Corneal Ulcer
A corneal ulcer is an open sore on the cornea — the clear, dome-shaped surface at the very front of your eye — most often caused by a bacterial, fungal, viral, or parasitic infection. Because the cornea is the eye's primary focusing surface, even a small scar in the center of your field of view can permanently blur your vision to the equivalent of a strong uncorrected prescription. Corneal ulcers are a vision emergency: do not wait to see whether symptoms improve on their own. The single biggest risk factor in high-income countries is contact lens wear, particularly sleeping in lenses or rinsing them with tap water. If your eye is suddenly painful, red, and your vision has changed — especially if you wear contact lenses — remove the lens immediately and see an ophthalmologist the same day. Hours matter. Delay converts a treatable infection into a permanent scar.
- Overview and Definition
- The Cornea — Anatomy and Vulnerability
- Types of Infectious Keratitis
- Risk Factors
- Symptoms and Clinical Presentation
- Diagnosis
- Treatment by Organism
- Contact Lens Safety
- Complications
- Prognosis and Recovery
- Key Research Papers
- Connections
Overview and Definition
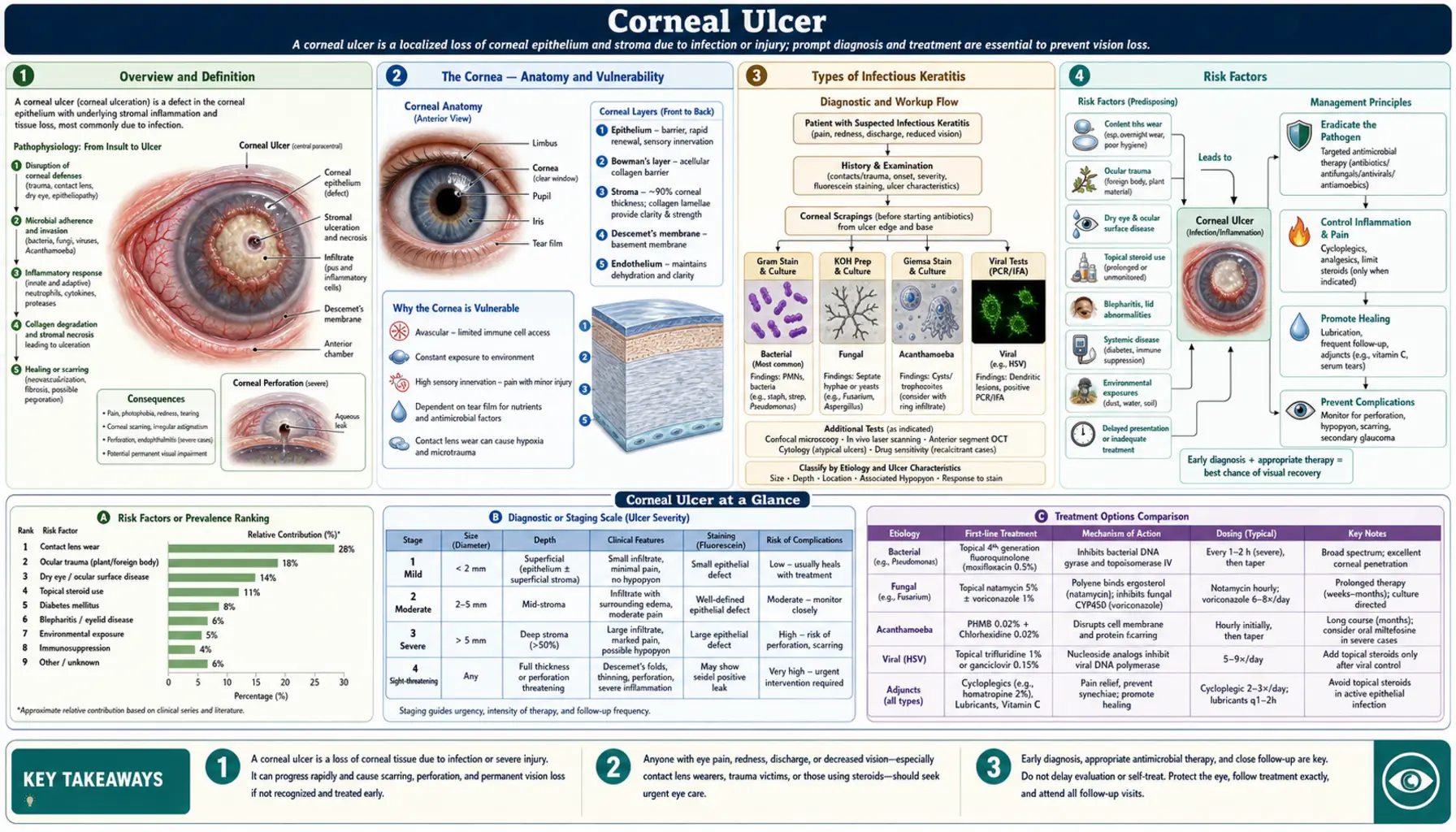
A corneal ulcer — technically called infectious keratitis with ulceration — is a breakdown of the corneal epithelium, and often the underlying stromal layers, caused by bacterial, fungal, viral, or parasitic organisms. The term "ulcer" reflects a true tissue defect: the protective outer cell layer has been breached, and the infectious agent is actively destroying corneal tissue beneath it.
This is a vision-threatening emergency. The cornea is only about 0.5 mm thick at its center — roughly the thickness of a credit card — and it performs the majority of the eye's focusing power. Even a small scar in the visual axis can permanently reduce vision to levels that require a strong corrective prescription, and a large or deep ulcer can perforate the cornea entirely. Worldwide, infectious keratitis accounts for an estimated 1.5 to 2 million new cases per year and is one of the leading causes of corneal blindness globally, particularly in tropical and low-resource settings where agricultural trauma and vitamin A deficiency are common triggers.
In high-income countries, the overwhelming majority of bacterial cases are driven by contact lens wear — a largely preventable cause. Recognizing the early warning signs and acting immediately is the single most important thing a patient can do to preserve their vision.
The Cornea — Anatomy and Vulnerability
Understanding why the cornea is so vulnerable to infection requires a brief look at its architecture. Five distinct layers make up the cornea, each with a different capacity to heal:
- Epithelium — five to six cell layers thick; forms a continuous tight-junction barrier; regenerates every seven days under normal conditions; the first and primary line of defense against infection.
- Bowman's layer — an acellular condensed collagen zone just beneath the epithelium; once injured it does not regenerate, leaving a permanent opacity.
- Stroma — constitutes about 90% of corneal thickness; composed of collagen lamellae arranged in a precise lattice that gives the cornea its optical transparency; infection here causes visible white opacity and structural weakening.
- Descemet's membrane — a thick basement membrane that is relatively resistant to enzymatic degradation; serves as the last barrier before the interior of the eye.
- Endothelium — a single layer of cells that actively pumps fluid out of the stroma to keep it clear; critically, these cells do not regenerate in adult humans. Endothelial failure from infection or inflammation causes permanent corneal edema and irreversible vision loss.
The cornea is also unusual in being entirely avascular — it derives its oxygen from the tear film and aqueous humor rather than blood vessels. This is essential for optical clarity, but it means that the eye's immune defenses arrive slowly once an infection is established. Neutrophils and macrophages must migrate from the limbal vasculature at the corneal rim; by the time a significant inflammatory response mounts, a virulent organism such as Pseudomonas aeruginosa may have already degraded substantial stromal tissue. Any disruption to the epithelium — from contact lens trauma, dry eye, chemical splash, UV exposure, or eyelid abnormalities — creates an entry point that the cornea cannot quickly seal against.
Types of Infectious Keratitis
Bacterial Keratitis
The most common form in contact lens wearers in developed countries. The organism most feared is Pseudomonas aeruginosa, which dominates soft contact lens-associated infections. Pseudomonas produces potent proteolytic enzymes (elastase, alkaline protease) that can liquefy stromal collagen within 24 to 48 hours, causing a ring abscess pattern and copious mucopurulent discharge. Other important bacteria include Staphylococcus aureus, Streptococcus pneumoniae, and various gram-negative enteric organisms. Slit-lamp appearance: a gray-white stromal infiltrate with an overlying fluorescein-staining epithelial defect. Hypopyon — a visible pus level in the anterior chamber — indicates severe infection and does not mean bacteria have entered the eye interior; it is a sterile inflammatory reaction to adjacent infection.
