Nystagmus
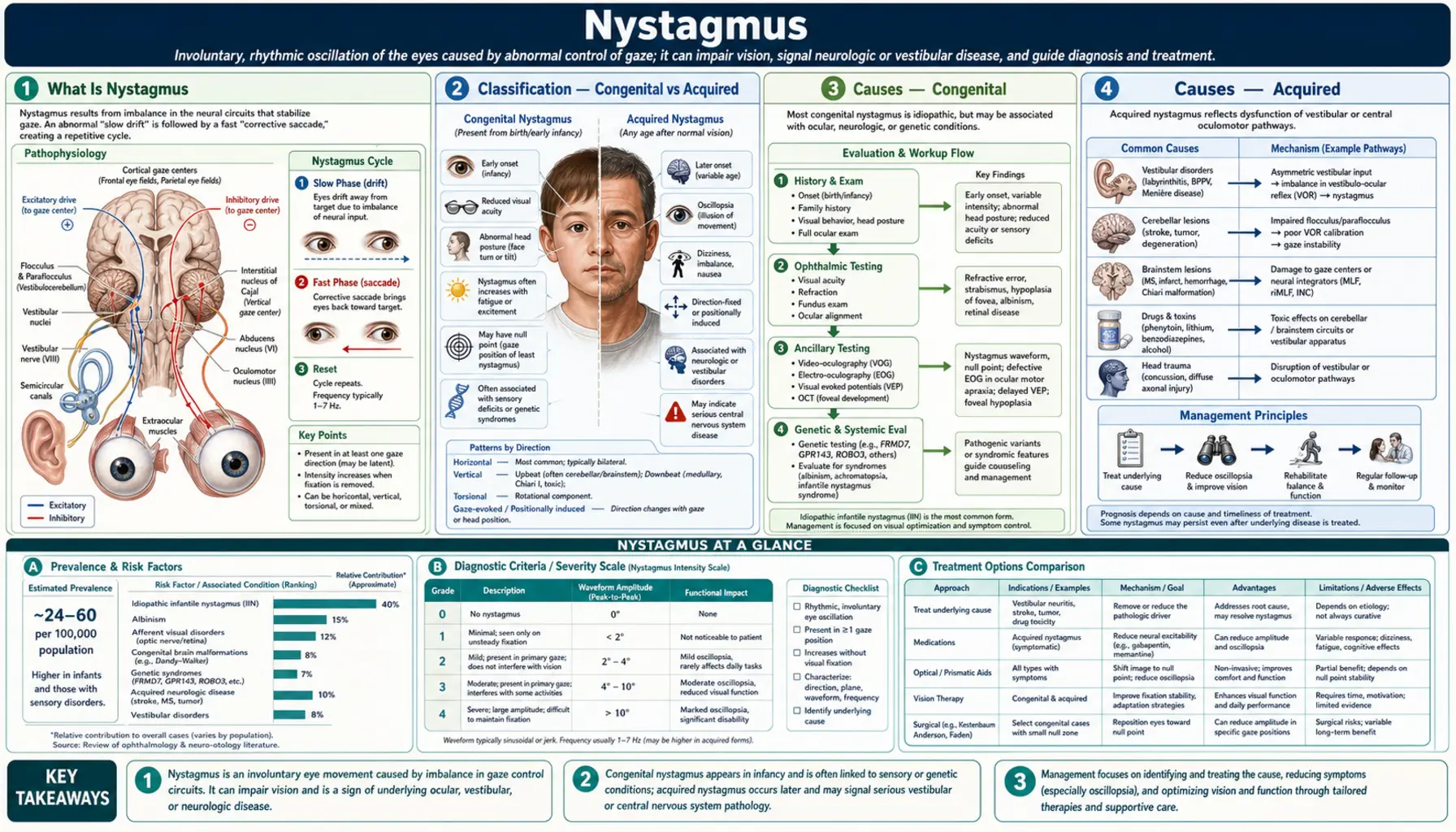
Nystagmus is a condition in which the eyes make involuntary, rhythmic, repetitive movements that the person cannot control. The eyes may drift slowly in one direction and then snap back, or they may oscillate back and forth like a pendulum, and this happens continuously — it does not stop when the person concentrates or tries harder to hold their eyes still. These movements interfere with the ability to keep objects in stable focus, and they affect an estimated 1 in 1,000 people worldwide, making nystagmus one of the more common conditions seen in pediatric eye clinics.
The condition comes in two broad forms. Congenital or infantile nystagmus appears in the first few months of life, often alongside conditions that reduce visual input early in development — such as albinism, early cataracts, or retinal disorders — though many cases are idiopathic, meaning no structural cause is ever found. Children with congenital nystagmus adapt remarkably well: their brains suppress the perception that the world is moving, and many grow up, attend mainstream schools, hold jobs, and lead entirely normal lives, even though their visual acuity is often reduced. Vision aids, corrective lenses, and in some cases surgery can bring meaningful improvements.
