Cirrhosis: History and Discovery
The hard, shrunken liver and the swollen belly that so often accompanied it were observed for more than two thousand years before anyone understood what tied them together. Physicians in antiquity could feel the firm liver and tap the fluid-filled abdomen; eighteenth-century anatomists, dissecting the dead, finally described the diseased organ in careful detail. The name we still use was given by one man — René Théophile Hyacinthe Laennec, the French physician who also invented the stethoscope — who in 1819 coined cirrhosis from the Greek kirrhos, “tawny,” for the orange-yellow colour of the scarred liver he saw at autopsy. This page traces that long arc: from Hippocrates’ hard livers, through Morgagni’s 1761 dissections and Laennec’s naming, to the modern recognition that alcohol, viral hepatitis, and fibrosis drive the end-stage scarring common to nearly every chronic liver disease.
Table of Contents
- Antiquity: Hard Livers and “Dropsy”
- Morgagni and the Birth of Pathology (1761)
- Laennec Names “Cirrhosis” (1819)
- From Kirrhos to “Laennec’s Cirrhosis”
- Portal Hypertension and Its Complications
- Understanding Fibrosis: The Scar-Making Cell
- Viral Hepatitis: Blumberg, Houghton, and the Nobel Discoveries
- Cirrhosis as a Common End-Stage
- Legacy and Modern Understanding
- Research Papers and References
- Connections
- Featured Videos
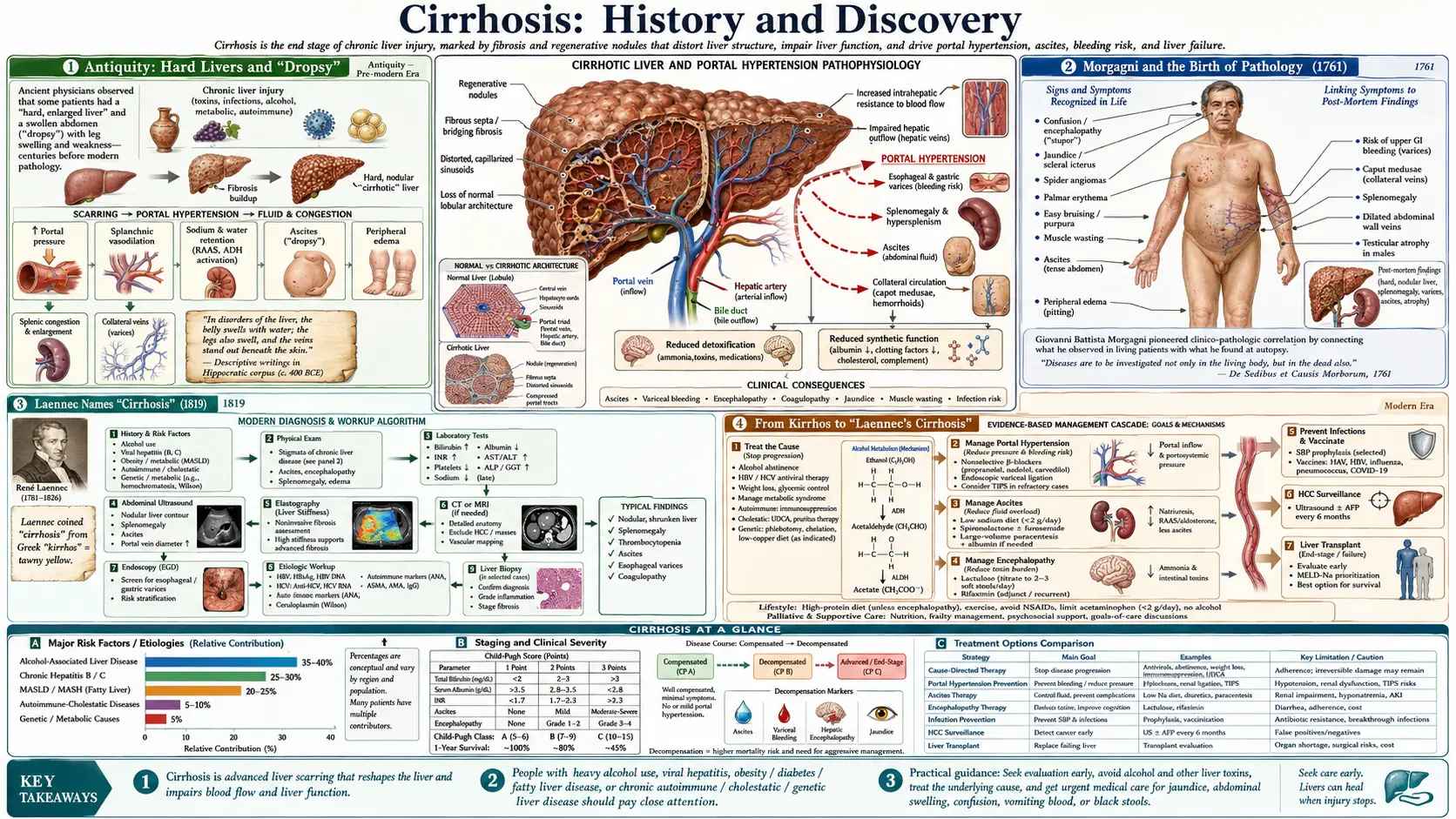
Antiquity: Hard Livers and “Dropsy”
Long before the liver’s functions were understood, physicians of the ancient Mediterranean could feel that something had gone badly wrong with it. The Hippocratic writers of fifth- and fourth-century BCE Greece — the texts attributed to Hippocrates of Cos (c. 460–370 BCE) and his school — described patients whose livers were abnormally hard on palpation and who developed hydrops (generalized swelling) and, in particular, abdominal swelling with fluid. The Greek term for that fluid-filled belly, askites, derives from askós, a leather wine-bag or sheepskin — an apt image for a taut, distended abdomen. The word survives today as ascites, still one of the defining complications of advanced cirrhosis.
The Hippocratic Corpus is also among the earliest medical literature to describe jaundice (icterus) in detail — its forms, its prognosis, and its association in some cases with delirium — and to discuss dropsy of the abdomen and its grave outlook. The Hippocratic physicians even practised abdominal paracentesis (tapping the belly to drain fluid), while cautioning against draining too much too quickly, a caution that modern hepatology echoes. What the ancients could not do was connect these signs to a single underlying organ disease: they observed the hard liver, the yellow skin, and the swollen abdomen as separate phenomena within their humoral framework, not yet as the linked consequences of one scarring process.