Fungal Keratitis
Caused by filamentous fungi (primarily Fusarium solani and Aspergillus species in tropical and subtropical climates) or by Candida in immunocompromised patients. The classic trigger is vegetative or soil trauma to the eye — an injury from a plant branch, grain husk, or agricultural tool. Slit-lamp appearance: a dry, rough-textured gray-white infiltrate with feathery or filamentous margins and satellite lesions. A critical danger is misdiagnosis as bacterial keratitis: the infiltrate can look similar in the early stages, and empiric antibiotics have no effect on fungi while allowing the infection to advance. The 2006 global epidemic of Fusarium keratitis linked to Bausch & Lomb's ReNu MoistureLoc contact lens solution demonstrated that this pathogen can affect otherwise healthy contact lens wearers, not only agricultural workers.
Herpes Simplex Virus (HSV) Keratitis
The most common cause of infectious corneal blindness in the developed world. HSV-1 establishes latent infection in the trigeminal ganglion after primary exposure and can reactivate in response to UV light, fever, emotional stress, or immunosuppression. Two clinically distinct forms:
- Epithelial (dendritic) keratitis: The classic branching, linear dendrite with terminal end-bulbs is pathognomonic for HSV. It stains brilliantly with fluorescein under cobalt blue light and with rose bengal dye at the terminal bulbs. This form is directly virus-mediated.
- Stromal (disciform) keratitis: Immune-mediated injury, not direct viral replication. Characterized by a round central stromal opacity with folds in Descemet's membrane and elevated intraocular pressure from trabeculitis. Can recur and cause cumulative stromal scarring with each episode.
Critical warning: Topical corticosteroids are absolutely contraindicated in active epithelial HSV keratitis. Steroids suppress the immune response that limits viral replication, allowing the dendrite to expand into a large, irregular "geographic ulcer" that can destroy the entire corneal surface. Steroids are used cautiously, only with concurrent antiviral cover, for the immune-mediated stromal form.
Acanthamoeba Keratitis
Acanthamoeba are free-living amoebae found ubiquitously in water — tap water, swimming pools, hot tubs, lakes, and soil. In practical terms, virtually every case occurs in a contact lens wearer who has either rinsed their lenses or lens case with tap water, swum or showered while wearing lenses, or stored lenses in homemade saline. Two clinical hallmarks make this diagnosis distinctive:
- Pain out of proportion to appearance: Very early in the infection, before visible corneal opacification, the patient experiences severe, burning, debilitating pain. This discordance — severe pain with a relatively normal-looking eye — is a red flag that should immediately raise suspicion for Acanthamoeba.
- Perineural infiltrates: Visible inflammation tracking along corneal nerve fibers on slit-lamp examination, and directly visible as cysts on confocal microscopy. A later ring infiltrate surrounding the central ulcer is a well-known but unfortunately late sign associated with worse prognosis.
The tragedy of Acanthamoeba keratitis is diagnostic delay. Average time from symptom onset to correct diagnosis has historically been three to four months. During that time, the patient is typically treated with antibiotics and sometimes steroids — neither of which helps and the latter of which worsens the outcome. Early diagnosis, ideally within weeks of symptom onset before the ring infiltrate forms, is the single most important determinant of whether the patient keeps functional vision without a corneal transplant.
Risk Factors
Contact lens wear is the dominant modifiable risk factor in high-income countries. Specific high-risk behaviors include: sleeping in lenses (10 to 15 times increased risk of bacterial keratitis compared with daily removal), wearing disposable lenses beyond their replacement schedule, rinsing lenses or cases with tap water (primary Acanthamoeba risk), swimming or showering with lenses in, and poor lens case hygiene (cases accumulate Pseudomonas biofilm rapidly). The estimated incidence of microbial keratitis is approximately 1 in 10,000 per year for daily contact lens wearers, rising to 1 in 500 per year for extended (overnight) wearers.