Acquired nystagmus — nystagmus that develops later in life in someone whose visual system was previously stable — is a different matter entirely. It almost always signals an underlying neurological, metabolic, or toxic process: multiple sclerosis, a stroke or tumor in the brainstem or cerebellum, thiamine deficiency, medication toxicity, or an inner ear disorder, among others. The hallmark symptom of acquired nystagmus is oscillopsia — the terrifying sensation that the world is constantly shimmering or bouncing — which is absent in congenital cases because the brain never learned to expect a stable world. Any adult who develops new, unexplained eye oscillation requires urgent neurological evaluation and brain imaging.
- What Is Nystagmus
- Classification — Congenital vs Acquired
- Causes — Congenital
- Causes — Acquired
- Symptoms and Impact
- Evaluation and Diagnosis
- Treatment — Optical and Pharmacological
- Treatment — Surgical and Botulinum Toxin
- Key Research Papers
- Connections
What Is Nystagmus
The word nystagmus comes from the Greek nystagmos, meaning "to nod" or "to be drowsy and nodding" — a reference to the bobbing quality that observers noticed in the eyes of affected individuals. In clinical terms, nystagmus is defined as an involuntary, rhythmic, repetitive oscillation of one or both eyes. The oscillations can occur in any plane:
- Horizontal nystagmus — the eyes move left and right; by far the most common direction in both congenital and most acquired forms
- Vertical nystagmus — the eyes move up and down; almost always a sign of brainstem or cerebellar pathology when it is the dominant direction
- Torsional (rotary) nystagmus — the eyes rotate clockwise and counterclockwise around the line of sight; common in brainstem strokes and BPPV
- Mixed nystagmus — components in more than one plane simultaneously
Nystagmus also comes in two fundamental waveform types that tell clinicians a great deal about where in the nervous system the problem originates:
- Jerk nystagmus — the most common type; characterized by a slow drift of the eye in one direction followed by a fast corrective saccade (jump) back. The nystagmus is named by the direction of the fast phase — so "right-beating" nystagmus means the fast phase goes to the right, even though the eye is drifting leftward. Jerk nystagmus is typical of vestibular disease, cerebellar disorders, and brainstem lesions.
- Pendular nystagmus — the eye oscillates back and forth with approximately equal velocity in both directions, like a pendulum on a clock. There is no fast-and-slow distinction. Pendular nystagmus is common in congenital nystagmus and in acquired forms associated with demyelinating disease.
Three other parameters describe nystagmus intensity: amplitude (how far the eye travels with each oscillation, typically measured in degrees), frequency (how many full cycles occur per second; most nystagmus falls between 1 and 6 Hz), and whether the movements are conjugate (both eyes moving together in the same direction by the same amount) or disconjugate (one eye moving more than the other, or moving in a different direction — an important sign of certain brainstem disorders such as internuclear ophthalmoplegia).
The functional consequences of nystagmus depend heavily on whether it is congenital or acquired, and on the presence or absence of a stable null zone — a position of gaze (often off-center, requiring a compensatory head turn) where the nystagmus quiets down and visual acuity improves. Many patients with infantile nystagmus develop a head posture to exploit their null zone, which can cause neck strain over decades but meaningfully improves their usable vision.
Classification — Congenital vs Acquired
The single most important clinical distinction in nystagmus is whether onset occurred before or after the visual system completed its early development — broadly, before or after six months of age. This divides nystagmus into two categories with different causes, different prognoses, and different management approaches.
Infantile (Congenital) Nystagmus Syndrome (INS)
Formerly called "congenital motor nystagmus," the preferred modern term is Infantile Nystagmus Syndrome. It is defined by onset within the first six months of life. Key characteristics:
- Direction is almost always horizontal, even on vertical gaze — a feature that helps distinguish it from acquired nystagmus
- Movements are conjugate (both eyes move together)
- Intensity dampens with convergence — the eyes tend to quiet when the patient focuses on something close-up, which is why many patients with INS read better at near distance than in the distance
- Absent during sleep — the nystagmus disappears the moment the patient falls asleep, a distinguishing feature from voluntary eye oscillation
- A null zone is usually present — a gaze direction or head position where the nystagmus is least intense and visual acuity is best; patients develop characteristic head postures to exploit this
- May be idiopathic (no underlying structural cause found, often genetic — mutations in the FRMD7 gene on the X chromosome) or associated with afferent pathway disease that reduces early visual input
Sensory Nystagmus
When a condition that impairs visual input is present from birth or early infancy, the ocular motor system lacks the visual feedback it needs to calibrate stable fixation. The result is sensory nystagmus — the eyes drift because the brain cannot hold them still without clear visual input. The most common causes are albinism, congenital cataracts, optic nerve hypoplasia, and retinal dystrophies. Sensory nystagmus overlaps with INS in presentation.
