Melioidosis
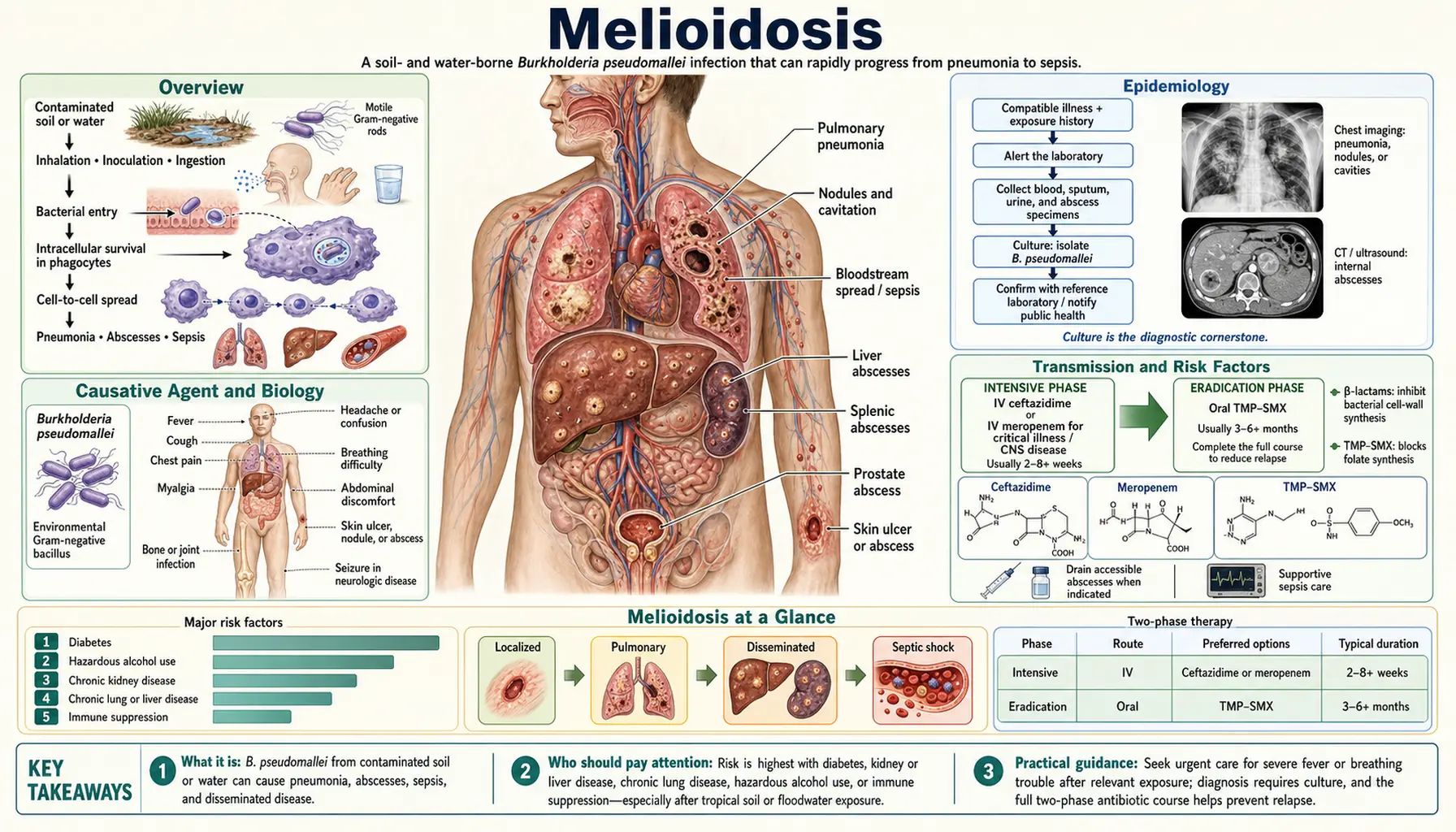
Table of Contents
- Overview
- Causative Agent and Biology
- Epidemiology
- Transmission and Risk Factors
- Clinical Manifestations
- Incubation and Latency
- Bioterrorism Potential
- Diagnosis
- Treatment
- Prevention and Prognosis
- References
- Connections
- Featured Videos
Overview
Melioidosis is a serious bacterial infection caused by Burkholderia pseudomallei, a gram-negative bacillus that lives in soil and water in tropical and subtropical regions. It is sometimes called "the great mimicker" because its clinical presentations range from a localized skin ulcer to overwhelming septicemia, and it can look like tuberculosis, typhoid fever, or pneumonia on first presentation.