Ocular trauma is the dominant risk factor in developing countries and agricultural settings. Plant, vegetable, or soil injuries carry a high risk of fungal keratitis; dirty projectile injuries risk polymicrobial bacterial infection.
Other important risk factors include:
- Pre-existing ocular surface disease: severe dry eye, bullous keratopathy (failed endothelial cells), trichiasis (inturned eyelashes), lagophthalmos (inability to fully close the eyelids)
- Prior ocular surgery or corneal transplant
- Topical corticosteroid drops — applied to an eye with undiagnosed viral or fungal infection, these dramatically accelerate tissue destruction
- Systemic immunosuppression: high-dose corticosteroids, HIV, organ transplant immunosuppression, chemotherapy — increase risk of Candida and atypical organisms
- Vitamin A deficiency: causes corneal xerosis (dryness and metaplasia of the epithelium) progressing to keratomalacia (corneal melting) — a major cause of childhood corneal blindness globally, rare in high-income countries
- Previous HSV keratitis: each recurrence increases the probability of the next
Symptoms and Clinical Presentation
A corneal ulcer produces a characteristic cluster of symptoms that distinguish it from the much more common and less dangerous condition of conjunctivitis (pink eye). Knowing these differences can help you decide whether you need to see a doctor today versus waiting for a routine appointment:
- Reduced visual acuity — blurred or decreased vision proportional to how close the ulcer is to the center of the cornea; peripheral ulcers may cause minimal visual disturbance, central ulcers often cause significant blurring. Vision loss does NOT occur with simple conjunctivitis.
- Severe pain — corneal ulcers are painful. The cornea has the highest density of pain receptors of any surface tissue in the body. Pain is out of proportion to what you would expect with a simple "red eye." Acanthamoeba keratitis is particularly notorious for extreme, burning, debilitating pain.
- Photophobia — intense sensitivity to light, often with involuntary eyelid closure (blepharospasm). Mild photophobia can occur with conjunctivitis, but severe photophobia that makes it difficult to open the eye in normal room lighting suggests corneal or anterior chamber involvement.
- Foreign body sensation and excessive tearing
- Discharge: purulent (thick yellow-green pus) suggests bacterial infection; watery or mucoid discharge suggests viral; minimal early discharge with severe pain suggests Acanthamoeba
- Eyelid swelling from reactive inflammation
- Visible white spot on the cornea — in advanced or larger ulcers, a white or grayish opacity may be visible to the naked eye without any equipment
- Hypopyon — a visible horizontal white pus level inside the eye, below the pupil; this indicates severe keratitis and is a clear sign that an ophthalmologist needs to see this eye the same day
If you have a red eye and also have any visual change, severe pain, or photophobia, this is not conjunctivitis until proven otherwise. Do not apply over-the-counter eye drops and wait. See an eye care provider immediately.
Diagnosis
Diagnosis of a corneal ulcer requires slit-lamp examination by an ophthalmologist or experienced optometrist. The key diagnostic steps are:
- Slit-lamp biomicroscopy: The cornea is examined under high magnification with a bright, focused beam of light. This defines the ulcer size, depth, and character. Fluorescein dye (which stains green under cobalt blue light) outlines the epithelial defect. Rose bengal stain highlights dead epithelial cells and viral lesions. A Seidel test (the fluorescein pool dilutes and streams with aqueous if positive) can detect corneal perforation. The slit lamp can identify the dendritic pattern of HSV, the feathery infiltrate of fungal infection, or the perineural infiltrates of Acanthamoeba.
- Corneal scraping and culture: For any significant ulcer — larger than 1 mm, centrally located, not a textbook HSV dendrite in a low-risk patient — scraping the base and edges of the ulcer with a sterile spatula provides material for Gram stain (bacteria), KOH preparation and calcofluor white fluorescence microscopy (fungal hyphae, Acanthamoeba cysts), Giemsa stain, and bacterial and fungal culture. PCR is increasingly used for rapid detection of HSV, VZV, and Acanthamoeba DNA.