Latent and Manifest Latent Nystagmus
This form is specifically associated with strabismus and amblyopia. Latent nystagmus is absent when both eyes are open but appears (or worsens markedly) when one eye is covered. The jerk direction is always toward the uncovered (viewing) eye. Manifest latent nystagmus is present even with both eyes open but worsens with monocular occlusion. Both forms are important because monocular visual acuity testing — standard in optometry offices — can artificially worsen results by inducing latent nystagmus; accurate testing requires special techniques.
Spasmus Nutans
A triad of head nodding + head tilt + nystagmus appearing in infants between 6 and 18 months and typically resolving by age 3. The nystagmus in spasmus nutans is often asymmetric or even monocular, fine amplitude, and high frequency. While usually benign and self-resolving, the presentation is identical to that of a diencephalic (midbrain) glioma, and neuroimaging is mandatory in all cases to exclude tumor before watchful waiting is adopted.
Acquired Nystagmus
Any nystagmus that develops after the visual system has matured — generally after age 6 months and certainly in adulthood — is acquired nystagmus. Unlike the congenital forms, acquired nystagmus almost always indicates an identifiable neurological, toxic, or systemic disease. The brain adapted to stable eyes early in life and now experiences the oscillations as pathological disruption. The workup is therefore fundamentally different: brain imaging, vestibular testing, medication review, and metabolic screening are standard initial steps.
Causes — Congenital
Idiopathic Infantile Nystagmus Syndrome
The most common form of congenital nystagmus has no identifiable structural cause in the eyes or brain. The retina looks normal, the optic nerve is healthy, and imaging is unremarkable. In many families, nystagmus passes through generations in an X-linked pattern linked to mutations in the FRMD7 gene (FERM domain-containing protein 7), which is expressed during development of the ocular motor system. Males are more severely affected; female carriers may have mild nystagmus or none at all. Onset is within the first few months of life, and the nystagmus is horizontal, conjugate, and usually pendular or jerk. Visual acuity ranges from near-normal to significantly reduced but rarely drops below 20/200.
Albinism
Albinism is one of the most common identifiable causes of congenital nystagmus. It comes in two forms:
- Oculocutaneous albinism (OCA1–4) — autosomal recessive; reduced or absent melanin in skin, hair, and eyes; the most severe form (OCA1A) has complete absence of melanin
- Ocular albinism (OA1) — X-linked; melanin reduction confined to the eyes; skin and hair appear normal, making the diagnosis easy to miss without targeted examination
In albinism, the fovea — the central retinal zone responsible for sharp, detailed vision — fails to develop properly (foveal hypoplasia). On optical coherence tomography (OCT) imaging, the normal foveal pit is absent, and the inner retinal layers abnormally cross into the foveal zone. Additionally, the optic nerve fibers that normally remain uncrossed (serving ipsilateral cortex) instead cross at the chiasm, resulting in abnormal routing of visual signals to the brain. This abnormal chiasmal decussation can be detected on visual evoked potential (VEP) testing — it produces a characteristic asymmetric waveform that is diagnostic for albinism even without skin or hair changes. Visual acuity in albinism typically ranges from 20/60 to 20/400.
Early-Onset Cataracts
The visual system requires clear retinal images during a critical developmental window — roughly the first 8 to 10 weeks of life — to establish normal ocular motor control. Congenital cataracts that are not surgically treated before this window closes deprive the developing brain of visual input, leading to form deprivation nystagmus. This is one reason pediatric ophthalmologists treat dense congenital cataracts as an urgent matter. Surgery before 6 to 8 weeks of age, followed immediately by refractive correction and amblyopia patching, gives the best chance of avoiding nystagmus or minimizing its severity.
Optic Nerve Hypoplasia
Optic nerve hypoplasia (ONH) is now the most common cause of permanent visual impairment in children in developed countries. The optic disc is abnormally small, with a reduced number of axons. When ONH is bilateral and severe, nystagmus develops from reduced visual input. ONH is associated with septo-optic dysplasia (de Morsier syndrome) — a triad of ONH, absence of the septum pellucidum on brain MRI, and pituitary insufficiency (growth hormone deficiency, hypothyroidism, or diabetes insipidus). All children diagnosed with ONH require a brain MRI and endocrine evaluation. Risk factors include young maternal age, first pregnancy, maternal diabetes, and prenatal valproate exposure.