These antique observations are named here as historical primary sources rather than as modern citations. Their importance is that the clinical picture of end-stage liver disease — firm liver, jaundice, ascites — was recognized and recorded at the very dawn of Western medicine, even though its cause and its unity would remain mysterious for more than two millennia.
Morgagni and the Birth of Pathology (1761)
The decisive shift from describing symptoms in the living to explaining them from the dead came in 1761, when the Italian anatomist Giovanni Battista Morgagni (1682–1771), professor at Padua, published his monumental De Sedibus et Causis Morborum per Anatomen Indagatis (“On the Seats and Causes of Diseases Investigated by Anatomy”). The work systematically correlated patients’ symptoms during life with the lesions found in their bodies after death, drawing on records of roughly 640 dissections. It is widely regarded as the founding text of anatomical (morbid) pathology as a discipline, and it earned Morgagni the lasting title “the father of modern pathology.”
Within that vast catalogue, Morgagni is credited with some of the first systematic descriptions of the hardened, scarred liver we now call cirrhotic — the firm, shrunken, nodular organ found at autopsy in patients who had suffered jaundice and dropsy. By placing the diseased liver at the centre of the clinical story, he supplied the anatomical foundation that earlier symptom-based medicine had lacked. He did not, however, give the condition the name it bears today; the descriptions were of the pathology, set within his larger anatomical survey.
Morgagni’s method — insisting that disease has a seat (a specific organ or tissue) and a cause that careful dissection can reveal — reframed how physicians thought about chronic illness. For liver disease specifically, it meant that the hard liver of the ancients was no longer an isolated finding but the visible lesion of a definable organ disease. The stage was set for a name.
Laennec Names “Cirrhosis” (1819)
That name arrived in 1819, from the pen of the French physician René Théophile Hyacinthe Laennec (1781–1826) — the same Laennec who, only a few years earlier, had invented the stethoscope and effectively founded the practice of chest auscultation. In his landmark treatise on listening to the body, De l’auscultation médiate (1819), Laennec introduced the word cirrhosis — notably in a brief footnote rather than in a major chapter. He coined it from the Greek kirrhos (κιρρóς), meaning “tawny” or orange-yellow, to capture the colour of the shrunken, nodular liver he observed at autopsy.
