Macular Degeneration: History and Discovery
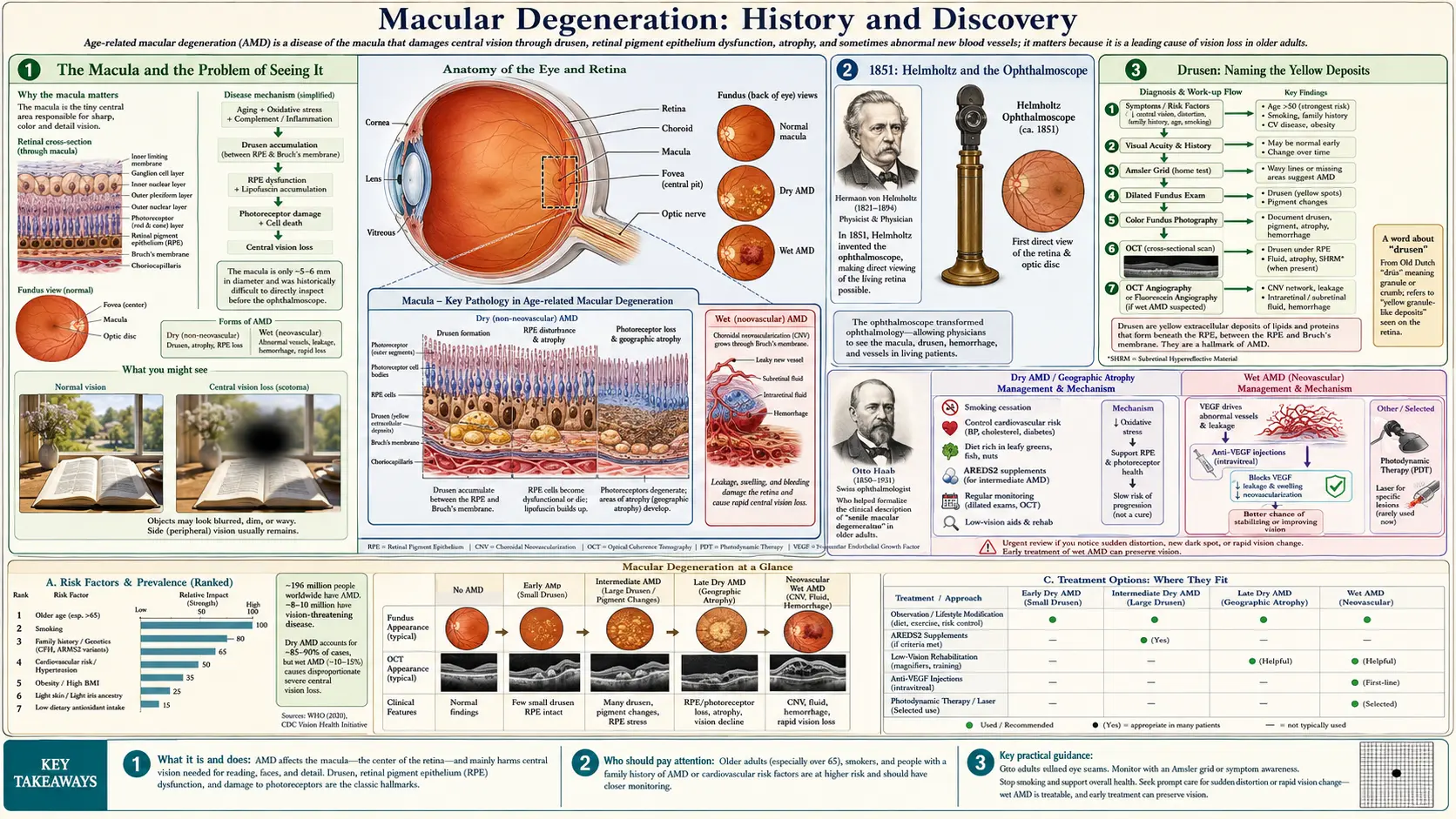
Age-related macular degeneration (AMD) is a disease of the macula, the tiny central island of the retina that we use for reading, recognizing faces, and seeing fine detail. As it advances, a blur or blank spot grows in the very middle of the visual field. For most of human history the condition was invisible to doctors: there was no way to look inside a living eye. That changed in 1851, when Hermann von Helmholtz built the ophthalmoscope and made the back of the eye visible for the first time. Within a generation, nineteenth-century observers had catalogued the yellow deposits called drusen, and around 1885 the Swiss ophthalmologist Otto Haab gathered these findings under the name “senile macular degeneration.” This page traces the long arc from that first look into the eye, through the split into “dry” and “wet” forms, to the revolution of the 2000s — when anti-VEGF injections turned wet AMD from a leading cause of blindness into a treatable disease, and the AREDS vitamin trials gave dry AMD its first evidence-based slowing strategy.