- Confocal microscopy: A non-invasive imaging modality that provides in vivo, high-resolution visualization of corneal cell layers. It can directly visualize fungal hyphae and — crucially — the double-walled cysts of Acanthamoeba in the stroma, enabling diagnosis within hours rather than weeks when used by an experienced examiner. Increasingly available at tertiary eye centers.
- Clinical diagnosis alone is appropriate for classic HSV epithelial dendrite in a patient without contact lenses and no immunosuppression — the pattern is sufficiently pathognomonic that scraping adds little and may worsen the epithelial defect.
Treatment by Organism
Bacterial Keratitis
Empiric therapy begins immediately, before culture results return. For most community-acquired bacterial keratitis in a contact lens wearer, fluoroquinolone monotherapy is the standard of care: moxifloxacin 0.5% or ciprofloxacin 0.3% applied every one hour while awake for the first 24 to 48 hours, then tapered as the ulcer responds. Fluoroquinolones provide excellent coverage for Pseudomonas (ciprofloxacin and moxifloxacin both have strong activity) and most gram-positive pathogens. Do not use ofloxacin as first choice for contact lens-associated keratitis — its Pseudomonas activity is comparatively lower.
For severe, rapidly progressive, non-responding, or hospital-acquired cases: fortified topical drops compounded by a pharmacy are required. The classic regimen combines vancomycin 25–50 mg/mL (covering methicillin-resistant Staphylococcus and gram-positives) with tobramycin 14 mg/mL or ceftazidime 50 mg/mL (covering Pseudomonas and gram-negatives), instilled alternately every 30 to 60 minutes around the clock initially. Corticosteroids are withheld until the organism is identified and a favorable treatment response is established.
Fungal Keratitis
Natamycin 5% ophthalmic suspension is the only FDA-approved topical antifungal for keratitis and is the first-line agent for filamentous fungi, particularly Fusarium. Clinical trial data from the Mycotic Ulcer Treatment Trial (MUTT I) demonstrated natamycin's superiority over voriconazole for Fusarium keratitis specifically. Voriconazole 1% (off-label; prepared by compounding pharmacy) provides better activity against Aspergillus and may be used as monotherapy or in combination. Amphotericin B 0.15% is preferred for Candida keratitis. Treatment duration is weeks to months — far longer than bacterial treatment. Topical corticosteroids are absolutely contraindicated. If medical treatment fails — infiltrate deepening despite adequate therapy, or perforation threatening — therapeutic penetrating keratoplasty (full-thickness corneal transplant) may be required, though outcomes in active fungal infection are poor.
Herpes Simplex Keratitis (Epithelial Form)
Antiviral therapy is highly effective for epithelial HSV keratitis. Options include:
- Ganciclovir 0.15% ophthalmic gel — five times daily; well tolerated; first-line in many guidelines
- Trifluridine 1% drops — every two hours up to nine doses daily for 14 days; effective but higher epithelial toxicity with prolonged use
- Oral acyclovir (400 mg five times daily) or valacyclovir (1 g three times daily) — equivalent efficacy to topical agents with easier compliance
Gentle debridement — wiping away the loose infected epithelial cells with a cotton-tipped applicator — accelerates healing. Never add topical corticosteroids to active epithelial keratitis. For the stromal (disciform) immune form, topical corticosteroids with concurrent antiviral cover are appropriate. Long-term suppressive therapy with oral acyclovir 400 mg twice daily reduces the rate of recurrence by approximately 41% (HEDS Prevention Trial, PMID 9682040) and is recommended for patients with two or more episodes per year.
Acanthamoeba Keratitis
Treatment is prolonged and intensive. The standard regimen is:
- Polyhexamethylene biguanide (PHMB) 0.02% drops — initially every hour around the clock, then tapered over months
- Propamidine isethionate (Brolene) 0.1% drops — used in combination with PHMB
- Chlorhexidine 0.02% is an alternative to PHMB with similar efficacy
Minimum treatment duration is three to six months, because the cyst form of Acanthamoeba is extraordinarily resistant to most disinfectants and requires sustained drug exposure to eradicate. Topical corticosteroids should be avoided (though there is limited debate about their use in managing the immune response in very late disease). Prognosis is directly tied to how early treatment begins: patients treated before the ring infiltrate appears generally do well with medical therapy alone; those treated late frequently require penetrating keratoplasty, and even then outcomes are guarded because residual organisms in the stroma can infect the donor button.