It is worth being precise about what Laennec did and did not do, because accuracy matters here. He did not discover the disease, nor was he the first to describe its pathology — the hard liver had been recognized in antiquity, and the hepatic lesion had been noted in England and elsewhere well before 1819, with Morgagni’s descriptions predating him by decades. Laennec’s specific and enduring contribution was nomenclature: he gave the condition a single, vivid, descriptive name rooted in the organ’s appearance. That word — cirrhosis — proved so apt that it displaced the older, looser language of “hardened liver” and “scirrhus” and remains the standard medical term two centuries later.
Laennec’s choice reflected a distinctly nineteenth-century sensibility: name the disease for what the eye sees on the dissecting table. The tawny colour he described comes in part from fat and bile pigments in the diseased, regenerating liver tissue. In choosing kirrhos, Laennec fused the new anatomical pathology of Morgagni’s generation with the classical Greek vocabulary that still furnished medicine its technical terms.
From Kirrhos to “Laennec’s Cirrhosis”
Over the nineteenth and twentieth centuries, the classic form of the disease — the micronodular cirrhosis associated with chronic heavy alcohol use, in which the liver is studded with small, uniform nodules separated by fibrous bands — came to be called “Laennec’s cirrhosis” in his honour. The eponym is still encountered today, most often as a synonym for alcohol-related cirrhosis.
There is a historical irony in the term, well documented in the medical-history literature: the eponym “Laennec’s cirrhosis” became widespread in North America — carried largely by the enormous influence of William Osler’s textbook of medicine — yet remained comparatively rare in France itself, even though it honours a French physician. The name thus says as much about how medical eponyms spread through influential textbooks as it does about Laennec’s original footnote.
Modern hepatology has largely moved toward classifying cirrhosis by cause (alcohol-related, viral, metabolic/fatty-liver, autoimmune, biliary, and so on) and by nodule pattern (micronodular versus macronodular) rather than by eponym. But “Laennec’s cirrhosis” endures as a respectful nod to the man who named the condition and, in the same era, taught physicians how to listen to the living chest.
Portal Hypertension and Its Complications
Naming the diseased liver was one thing; explaining why it killed was another. Much of the danger of cirrhosis comes not from the liver’s loss of function alone but from portal hypertension — the dangerous rise in blood pressure within the portal venous system that drains the gut to the liver, caused when scarring obstructs blood flow through the hardened organ. As pressure backs up, blood is forced through fragile collateral channels, producing the swollen veins of the oesophagus and stomach (varices) that can rupture and bleed catastrophically, and contributing to the ascites the ancients had observed.
The term “portal hypertension” was introduced in 1902 by the French physicians Augustin Gilbert and Carnot, who, describing the clinical features of cirrhosis, proposed that the disease raised pressure in the portal system and thereby opened the collateral connections — including the oesophageal veins — between the portal and systemic circulations. This was, in its original framing, a hypothesis about mechanism, and it is fair to present it as such; subsequent measurement and imaging across the twentieth century confirmed and refined the concept and made portal-pressure assessment central to managing the disease.
Linking cirrhosis to portal hypertension transformed it from a static autopsy finding into a dynamic, understandable, and partly treatable circulatory problem. It explained the bleeding varices, much of the ascites, and the splenic enlargement seen in advanced disease, and it pointed the way toward the shunt operations and, later, the endoscopic and pharmacological treatments used today to lower portal pressure and prevent haemorrhage.
Understanding Fibrosis: The Scar-Making Cell
The deepest layer of understanding came with the cellular biology of fibrosis — the scarring process that is cirrhosis at the microscopic level. Cirrhosis is, in essence, the liver’s end-stage scar: excessive deposition of fibrous connective tissue that walls off regenerating nodules and chokes the organ’s normal architecture. Identifying which cell lays down that scar took more than a century of patient microscopy.
The trail begins in 1876, when the German anatomist Karl Wilhelm von Kupffer stained the liver with a gold-chloride method and described star-shaped cells in the hepatic lobules, which he named Sternzellen (“stellate cells”). Their function stayed mysterious for decades. In the twentieth century, Toshio Ito described fat- and vitamin-A–storing cells in the perisinusoidal space, and in 1971 Kenjiro Wake demonstrated that von Kupffer’s Sternzellen and Ito’s fat-storing cells were one and the same cell — the hepatic stellate cell — and confirmed its role as the liver’s main store of vitamin A. (The phagocytic “Kupffer cells” that also bear von Kupffer’s name are a separate population; the historical disentangling of these cell types is itself part of the story.)