Table of Contents
- The Macula and the Problem of Seeing It
- 1851: Helmholtz and the Ophthalmoscope
- Drusen: Naming the Yellow Deposits
- Otto Haab and “Senile Macular Degeneration”
- Dry and Wet: Splitting the Disease in Two
- Lasers and Light: The First Treatments
- The VEGF Story and the Anti-VEGF Revolution
- AREDS, Smoking, and the Genetics of Risk
- Research Papers and References
- Connections
- Featured Videos
The Macula and the Problem of Seeing It
The retina lines the inside of the eye like film in a camera, but it is not uniform. At its center lies a small, yellow-tinged patch about five millimeters across called the macula, and at the heart of the macula is a pinpoint pit, the fovea, packed densely with cone photoreceptors. This tiny region carries almost all of our sharp, straight-ahead, detailed vision — the kind we use to read a word, thread a needle, or recognize a face. The rest of the retina handles peripheral and night vision. When the macula fails, a person can still walk around a room and see movement at the edges, yet a smudge or blank spot sits squarely where they are trying to look. That is the signature of macular degeneration.
For nearly all of recorded medicine, this kind of central vision loss was a mystery doctors could describe only from the outside. A patient could report that the middle of the page had gone gray, or that straight lines now bent and wavered, but the physician had no way to see the cause. The pupil is a dark window, and ordinary light reflected back out the way it came in, leaving the interior in shadow. Conditions we now separate cleanly — cataract clouding the lens, glaucoma damaging the optic nerve, degeneration eroding the macula — were lumped together under vague old labels such as amaurosis (blindness with no visible external cause) or “senile amblyopia,” dimness of sight in the old.
The entire history of macular degeneration as a recognized disease therefore depends on a single technological leap: a way to shine light into the living eye and actually see the retina at the back. Until that instrument existed, drusen, atrophy, and abnormal blood vessels were all hidden in the dark. The story properly begins, then, not with a doctor but with a physicist’s clever mirror.
1851: Helmholtz and the Ophthalmoscope
In 1850 and 1851, the German physician and physicist Hermann von Helmholtz (1821–1894) solved the puzzle of the dark pupil. Working in Königsberg, partly while thinking about how the eye reflects light, he realized that if an observer looked along the same path that light entered the eye, the dim glow returning from the illuminated retina could be caught and viewed. His first device was almost comically humble — cardboard, glue, and a few small glass plates acting as a partial mirror — but it worked. He called it the Augenspiegel, the “eye mirror”; the Greek-derived name ophthalmoscope came into general use a few years later. For the first time in history, a living human retina — its optic disc, its blood vessels, and its macula — could be seen and studied in a conscious patient.
It is hard to overstate what this opened up. Almost overnight, the back of the eye became visible territory, and a generation of clinicians began mapping it. Because the retina is the one place in the body where blood vessels and nervous tissue can be inspected directly and non-invasively, the ophthalmoscope quickly became important far beyond eye disease, revealing the retinal signs of diabetes, high blood pressure, and kidney disease. But its first and most natural use was to catalogue the diseases of the retina itself. The pale, atrophic patches, the yellow flecks, and the hemorrhages of what we now call AMD were among the findings that observers began recording within a couple of decades of Helmholtz’s invention.