Retinal Dystrophies
Leber congenital amaurosis (LCA) is the most severe early-onset retinal dystrophy. Affected children have profound vision loss from birth, roving nystagmus, and may press on their eyes (oculodigital reflex). The electroretinogram (ERG) is flat or nearly flat, confirming retinal non-function. LCA is caused by mutations in any of more than 20 genes, including RPE65 and CEP290. Voretigene neparvovec (Luxturna), a gene therapy that delivers a functional copy of the RPE65 gene directly into retinal cells, was FDA-approved in 2017 — the first FDA-approved gene therapy for an inherited retinal disease — and can meaningfully restore usable vision in eligible patients. Other retinal dystrophies (achromatopsia, congenital stationary night blindness) also cause nystagmus through the same afferent deprivation mechanism.
Causes — Acquired
Demyelinating Disease
Multiple sclerosis (MS) is the most common cause of acquired nystagmus in young adults. MS attacks the myelin sheaths of axons throughout the central nervous system, and the brainstem and cerebellum are particularly vulnerable. Several distinct nystagmus patterns are associated with MS:
- Internuclear ophthalmoplegia (INO) — demyelination of the medial longitudinal fasciculus (MLF) disconnects the nerve signals that coordinate horizontal gaze. The result: the adducting eye (the eye turning inward) moves slowly and incompletely, while the abducting eye (turning outward) develops nystagmus in compensation. Bilateral INO in a young person is MS until proven otherwise.
- Pendular nystagmus — acquired pendular nystagmus with oscillopsia is particularly common in advanced MS and arises from cerebellar and brainstem circuit disruption
- Gaze-evoked nystagmus — direction-changing horizontal nystagmus that appears when the eyes look to either side, from cerebellar pathway involvement
Cerebellar Disease
The cerebellum is the primary calibrator of smooth, accurate eye movements — it fine-tunes gaze holding so the eyes stay where you point them. When the cerebellum is damaged, the eyes drift off target and jerk back repeatedly: gaze-evoked nystagmus. Key cerebellar nystagmus patterns include:
- Gaze-evoked nystagmus — direction-changing, with fast phase always toward the direction of gaze; the most sensitive sign of cerebellar pathway dysfunction
- Downbeat nystagmus — the eyes beat downward in primary (straight-ahead) gaze. This is a localizing sign pointing to the flocculus/paraflocculus of the cerebellum or the craniocervical junction. Causes include Chiari malformation (cerebellar tonsil herniation through the foramen magnum), cerebellar degeneration, lithium toxicity, anticonvulsants, and magnesium deficiency. A Chiari malformation must be excluded by brain and cervical spine MRI in every patient with new downbeat nystagmus.
- Upbeat nystagmus — beats upward; associated with brainstem lesions, Wernicke's encephalopathy, and anti-epileptic drugs
- Periodic alternating nystagmus (PAN) — the nystagmus beats in one horizontal direction for approximately 90 seconds, then quiets briefly, then reverses direction for another 90 seconds, cycling continuously. PAN is a specific cerebellar sign; it responds dramatically to baclofen.
Brainstem Lesions
Strokes or tumors in the brainstem produce nystagmus patterns that help localize the lesion. Wallenberg syndrome (posterior inferior cerebellar artery — PICA — infarction) produces a characteristic cluster: torsional nystagmus toward the side of the lesion, ipsilateral facial numbness, contralateral body numbness, ipsilateral Horner syndrome (drooping eyelid + small pupil), dysphagia, and hoarseness. The torsional nystagmus in Wallenberg syndrome is diagnostic when combined with the other features.
Vestibular Disorders
The vestibular system — the inner ear balance apparatus and its central connections — normally generates a corrective eye movement that keeps vision stable during head movement. When the vestibular system is disrupted, the eyes drift toward the damaged side and the brain corrects with a fast saccade away, producing vestibular nystagmus. Key forms:
- Benign paroxysmal positional vertigo (BPPV) — the most common vestibular disorder; caused by displaced calcium carbonate crystals in the semicircular canals; triggered by position change; produces a characteristic horizontal-torsional nystagmus with a latency of several seconds, lasting less than 60 seconds, and fatiguing with repeated testing. The Epley canalith repositioning maneuver resolves BPPV in most patients in a single office visit.
- Acute vestibular neuritis — sudden unidirectional horizontal-torsional nystagmus with severe vertigo; nystagmus is suppressed when the patient fixates on a target (fixation suppression test) — this is a key feature that distinguishes peripheral from central vestibular disease. Central causes (stroke) do not suppress with fixation.
