnstone AJ. Diagnosing acute compartment syndrome. J Bone Joint Surg Br. 2003;85(5):625–32. — Search PubMed — Systematic review of the sensitivity and specificity of the clinical signs; demonstrates that pain on passive stretch is the most sensitive early clinical sign.
- Ulmer T. The clinical diagnosis of compartment syndrome of the lower leg: are clinical findings predictive of the disorder? J Orthop Trauma. 2002;16(8):572–7. — Search PubMed — Systematic review finding that pain out of proportion and pain on passive stretch have the highest likelihood ratios for predicting compartment syndrome; absent pulses have poor diagnostic utility.
- Rorabeck CH, Macnab I. The pathophysiology of the anterior tibial compartment syndrome. Clin Orthop Relat Res. 1975;113:52–7. — Search PubMed — Experimental and clinical description of the anterior tibial compartment, delineating the relationship between pressure, arterial flow, and tissue viability.
- Court-Brown CM, et al. Tibial shaft fractures complicated by compartment syndrome. J Bone Joint Surg Br. 1992;74(4):600–4. — Search PubMed — Large series demonstrating that open tibial fractures carry comparable compartment syndrome risk to closed fractures, countering the false reassurance of an open wound.
- Pedowitz RA, et al. Modified criteria for the objective diagnosis of chronic compartment syndrome of the leg. Am J Sports Med. 1990;18(1):35–40. — Search PubMed — Established the widely used pressure thresholds (pre-exercise ≥15 mmHg, 1-min post ≥30 mmHg, 5-min post ≥20 mmHg) for diagnosing chronic exertional compartment syndrome.
- Matsen FA 3rd. Compartmental syndrome. An unified concept. Clin Orthop Relat Res. 1975;113:8–14. — Search PubMed — A landmark conceptual paper unifying the pathophysiology of compartment syndrome across different anatomical locations and causes.
- Sheridan GW, Matsen FA 3rd. Fasciotomy in the treatment of the acute compartment syndrome. J Bone Joint Surg Am. 1976;58(1):112–6. — Search PubMed — Clinical series demonstrating that early fasciotomy prevents Volkmann's ischemic contracture and that delay correlates directly with worse outcomes.
PubMed Research Searches
- Acute compartment syndrome fasciotomy timing
- Compartment syndrome tibial fracture diagnosis
- Chronic exertional compartment syndrome runners
- Compartment pressure measurement delta pressure fasciotomy
Connections
- Orthopedics
- Stress Fracture
- Hip Fracture
- Osteonecrosis
- Osteomyelitis
- Rhabdomyolysis
- Acute Kidney Injury
- Creatine Kinase
- Septic Arthritis