The instrument also explains the timeline of this entire page. Notice that no credible “first description” of macular degeneration predates the 1850s, and the key descriptive milestones cluster in the 1870s and 1880s. That is not a coincidence: doctors could only begin to see, draw, and name what the disease did to the macula once they had a tool that let them look. The history of AMD is, in a real sense, the history of looking into the eye.
Drusen: Naming the Yellow Deposits
The earliest hallmark of macular degeneration that nineteenth-century observers could see were small, glistening, yellow-white deposits beneath the retina. The hunt to understand them began in the 1850s, almost as soon as the ophthalmoscope and the microscope could be turned on the eye together. The Dutch ophthalmologist Franciscus Cornelis Donders (1818–1889), examining the eyes of older people with failing sight, described these white flecks and called them Colloidkugeln — “colloid spheres” — arguing they were a degenerative deposit rather than fatty change, and famously likening them to gravestones marking dying cells of the underlying pigment layer. Around the same period the pathologist Carl Wedl gave an early histological description (about 1854).
The memorable name we still use today came from the German anatomist Heinrich Müller, who called the deposits drusen — a German mining and mineralogy word for a small rock cavity lined with sparkling crystals (a geode) — because under the microscope the rounded, glassy bodies seemed to glint. In 1874 the British surgeon Jonathan Hutchinson (working with the ophthalmoscopic observations of Warren Tay) published a careful account of an aging choroid “speckled with minute dots of yellowish-white deposits,” and laid out three stages: scattered yellow-white spots; their coalescence into larger patches; and finally hemorrhage at the macula. Remarkably, that nineteenth-century sketch of drusen progressing toward bleeding still maps onto the modern transition from dry AMD to wet AMD.
It is worth being honest about the limits of this early work. These observers were describing what they saw and arguing about what it meant; the deeper questions — what drusen are made of, why they form, how they relate to vision loss — would not be answered for more than a century, and some remain open today. We now know drusen are deposits of lipids, proteins, and cellular debris (including complement immune proteins) that accumulate between the retinal pigment epithelium and its underlying membrane. But the descriptive groundwork — that a constellation of yellow deposits in the aging macula signals a distinct disease process — was laid in those first decades of looking.
Otto Haab and “Senile Macular Degeneration”
By the 1880s, enough pieces were on the table to recognize macular degeneration as a clinical entity in its own right rather than a vague “dimness of age.” In 1884 the English ophthalmologist Edward Nettleship described a pattern of central atrophy he termed “central senile areolar choroidal atrophy.” Then, around 1885, the Swiss ophthalmologist Otto Haab (1850–1931) of Zurich published clinical descriptions of the atrophic and pigmentary changes in the macular region of older patients and applied the name that would stick for nearly a century: “senile macular degeneration.” Haab is widely credited with first delineating the condition as a defined diagnosis, and his name is the one most often cited as marking AMD’s entry into the medical vocabulary.
Two points of accuracy deserve emphasis, because medical history is easy to oversimplify. First, no single person “discovered” macular degeneration; Haab synthesized and named a picture that Donders, Müller, Hutchinson, Nettleship, and others had been assembling for thirty years. Crediting him is shorthand for a collective achievement, not the work of one pair of eyes. Second, the very word senile reflects the limited understanding of the time: doctors saw the disease in old people and assumed it was simply wear and tear, “just aging.” The modern term age-related macular degeneration deliberately replaced “senile” in the late twentieth century to shed that fatalism — age is the largest risk factor, but the disease is now understood as a specific process driven by genetics, immune activity, and environment, not an inevitable consequence of getting old.