- Méniére's disease — episodic nystagmus with vertigo, tinnitus, and fluctuating hearing loss
Drugs and Toxins
Multiple medications reliably produce nystagmus, usually gaze-evoked, as a dose-dependent effect:
- Anticonvulsants — phenytoin, carbamazepine, and lamotrigine all cause horizontal gaze-evoked nystagmus at elevated plasma levels; serum drug levels should be checked in any patient on these medications who develops new nystagmus
- Alcohol — acute intoxication causes horizontal gaze-evoked nystagmus (positional alcohol nystagmus); heavy chronic use causes Wernicke's encephalopathy (see below)
- Wernicke's encephalopathy — thiamine (vitamin B1) deficiency, almost always from alcoholism, malnutrition, or prolonged vomiting; produces a classic triad of nystagmus (both vertical and horizontal), ataxia, and confusion; nystagmus in Wernicke's often has both horizontal and vertical components, which helps distinguish it from simple alcohol intoxication. Treatment with IV thiamine is urgent — delay risks permanent Korsakoff syndrome.
- Lithium — both acute toxicity and chronic use can produce downbeat nystagmus
- Barbiturates and benzodiazepines — produce gaze-evoked nystagmus at toxic doses
- Aminoglycosides (gentamicin, tobramycin) — vestibulotoxic; can cause permanent vestibular damage with associated nystagmus
Symptoms and Impact
Oscillopsia
Oscillopsia is the illusion that the visual world is constantly moving, oscillating, or shimmering. It is the most disabling symptom of acquired nystagmus and can be profoundly disorienting — patients describe it as trying to read while someone is shaking the page, or feeling perpetually motion-sick. Crucially, oscillopsia is absent in congenital nystagmus. Because children with infantile nystagmus never experienced stable vision, the brain adapts during development to suppress the perception of image motion. This cortical suppression is one reason many people with congenital nystagmus are surprised to learn their eyes are moving — they do not feel it. Patients with acquired nystagmus lose this suppression because their brain learned to expect stillness; they feel every oscillation.
Reduced Visual Acuity
In congenital nystagmus, visual acuity is reduced because the moving eye cannot hold a stable retinal image of a target long enough for the fovea to process sharp detail. Acuity typically ranges from 20/30 (mild) to 20/200 (moderate-severe), depending on the underlying cause and the presence of structural problems such as foveal hypoplasia in albinism. The null zone is the patient's best friend: at the head position where nystagmus quiets, acuity can improve by several lines on a vision chart. Paradoxically, many patients with congenital nystagmus read at near without difficulty, because convergence damps the nystagmus.
Abnormal Head Postures
To exploit their null zone, many patients with congenital nystagmus adopt a characteristic head posture — a face turn to the left or right, a chin-up or chin-down tilt, or a head tilt to one shoulder. These compensatory postures are effective for improving vision but impose a lifetime of asymmetric strain on the cervical spine and can cause chronic neck pain. They are also cosmetically noticeable and can draw unwanted attention. Surgical treatment (the Kestenbaum-Anderson procedure) can shift the null zone to the straight-ahead position, eliminating or reducing the abnormal head posture. Botulinum toxin to the sternocleidomastoid muscle is an alternative for patients who are not surgical candidates.
Reading and Academic Impact
Scanning a line of text requires precise, rapid eye movements. When the eyes are oscillating continuously, the ability to scan text smoothly is compromised, leading to slower reading speeds, increased reading effort, and fatigue with sustained visual tasks. Children with nystagmus frequently need extended time allowances on exams, preferential seating, and larger print. Tinted lenses improve contrast sensitivity in some patients, which can make reading easier. As adults, many patients find that computer screens at close range are easier to use than printed text at distance.
Social and Psychological Impact
The visible movement of the eyes is noticed by others, and children with nystagmus frequently report bullying, unwanted questions, and social self-consciousness. Adults describe the same awareness in job interviews and social interactions. A UK survey of adults with nystagmus found that most felt their condition had limited their career choices and that they had experienced discrimination. Psychological support and connecting with nystagmus support organizations (such as Nystagmus Network in the UK or the American Nystagmus Network) can be meaningfully beneficial alongside medical management.
Driving
Most patients with congenital nystagmus cannot meet visual acuity standards for unrestricted driving — in most countries, legal driving requires at least 20/40 vision in the better eye, which many nystagmus patients cannot achieve. Acquired nystagmus almost universally prevents driving until the underlying condition is treated and the nystagmus resolves or significantly improves. Low-vision specialists and occupational therapists can help patients find alternative transportation solutions and maximize independence.
Evaluation and Diagnosis
History
The clinical history begins with a precise chronology. The most critical question is when did the nystagmus appear? Onset before 6 months suggests infantile nystagmus; onset after visual maturity requires a neurological explanation. The clinician will ask about:
- Family history — X-linked FRMD7 mutations, albinism, or retinal dystrophies
- Associated symptoms — vertigo, hearing loss, diplopia (double vision), oscillopsia, headache, balance problems, limb weakness or incoordination, speech difficulty, or swallowing problems. Any of these alongside new nystagmus are red flags pointing to brainstem or cerebellar disease.