Contact Lens Safety
Contact lens-related keratitis is almost entirely preventable. The following behaviors are the primary drivers of risk:
- Never sleep in contact lenses — even lenses labeled "extended wear" carry a 10 to 15 times higher risk of bacterial keratitis compared with lenses removed every night. The cornea needs overnight oxygen exposure; lenses worn during sleep dramatically reduce oxygen delivery and create conditions that favor bacterial colonization.
- Never use tap water near contact lenses — this is the single most important rule for preventing Acanthamoeba keratitis. Never rinse lenses, lens cases, or your hands (before handling lenses) with tap water. Never top off lens solution — always discard old solution and fill with fresh.
- Never swim or shower with lenses in — pools, lakes, hot tubs, and tap water all carry Acanthamoeba. Remove lenses before any water exposure.
- Replace lenses on schedule — wearing disposable lenses beyond their intended replacement interval allows protein and lipid deposits to accumulate, increasing the risk of infection and inflammatory reactions.
- Replace the lens case every three months — lens cases are a primary reservoir for Pseudomonas biofilm. Wash the case with multipurpose solution (never water), rub it, and leave it face-down on a clean tissue to air dry.
- Remove lenses immediately at the first sign of redness, pain, or visual change — do not try to "wait it out." If symptoms do not resolve within a few hours of lens removal, see an eye care provider the same day.
Estimated annual incidence: approximately 1 in 10,000 for daily-wear soft contact lens users, 1 in 500 for extended (overnight) wear users. Rigid gas-permeable lenses carry lower risk than soft lenses because they are less adherent to the corneal surface and are not typically worn overnight.
Complications
Untreated or inadequately treated corneal ulcers can cause severe, permanent harm:
- Corneal scarring: Any opacity in the visual axis — even a small one — reduces best-corrected visual acuity. Scars from healed ulcers are permanent unless surgically addressed. Central scars often require penetrating keratoplasty (corneal transplant) to restore vision.
- Corneal perforation: Bacterial proteases, particularly from Pseudomonas, can dissolve stromal collagen so rapidly that the cornea perforates within 24 to 48 hours without treatment. A perforated cornea loses anterior chamber depth, risks lens and iris prolapse, and creates an entry route for bacteria into the interior of the eye.
- Endophthalmitis: Infection of the vitreous cavity — a catastrophic complication that often results in severe, permanent vision loss despite aggressive treatment. Can follow perforation or penetrating surgery in an infected eye.
- Corneal neovascularization: Chronic inflammation stimulates blood vessel growth into the normally avascular cornea. These vessels become permanent and can obstruct vision, cause irregular astigmatism, and create antibodies that complicate future corneal transplantation.
- Secondary glaucoma: Elevated intraocular pressure from trabeculitis, synechiae (adhesions between the iris and lens), or steroid treatment can damage the optic nerve.
- Recurrent corneal erosion syndrome: After a healed epithelial ulcer, the newly regenerated epithelium may not adhere properly to the basement membrane, causing recurring painful epithelial sloughing, typically upon waking.
- Amblyopia (in children): Any corneal opacity that obstructs the visual axis during the critical period of visual development (birth to approximately age 7) can cause permanent deprivation amblyopia — the brain stops developing the connections for that eye — even if the opacity is later surgically removed.
Prognosis and Recovery
Outcomes depend heavily on the causative organism, the ulcer's size and location, and — above all — how quickly appropriate treatment begins.
Bacterial keratitis: With prompt, appropriate antibiotic therapy, most peripheral bacterial ulcers heal without permanent visual loss. Central ulcers, even when treated effectively, leave varying degrees of scarring in the visual axis. Pseudomonas keratitis is particularly destructive and can progress to perforation within 48 hours without treatment; with aggressive fluoroquinolone therapy, most cases do respond, but central ulcers commonly leave significant opacity.