For roughly the next eighty years after Haab, this is essentially where matters stood. Clinicians could diagnose macular degeneration with an ophthalmoscope, grade its severity by the look of the drusen and atrophy, and watch it progress — but they could do almost nothing to change its course. The disease was named, described, and understood to be common, yet it remained, for the patient, a slow and untreatable erosion of central sight. The breakthroughs that would change that lay in the second half of the twentieth century, and they came first from light, then from biology.
Dry and Wet: Splitting the Disease in Two
One of the most important conceptual advances was the recognition that “macular degeneration” is not one disease but two related ones, with very different tempos and, eventually, very different treatments. Clinicians divide AMD into a dry (atrophic) form and a wet (neovascular or exudative) form. The distinction was sharpened enormously in the 1960s and beyond, when the new technique of fluorescein angiography — injecting a fluorescent dye into the bloodstream and photographing it as it traced through the retinal and choroidal vessels — let doctors see, for the first time, the abnormal leaking blood vessels that define the wet form.
Dry AMD is the common, slow form, accounting for the large majority of cases. It is marked by drusen and by the gradual thinning and death of the retinal pigment epithelium and photoreceptors. In its advanced stage, called geographic atrophy, well-defined islands of retinal tissue waste away, and central vision fades over years. Wet AMD is the less common but far more dangerous form: fragile new blood vessels grow up from the choroid beneath the retina (choroidal neovascularization), then leak fluid and blood. Because these vessels are abnormal and leaky, wet AMD can destroy central vision rapidly — sometimes within days or weeks — and a frequent early warning sign is the sudden distortion of straight lines, where a doorframe or line of text appears bent or wavy (metamorphopsia).
That warning sign gave rise to one of the simplest and most enduring tools in all of ophthalmology. In 1947 the Swiss ophthalmologist Marc Amsler (1891–1968) introduced the Amsler grid, a small printed square of evenly spaced lines with a central dot. A patient covers one eye, stares at the dot, and notes whether any of the lines look wavy, broken, or missing. Decades later, the Amsler grid remains a standard at-home self-check that helps people with AMD catch the conversion to the wet form early — which, in the anti-VEGF era, can mean the difference between saved and lost vision. The grid is a reminder that not every advance in this field is high technology; sometimes it is a clever idea on a card.
Lasers and Light: The First Treatments
The first treatments that could actually alter the course of wet AMD arrived in the late twentieth century, and they used light to attack the leaking vessels. The earliest approach was thermal laser photocoagulation: focusing an intense laser beam to burn and seal the abnormal blood vessels. Its benefit was established by the landmark Macular Photocoagulation Study (MPS), a set of National Eye Institute–sponsored randomized trials that recruited patients beginning in 1979 and reported through the 1980s and early 1990s. The MPS proved that argon-laser treatment of certain choroidal neovascular lesions could prevent or delay severe vision loss for years — the first rigorous evidence that anything could be done.
But thermal laser had a cruel limitation: the burn destroys retinal tissue wherever it lands. If the abnormal vessels sat directly under the center of the macula — the subfoveal location, which is common — treating them meant burning the very spot responsible for central vision, trading a slow loss for an immediate one. Doctors needed a way to close the bad vessels without scorching the retina. That came around the turn of the millennium with photodynamic therapy (PDT) using the drug verteporfin (Visudyne). PDT is a two-step process: a light-sensitive drug is infused into the bloodstream, and then a cool, non-thermal laser of a specific wavelength is shone on the macula, activating the drug only where it has pooled in the abnormal vessels and closing them with far less collateral damage. Verteporfin PDT was first approved in Switzerland in December 1999 and by the U.S. FDA in April 2000, becoming the first pharmacologic treatment for neovascular AMD.
PDT was a genuine step forward, and it is still used in selected cases today. But it is important to be clear about what it did and did not achieve: for most patients, photodynamic therapy slowed vision loss rather than restoring sight, and many eyes continued to decline despite repeated sessions. Both laser approaches treated the leaking vessels as a plumbing problem — seal the leak — without addressing the biological signal that was driving the vessels to grow in the first place. The truly transformative breakthrough required understanding that signal, and it was already taking shape in cancer-research laboratories that, at first glance, had nothing to do with the eye.