- Medications — a complete list, with particular attention to anticonvulsants, lithium, and sedatives
- Alcohol and toxin exposure
- Head posture — a habitual head turn or tilt, present from infancy, strongly suggests a congenital null zone
Eye Movement Examination
A detailed eye movement examination records the nystagmus direction, amplitude, and frequency in all positions of gaze, including up, down, left, right, and diagonals. The examiner notes whether nystagmus changes direction between gaze positions (direction-changing nystagmus suggests cerebellar disease), whether it is suppressed by fixation (peripheral vestibular) or not (central), and whether it changes with convergence (dampening with convergence is a feature of INS). Video-oculography — recording eye movements with infrared cameras — provides an objective, quantitative record of amplitude, frequency, and waveform that is invaluable for documenting baseline severity and tracking treatment response.
Ophthalmologic Examination
A complete dilated fundus examination assesses the optic nerve (for hypoplasia), foveal reflex (absent in albinism), and retina (for dystrophic changes). Optical coherence tomography (OCT) of the macula is particularly useful in suspected albinism: foveal hypoplasia produces a characteristic OCT appearance — absence of the normal foveal pit depression, abnormal thickening of the foveal zone, and crossing of inner retinal ganglion cell layers across the foveal center. This is a sensitive diagnostic marker that can confirm albinism even in individuals with subtle skin and hair pigmentation.
Electrodiagnostic Testing
- Electroretinogram (ERG) — measures the electrical response of the retina to light flashes; a flat or severely attenuated ERG in a child with nystagmus points to a primary retinal dystrophy (LCA, achromatopsia, congenital stationary night blindness)
- Visual evoked potential (VEP) — measures the brain's electrical response to visual stimulation; the key finding in albinism is an asymmetric response between hemispheres from the abnormally crossed optic fibers — the hemisphere ipsilateral to the stimulated eye receives a stronger signal than normal, because more fibers crossed the chiasm than should have. This VEP pattern is diagnostic for albinism.
Neuroimaging
MRI of the brain and posterior fossa is mandatory for all acquired nystagmus and for any congenital nystagmus where a structural cause is suspected (vertical nystagmus, asymmetric nystagmus, spasmus nutans pattern, or associated neurological signs). Key findings to look for include MS plaques in the brainstem and periventricular white matter, Chiari malformation at the craniocervical junction, posterior fossa tumors, cerebellar atrophy, and the characteristic thalamic and mammillary body signal changes of Wernicke's encephalopathy. Gadolinium contrast is added when demyelinating disease or tumor is in the differential.
Genetic Testing
Next-generation sequencing panels are now available and clinically useful in pediatric nystagmus. Testing can identify FRMD7 mutations (X-linked INS), oculocutaneous albinism genes (OCA1–4), and a broad array of retinal dystrophy genes (LCA panel, retinal dystrophy panel). A positive genetic result confirms the diagnosis, enables accurate counseling about inheritance, identifies other family members at risk, and — in the case of RPE65 or CEP290-related LCA — opens the door to gene therapy eligibility.
Treatment — Optical and Pharmacological
Accurate Refractive Correction
The first and most universally applicable treatment for nystagmus is ensuring that the patient's refractive error — nearsightedness, farsightedness, or astigmatism — is fully and accurately corrected. Better retinal image quality provides stronger visual feedback to the ocular motor system, which reduces nystagmus intensity. In children, this also means maximizing visual input during the critical period to support the best possible visual development. Full correction, not under-correction, is the standard.
Contact Lenses
Several studies have found that rigid gas-permeable or soft contact lenses reduce nystagmus intensity compared with spectacles in patients with congenital nystagmus, with improvements in visual acuity of up to 2 lines on the Snellen chart. The mechanism is debated — one hypothesis is that the tactile stimulation of the lens on the ocular surface provides somatosensory feedback that helps stabilize the eye through a proprioceptive mechanism. Contact lenses are a reasonable option for patients with INS who cannot achieve adequate acuity with glasses alone, and a trial is worthwhile in motivated patients.
Prism Glasses
Base-out prisms induce convergence — and because many patients with INS have their nystagmus dampened by convergence, prisms can reduce nystagmus intensity and improve acuity by essentially tricking the eyes into a convergent posture. Separately, prisms can also shift the visual image in the direction of the null zone, allowing the patient to view objects through their best-acuity gaze position without adopting an abnormal head turn. Neither approach eliminates nystagmus, but both can provide meaningful functional improvement without surgery.