The pathological punchline followed when investigators including Kent and Popper showed that these stellate cells are intimately linked to the genesis of hepatic fibrosis: on injury they transform from quiescent vitamin-A stores into activated, scar-secreting myofibroblasts that pour out collagen. That insight — that a single, identifiable cell drives the scarring — reframed cirrhosis as a potentially modifiable process and made the hepatic stellate cell the principal target of modern anti-fibrotic drug research. It also clarified a crucial clinical point: caught early, liver fibrosis can regress when its cause is removed, whereas established cirrhosis is far harder to reverse.
Viral Hepatitis: Blumberg, Houghton, and the Nobel Discoveries
For most of history, the great recognized cause of cirrhosis was alcohol. But a large share of the world’s cirrhosis — and of the liver cancer that follows it — comes from chronic viral hepatitis, and identifying those viruses was a twentieth-century triumph crowned by two Nobel Prizes.
The first breakthrough was the hepatitis B virus. In 1965, the American physician-scientist Baruch Samuel Blumberg and colleagues detected a novel serum antigen in an Australian Aboriginal donor — the famous “Australia antigen” — which was soon shown to be a surface component of the hepatitis B virus (today’s hepatitis B surface antigen). Blumberg’s work opened the way to a blood test and ultimately a vaccine, and he shared the 1976 Nobel Prize in Physiology or Medicine (with D. Carleton Gajdusek) for new insights into the origin and spread of infectious diseases. Chronic hepatitis B is a leading global cause of cirrhosis and primary liver cancer.
The second breakthrough was the hepatitis C virus, the agent long known only as the cause of mysterious “non-A, non-B” post-transfusion hepatitis. In 1989, working at the biotechnology company Chiron, Michael Houghton and colleagues cloned and identified the virus’s genome; Harvey J. Alter had earlier shown that an unknown blood-borne agent caused much chronic hepatitis, and Charles M. Rice later engineered a working laboratory strain that proved the virus alone could cause liver disease. The three shared the 2020 Nobel Prize in Physiology or Medicine for the discovery of hepatitis C virus. Because chronic hepatitis C silently scars the liver over years, its identification — and the curative antiviral drugs that followed — has had a direct, large-scale impact on preventing cirrhosis.
Cirrhosis as a Common End-Stage
One of the most important modern understandings is conceptual rather than tied to a single discovery: cirrhosis is not one disease but a common end-stage — the final, shared scarring pattern that many different chronic liver diseases converge upon. The liver has a limited repertoire of responses to long-term injury, and sustained damage from almost any cause tends to end in the same hard, nodular, fibrotic organ Laennec named.
The roster of causes is broad and has grown over time. Chronic alcohol use remains the classic cause behind “Laennec’s cirrhosis.” Chronic viral hepatitis B and C account for a vast share worldwide. Metabolic dysfunction–associated fatty liver disease (long called non-alcoholic fatty liver disease, NAFLD/NASH) has risen with obesity and type 2 diabetes to become a major and growing cause. Additional causes include autoimmune hepatitis, the biliary diseases (primary biliary cholangitis and primary sclerosing cholangitis), and inherited disorders of metal handling — iron overload (haemochromatosis) and copper accumulation (Wilson’s disease) — among others.
This “many roads, one destination” framing matters clinically because it shifts attention upstream: preventing or treating the underlying cause — abstaining from alcohol, curing hepatitis C, controlling metabolic disease, removing excess iron or copper — is what halts or even reverses fibrosis before it becomes irreversible cirrhosis. The history of cirrhosis is, in this sense, the history of learning to identify and address each of the separate diseases that all end at the same scarred liver.
Legacy and Modern Understanding
The story that runs from a Hippocratic physician’s hand pressed on a hard liver to a modern laboratory dissecting the hepatic stellate cell is one of steadily deepening explanation. Antiquity gave the clinical picture — firm liver, jaundice, dropsy. Morgagni gave the pathology, anchoring the disease in a dissectible organ. Laennec gave the name, cirrhosis, for the tawny scarred liver he saw at autopsy. The twentieth century gave the mechanisms: portal hypertension to explain the bleeding and the fluid, fibrosis biology to explain the scar, and virology to explain a major share of the cause.