The VEGF Story and the Anti-VEGF Revolution
The single most important development in the history of macular degeneration grew out of a question about tumors. In 1971 the surgeon-scientist Judah Folkman proposed that solid cancers cannot grow beyond a tiny size unless they recruit their own blood supply, and that blocking this angiogenesis might starve them. The hunt was on for the molecular signal that tells the body to sprout new vessels. In 1989, Napoleone Ferrara and colleagues at the biotechnology company Genentech cloned and characterized that signal: a protein they named vascular endothelial growth factor (VEGF). It turned out to be the master switch for abnormal vessel growth — and abnormal vessel growth is exactly what destroys vision in wet AMD.
The insight that reframed wet AMD was this: the destructive choroidal neovascularization was being driven by VEGF. If you could neutralize VEGF inside the eye, you might stop the vessels from growing and leaking. The proof came with astonishing speed in the 2000s. The first VEGF-blocking drug approved for the eye was pegaptanib (Macugen), an aptamer that the FDA cleared in December 2004; it could slow vision loss but rarely improved sight. The true turning point was ranibizumab (Lucentis), an antibody fragment engineered specifically for the eye, FDA-approved in 2006. In its pivotal trials, ranibizumab did something no prior treatment had managed: not only did it halt vision loss in the great majority of patients, a substantial fraction actually gained meaningful vision. For the first time, wet AMD could be pushed backward.
A parallel and very human story unfolded alongside Lucentis. Bevacizumab (Avastin) — a closely related, full-length anti-VEGF antibody (also developed at Genentech, building on Ferrara’s work) that had been approved for colon cancer — was found by retina specialists to work in the eye when injected in tiny doses, at a tiny fraction of the cost. Used off-label, Avastin became, and remains, one of the most widely used AMD treatments in the world, and a major U.S. National Eye Institute trial (CATT) later found it broadly comparable to Lucentis for vision outcomes. The field then expanded further with aflibercept (Eylea), a decoy-receptor “VEGF trap” approved in November 2011 that allowed longer intervals between injections, and more recently with longer-acting second-generation agents such as brolucizumab and the dual-action faricimab. The practical upshot is profound and worth stating plainly: a disease that was, within living memory, a leading cause of irreversible blindness in older adults became, for its most aggressive form, a treatable condition — managed with periodic injections that preserve, and often improve, sight.
AREDS, Smoking, and the Genetics of Risk
The anti-VEGF revolution transformed wet AMD, but most people with macular degeneration have the slow, dry form, for which there was long no proven treatment at all. The key advance here was nutritional, and it came from a single large, rigorous trial. The Age-Related Eye Disease Study (AREDS), sponsored by the U.S. National Eye Institute and published in 2001, followed several thousand participants and found that a specific high-dose supplement combination — vitamin C, vitamin E, beta-carotene, zinc, and copper — reduced the risk of progressing to advanced AMD by roughly a quarter in people who already had intermediate disease. It was the first evidence that anything could slow dry AMD.
The follow-up study, AREDS2, published in 2013, refined the formula. It replaced beta-carotene — which had been linked to a higher lung-cancer risk in smokers — with the macular pigments lutein and zeaxanthin, which proved at least as effective and safer. The modern “AREDS2 formula” sold in pharmacies today comes directly from this trial. Two cautions matter for readers, and they reflect what the studies actually showed: these supplements are intended to slow progression in people with intermediate or advanced AMD — they are not a cure, they do not restore lost vision, and the evidence does not support them as a preventive for people with healthy eyes or only the earliest changes. They should be chosen with an eye doctor’s guidance, especially by current or former smokers.