Fungal keratitis: Generally carries a worse prognosis than bacterial keratitis. Medical treatment failure requiring therapeutic penetrating keratoplasty occurs in approximately 15 to 27% of cases across published series. Outcomes in keratoplasty for active fungal infection are poor; the procedure is primarily used to excise actively infected tissue.
HSV keratitis: First episode of epithelial keratitis typically heals well with antiviral therapy, leaving minimal scarring. However, HSV is a recurrent disease — each episode of stromal keratitis causes cumulative immune-mediated scarring. After three or more episodes of stromal disease, significant visual impairment is common. Long-term suppressive therapy (acyclovir 400 mg twice daily) reduces recurrence risk by about 41% and is recommended for patients with recurrent disease.
Acanthamoeba keratitis: Historically, 50 to 80% of patients required penetrating keratoplasty and outcomes were poor. With growing availability of confocal microscopy enabling earlier diagnosis, and prompt initiation of PHMB-based therapy, outcomes have improved substantially. Patients diagnosed before ring infiltrate formation who receive immediate aggressive treatment have reasonable prospects of retaining useful vision with medical therapy alone. The key message remains: early diagnosis is everything.
Penetrating keratoplasty (full-thickness corneal transplant) is required in approximately 5 to 15% of infectious keratitis cases in developed-country settings — primarily for cases with perforation, extensive scarring in the visual axis following healed infection, or failure of medical therapy for fungal or Acanthamoeba infections. Graft survival in eyes with prior infection is somewhat lower than for other indications due to corneal neovascularization and the increased risk of immune rejection.
Key Research Papers
- Herpetic Eye Disease Study Group. "Acyclovir for the prevention of recurrent herpes simplex virus eye disease." N Engl J Med. 1998;339:300–306 — Search PubMed
- Bourcier T et al. "Bacterial keratitis: predisposing factors, clinical and microbiological review of 300 cases." Br J Ophthalmol. 2003;87:834–838. PMID: 12812878
- Liesegang TJ. "Herpes simplex virus epidemiology and ocular importance." Cornea. 2001;20:1–13 — Search PubMed
- Gorscak JJ et al. "An outbreak of Fusarium keratitis associated with contact lens use in the northeastern United States." Ophthalmology. 2007;114:1328–1333 — Search PubMed
- Seal DV et al. "Acanthamoeba keratitis: a threat to contact lens wearers." Bull World Health Organ. 1992;70:173–179 — Search PubMed
- Austin A et al. "Review of 72 consecutive cases of Acanthamoeba keratitis, 1992–1996." Br J Ophthalmol. 1998;82:1121–1124 — Search PubMed
- Srinivasan M et al. "The Steroids for Corneal Ulcers Trial (SCUT): secondary outcomes at 3 months." Arch Ophthalmol. 2012;130:143–150 — Search PubMed
- Lalitha P et al. "A randomized trial of voriconazole versus natamycin for Fusarium and Aspergillus keratitis." Ophthalmology. 2015;122:1486–1492 — Search PubMed
- Khor WB et al. "Fusarium keratitis in Singapore: a reemergence following the global contact lens-associated fungal keratitis outbreak of 2005–2006." Ophthalmology. 2012;119:260–265 — Search PubMed
- Stapleton F et al. "The incidence of contact lens-related microbial keratitis in Australia." Ophthalmology. 2008;115:1655–1662 — Search PubMed
- Dart JK et al. "Risk factors for microbial keratitis with contemporary contact lenses: a case-control study." Ophthalmology. 2008;115:1647–1654. PMID: 18538404
PubMed topic searches:
- Corneal ulcer bacterial keratitis treatment
- Acanthamoeba keratitis contact lens
- Herpes simplex keratitis recurrence prevention
- Fungal keratitis natamycin voriconazole
Connections
- Ophthalmology
- Conjunctivitis
- Uveitis
- Dry Eye Disease
- Keratoconus
- Optic Neuritis
- Orbital Cellulitis
- Diseases