Gabapentin
Gabapentin (300 to 1,200 mg per day, in divided doses) has the strongest evidence base among pharmacological treatments for nystagmus. It is most effective for acquired pendular nystagmus — particularly the type seen in multiple sclerosis — where it reduces both nystagmus amplitude and oscillopsia severity. A randomized controlled trial by Averbuch-Heller and colleagues demonstrated statistically significant benefit versus placebo. The drug acts on voltage-gated calcium channels and likely stabilizes aberrant brainstem oscillations. Side effects — sedation, dizziness, and gait unsteadiness — are dose-dependent and may limit tolerability in patients who already have balance problems from their underlying disease.
Memantine
Memantine (100 to 300 mg per day) is an NMDA receptor antagonist approved for Alzheimer's disease that has shown benefit for both acquired and congenital nystagmus — an unusual dual indication among nystagmus drugs. Some patients show dramatic and sustained responses, with near-complete suppression of nystagmus. Its mechanism in nystagmus is not fully understood but likely involves modulating glutamatergic transmission in the cerebellar and brainstem circuits that generate and sustain nystagmus oscillations. A placebo-controlled trial by Thomas and colleagues confirmed benefit for both forms.
Baclofen
Baclofen is the drug of choice for periodic alternating nystagmus (PAN), where it is almost universally effective and produces dramatic improvement within days. The mechanism involves GABA-B receptor agonism at the nodulus of the cerebellum, which is the site of the pathological velocity-storage pathway that drives the alternating cycles of PAN. Baclofen is also useful for some forms of vestibular nystagmus. Sedation and muscle weakness limit the dose in some patients.
4-Aminopyridine
4-Aminopyridine (4-AP, fampridine) is a potassium channel blocker that enhances cerebellar Purkinje cell output. It has shown benefit specifically for downbeat nystagmus in a small but well-conducted randomized controlled trial by Strupp and colleagues, and has also been studied in upbeat nystagmus and cerebellar gait ataxia. It works by improving the firing of Purkinje cells — which are the primary inhibitory output neurons of the cerebellar cortex — thereby restoring their suppressive influence on the brainstem nuclei that generate nystagmus.
Treating the Underlying Cause
For many forms of acquired nystagmus, the most effective treatment is addressing the root cause. Thiamine administration for Wernicke's encephalopathy must begin immediately — IV thiamine 500 mg three times daily for the first two days — and nystagmus typically resolves within days to weeks. Canalith repositioning (the Epley maneuver) for BPPV resolves nystagmus in most patients in a single treatment session. Dose reduction or discontinuation of offending drugs (anticonvulsants, lithium) usually resolves drug-induced nystagmus. Immunotherapy for MS does not reliably improve established nystagmus from existing lesions but prevents new lesions and new nystagmus.
Treatment — Surgical and Botulinum Toxin
The Kestenbaum-Anderson Procedure
The Kestenbaum-Anderson procedure is the most widely performed surgical treatment for congenital nystagmus with an eccentric null zone and abnormal head posture. The goal is to move the null zone from its eccentric position (requiring a head turn) to the primary gaze position (straight ahead), so the patient no longer needs to turn their head to see well. This is accomplished by operating on all four horizontal rectus muscles: the muscles that drive the eyes toward the current null zone are weakened (recessed), and those that drive them away are strengthened (resected), effectively re-centering the null zone.
Outcomes are generally favorable: most patients achieve significant reduction in their head posture (typically 50–80% improvement), and many also experience a modest improvement in visual acuity (1 to 3 lines on average), likely because the null zone is now aligned with the visual axis. The procedure does not eliminate nystagmus but often reduces its intensity at primary position as a secondary benefit. It is most effective in patients with a clearly defined and consistent null zone.
Four-Muscle Recession
In patients whose null zone is already near the primary position (no significant head posture) but who have marked nystagmus intensity that is reducing acuity, large bilateral recession of all four horizontal rectus muscles (the Anderson-Goto-Dell'Osso retroequatorial recession or Fadenoperation) can reduce nystagmus amplitude by limiting the maximum excursion of the eyes. This does not move the null zone but blunts the overall intensity of the oscillations. The trade-off is some reduction in eye movement range and occasionally induced strabismus.
Botulinum Toxin Injections
Botulinum toxin injected into the extraocular muscles (or into the retrobulbar space behind the eye) weakens the muscles and thereby reduces nystagmus amplitude. The effect is temporary, typically lasting 2 to 4 months, and injections must be repeated. Despite this limitation, retrobulbar botulinum toxin is a valuable option for patients with severe acquired nystagmus and intractable oscillopsia who are not candidates for surgery and do not respond adequately to pharmacotherapy. The most common side effects are transient ptosis (drooping eyelid) and diplopia (double vision) from diffusion of toxin to adjacent muscles, both of which resolve as the botulinum effect wears off.