Two through-lines deserve emphasis for anyone reading this as a patient or carer rather than a historian. First, cirrhosis is the end-stage of many distinct diseases, which means the most powerful action is almost always to find and treat the underlying cause early — before scarring becomes permanent. Second, the field has moved from passive description toward genuine prevention and treatment: vaccines and tests for hepatitis B, curative drugs for hepatitis C, treatments to lower portal pressure and manage varices and ascites, and an active search for anti-fibrotic therapies aimed squarely at the scar-making cell.
Laennec’s two-hundred-year-old footnote thus opens onto a living, fast-moving science. The detailed clinical picture of the disease — its symptoms, complications, diagnosis, and management — is covered in the main Cirrhosis article, while related conditions that lead to or overlap with cirrhosis are explored in the companion pages linked in the Connections section below.
Research Papers and References
The references below combine peer-reviewed historical and review articles with curated PubMed topic-search links into the history-of-medicine literature on cirrhosis, liver pathology, portal hypertension, hepatic fibrosis, and the discovery of the hepatitis viruses. Historical primary texts — the Hippocratic Corpus, Morgagni’s De Sedibus (1761), and Laennec’s De l’auscultation médiate (1819) — are named in the article as historical sources rather than as modern citations. External links open in a new tab.
- Roguin A. Rene Theophile Hyacinthe Laënnec (1781–1826): the man behind the stethoscope. Clinical Medicine & Research. 2006;4(3):230–235. — doi:10.3121/cmr.4.3.230
- Duffin JM. Why does cirrhosis belong to Laennec? Canadian Medical Association Journal. 1987;137(5):393–396. (Laennec coined “cirrhosis” from Greek kirrhos, tawny, in a footnote to his 1819 treatise.) — PubMed: PMID 3304599
- Laennec’s cirrhosis (historical perspective). The Lancet. — doi:10.1016/S0140-6736(18)32523-6
- Morgagni GB. De Sedibus et Causis Morborum per Anatomen Indagatis (1761) — the founding of anatomical pathology and early descriptions of hepatic cirrhosis. — PubMed: Morgagni De Sedibus history
- Liver fibrosis: our evolving understanding (review covering Morgagni, stellate cells, and the cellular basis of cirrhosis). — PMC: Liver fibrosis — evolving understanding
- The 2020 Nobel Prize in Medicine for the discovery of hepatitis C virus (Alter, Houghton, Rice). — PMC: Discovery of hepatitis C virus — 2020 Nobel Prize
- The Nobel Prize in Physiology or Medicine 1976 — Baruch S. Blumberg and the Australia antigen / hepatitis B virus. — NobelPrize.org: Blumberg 1976
- Balducci G, et al. A short history of portal hypertension and of its management (Gilbert & Carnot, 1902). Journal of Gastroenterology and Hepatology. 2016;31(3):541–545. — doi:10.1111/jgh.13200
- Wong F. Historical aspects of ascites and the hepatorenal syndrome (Hippocrates, dropsy, paracentesis). Clinical Liver Disease. 2021. — doi:10.1002/cld.1090
- Karl Wilhelm von Kupffer and his contributions to modern hepatology (1876 Sternzellen / stellate cells). — PMC: von Kupffer and modern hepatology
- Hepatic stellate cells: history, biology, and role in fibrosis (von Kupffer, Ito, Wake 1971, Kent & Popper). — PubMed: hepatic stellate cell history fibrosis
- Jaundice and liver disease in the Hippocratic Corpus — descriptions in antiquity. — PubMed: jaundice in the Hippocratic Corpus
- History of cirrhosis — nomenclature, pathology, and concept of a common end-stage. — PubMed: cirrhosis history Laennec pathology
- Discovery and history of the hepatitis B virus and Australia antigen. — PubMed: hepatitis B Australia antigen Blumberg history
External Authoritative Resources
- NobelPrize.org — 2020 Prize: Discovery of Hepatitis C Virus
- NIDDK (NIH) — Cirrhosis
- PubMed — All research on the history of cirrhosis
Connections
- Nephrology & Hepatology
- Cirrhosis (main article)
- Liver Disease
- Non-Alcoholic Fatty Liver Disease
- Hepatitis
- Hepatitis B
- Hepatitis C
- All Conditions