Finally, the late twentieth and early twenty-first centuries reframed why people get AMD. Two threads stand out. The first is smoking, now firmly established as the strongest modifiable risk factor, roughly multiplying a person’s risk — making quitting the single most powerful thing an individual can do to protect their macula. The second is genetics. In 2005, in a landmark convergence, four independent research groups reported almost simultaneously that a common variant in the complement factor H (CFH) gene — a regulator of the immune system’s alternative complement pathway — strongly raises the risk of AMD. This was a watershed: it tied the disease to the immune system and inflammation, helped explain why complement proteins are found inside drusen, and pointed research toward complement-targeting therapies for geographic atrophy. From a nineteenth-century “senile” deposit of unknown cause, drusen had become a clue to the immunology of an aging retina — the latest turn in a story that began with a physicist’s cardboard mirror.
Research Papers and References
The list below combines key peer-reviewed sources on the history and treatment of age-related macular degeneration with curated PubMed topic-search links into the historical and clinical literature. Where a stable DOI or PMID is given, the link opens that record directly; the remaining links open a PubMed topic search at the U.S. National Library of Medicine. All links open in a new tab.
- de Jong PTVM. A Historical Analysis of the Quest for the Origins of Aging Macula Disorder, the Tissues Involved, and Its Terminology. Ophthalmology and Eye Diseases. 2016;8:5–14. — doi:10.4137/OED.S40523
- de Jong PTVM. Elusive drusen and changing terminology of AMD. Eye (London). 2018;32(5):904–914. — doi:10.1038/eye.2017.298
- Treatment of Age-Related Macular Degeneration with Photodynamic Therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neovascularization in AMD with verteporfin: one-year results of 2 randomized clinical trials — TAP report. Archives of Ophthalmology. 1999;117(10):1329–1345. — PMID: 10532441
- Macular Photocoagulation Study Group. Argon laser photocoagulation for neovascular maculopathy: five-year results from randomized clinical trials. Archives of Ophthalmology. 1991;109(8):1109–1114. — PMID: 1714270
- Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled clinical trial of high-dose supplementation with vitamins C and E, beta-carotene, and zinc for age-related macular degeneration (AREDS report no. 8). Archives of Ophthalmology. 2001;119(10):1417–1436. — PMID: 11594942
- Age-Related Eye Disease Study 2 (AREDS2) Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the AREDS2 randomized clinical trial. JAMA. 2013;309(19):2005–2015. — doi:10.1001/jama.2013.4997
- Klein RJ, Zeiss C, Chew EY, et al. Complement factor H polymorphism in age-related macular degeneration. Science. 2005;308(5720):385–389. — doi:10.1126/science.1109557
- Gass JDM. Pathogenesis of disciform detachment of the neuroepithelium (a classic clinicopathologic series on macular degeneration). American Journal of Ophthalmology. 1967. — PubMed: Gass disciform macular degeneration
- History of the ophthalmoscope and Hermann von Helmholtz — PubMed: ophthalmoscope history (Helmholtz)
- Drusen — history, terminology, and pathology in age-related macular degeneration — PubMed: drusen history and terminology
- Ranibizumab (Lucentis) pivotal trials for neovascular AMD (MARINA / ANCHOR) — PubMed: ranibizumab MARINA ANCHOR trials
- Bevacizumab versus ranibizumab for AMD — the CATT comparison of anti-VEGF therapies — PubMed: CATT bevacizumab vs ranibizumab
- Discovery of vascular endothelial growth factor (VEGF) — Ferrara and the biology of angiogenesis — PubMed: VEGF discovery (Ferrara)
- Marc Amsler grid and the detection of metamorphopsia in macular disease — PubMed: Amsler grid and metamorphopsia
External Authoritative Resources
- National Eye Institute (NIH) — Age-Related Macular Degeneration
- EyeWiki (American Academy of Ophthalmology) — Age-Related Macular Degeneration
- PubMed — All research on the history of age-related macular degeneration
Connections
- Ophthalmology
- Macular Degeneration (main article)
- Cataracts
- Glaucoma
- Glaucoma: History and Discovery
- Diabetes
- Diabetic Retinopathy & Complications
- All Conditions