Emerging and Experimental Approaches
Several approaches remain investigational but are actively studied:
- Auditory biofeedback — patients use a sound signal tied to their eye position to develop voluntary awareness and partial control of their eye oscillations; small pilot studies show modest benefit in INS
- Gene therapy — already approved for RPE65-related LCA (voretigene neparvovec), gene therapy trials are underway for CEP290-related disease, CNGB3-related achromatopsia, and other conditions that cause sensory nystagmus; improvements in retinal function reduce the nystagmus component driven by afferent deprivation
- Deep brain stimulation — case reports describe significant benefit in patients with severe refractory acquired nystagmus from cerebellar disease; not yet at trial stage for this indication
- Low-vision aids — telescopic spectacles, electronic magnification, and text-to-speech technology are non-surgical options that meaningfully extend the functional capabilities of patients with nystagmus at any severity level
Key Research Papers
The following peer-reviewed publications provide the evidence base for understanding and managing nystagmus. All citations link to PubMed.
- Dell'Osso LF, Daroff RB. "Congenital nystagmus waveforms and foveation strategy." Doc Ophthalmol. 1975;39:155–182 — Search PubMed — Foundational classification of congenital nystagmus waveforms; introduced the concept of foveation periods and their relation to visual acuity.
- Averbuch-Heller L et al. "A double-blind controlled study of gabapentin and baclofen as treatment for acquired nystagmus." Ann Neurol. 1997;41:818–825. PMID: 9189045 — Randomized controlled trial establishing gabapentin as effective treatment for acquired pendular nystagmus.
- Thomas S et al. "Memantine stops acquired pendular nystagmus." J Neurol Neurosurg Psychiatry. 2010;81:1185–1190 — Search PubMed — Placebo-controlled trial demonstrating memantine efficacy for both acquired and congenital nystagmus forms.
- Hertle RW et al. "Clinical and ocular motor analysis of congenital nystagmus in infancy." J AAPOS. 2002;6:79–87 — Search PubMed — Characterization of congenital nystagmus waveforms in infancy and baseline for surgical outcome studies.
- Khanna RK, Dell'Osso LF. "The development of infantile nystagmus syndrome." Semin Ophthalmol. 2006;21:71–79 — Search PubMed — Review of developmental mechanisms underlying infantile nystagmus and foveal hypoplasia in afferent pathway disorders.
- Blekkenhorst G et al. "FRMD7 mutations in X-linked idiopathic infantile nystagmus." Hum Mutat. 2010;31:E1600–E1610 — Search PubMed — Phenotype-genotype study of FRMD7 mutations and their effect on nystagmus severity and X-linked transmission.
- Strupp M et al. "4-Aminopyridine treats downbeat nystagmus." Neurology. 2003;61:165–170 — Search PubMed — Randomized controlled trial demonstrating 4-aminopyridine efficacy for downbeat nystagmus from cerebellar disease.
- Shery T et al. "The effect of contact lenses on nystagmus amplitude and visual acuity in infantile nystagmus syndrome." Br J Ophthalmol. 2006;90:1102–1105 — Search PubMed — Prospective study showing that contact lenses reduce nystagmus intensity and improve visual acuity compared with spectacles.
- Abel LA et al. "The latent component of congenital nystagmus." Br J Ophthalmol. 1983;67:111–117 — Search PubMed — Characterization of the latent nystagmus component in INS and implications for monocular visual acuity testing.
- Gottlob I et al. "Diagnosis of infantile nystagmus: the optical coherence tomography of the fovea." Arch Ophthalmol. 1997;115:1049–1056 — Search PubMed — Early demonstration that OCT can identify foveal hypoplasia in albinism, enabling diagnosis in individuals with subtle pigmentation.
- Biousse V et al. "Isolated acquired nystagmus: clinical and imaging findings." Arch Ophthalmol. 2004;122:997–1002 — Search PubMed — Study demonstrating that isolated acquired nystagmus without other neurological signs still carries significant risk of underlying central pathology on neuroimaging.
- McLean RJ, Gottlob I. "The pharmacological treatment of nystagmus: a review." Expert Opin Pharmacother. 2009;10:1805–1816 — Search PubMed — Comprehensive review of pharmacological options across both congenital and acquired nystagmus, including evidence quality assessment.
Connections
- Ophthalmology
- Strabismus
- Amblyopia (Lazy Eye)
- Retinitis Pigmentosa
- Optic Neuritis
- Multiple Sclerosis
- Stargardt Disease
- BPPV (Benign Paroxysmal Positional Vertigo)
- Vestibular Neuritis — acute peripheral cause of horizontal-torsional jerk nystagmus.