Global mortality is approximately 89,000 deaths per year — comparable to measles — yet the disease remains largely unknown outside endemic regions because it is chronically underreported and misdiagnosed. Diagnostic cultures and clinical awareness are lacking across most of the high-burden settings in South and Southeast Asia, meaning many cases are recorded as "culture-negative sepsis" and never confirmed.
The name comes from the Greek words for "resembling glanders" — glanders being another bacterial disease historically associated with horses and mules. B. pseudomallei and glanders (B. mallei) are closely related, though melioidosis is primarily a soil-borne environmental infection rather than an animal-contact disease.
Causative Agent and Biology
Burkholderia pseudomallei is a motile, aerobic, gram-negative rod. It is an environmental saprophyte naturally found in moist soil and stagnant surface water in endemic regions, particularly at depths of 10–30 cm in rice paddies and agricultural soils. It thrives in the wet season and can survive in soil for months to years under the right conditions.
One of the most clinically important characteristics of B. pseudomallei is its intrinsic resistance to many commonly used antibiotics. It is naturally resistant to:
- Penicillin G and ampicillin
- First and second generation cephalosporins (cephalexin, cefazolin, cefuroxime)
- Macrolides (azithromycin, clarithromycin)
- Aminoglycosides (gentamicin, tobramycin)
- Colistin
This resistance is chromosomally encoded via efflux pumps and beta-lactamases and cannot be overcome by combination or dose escalation. Empirical antibiotic regimens that cover most gram-negative sepsis will fail against melioidosis — which is a major reason why unrecognized melioidosis in endemic regions carries such high mortality.
Because of its high virulence, environmental stability, and aerosol infectivity, B. pseudomallei is classified as a CDC Category B select agent and a potential bioterrorism threat. Laboratory workers must handle it under Biosafety Level 3 (BSL-3) conditions. If you suspect melioidosis, always notify your microbiology lab before sending specimens so they can take appropriate precautions.
Epidemiology
Melioidosis is endemic across a wide tropical belt. The regions with the highest recognized burden include:
- Northern Australia — particularly the Top End of the Northern Territory and the Darwin region. Approximately 50 cases per year occur in a relatively small population, with a high case-fatality rate even with access to intensive care.
- Southeast Asia — Thailand (northeastern Thailand has the highest prevalence in the country), Malaysia, Vietnam, Singapore, Cambodia, Laos, and Myanmar are all endemic. Thailand's Khon Kaen region has among the highest documented incidence globally.
- South Asia — India is increasingly recognized as carrying a very large burden, particularly in Odisha/Orissa state and Tamil Nadu. A 2016 modelling study estimated that India alone accounts for nearly 45% of the global disease burden — a figure that was shocking to the international infectious disease community and reflects decades of underdiagnosis.
- Sub-Saharan Africa — cases are being recognized with increasing frequency. Many past cases were likely recorded as culture-negative sepsis due to absence of adequate laboratory infrastructure.
- The Americas — Brazil, Ecuador, Mexico, and parts of the Caribbean have documented endemic transmission, historically considered non-endemic but now clearly established.
A striking seasonal pattern exists: cases peak dramatically during the monsoon and wet season. Heavy rainfall disrupts soil, creates aerosols carrying bacteria, floods rice paddies, and brings agricultural workers into closer contact with contaminated soil and standing water.
The global burden has been systematically underestimated. A landmark 2016 modelling study published in Nature Microbiology estimated 165,000 cases and 89,000 deaths per year worldwide — placing melioidosis in the same mortality league as measles, yet with a fraction of the public health attention or research funding.
Transmission and Risk Factors
Melioidosis is not transmitted from person to person. All infections originate from environmental exposure. Three main routes have been established:
- Inhalation of aerosols from contaminated soil and water. This is especially common during heavy monsoon rainstorms, typhoon or cyclone events, and agricultural activities generating dust from contaminated soil. This route tends to cause primary pneumonia and is the most common route in Australia.
- Skin inoculation through cuts, abrasions, or skin trauma during contact with contaminated soil or water. This is the most common route in rice paddy workers and other agricultural laborers who work barefoot or with exposed skin.
- Ingestion of contaminated water or food. Less common but documented, particularly in outbreak settings associated with contaminated water supplies.
The most important risk factors — in rough order of clinical impact:
- Diabetes mellitus — the single most powerful risk factor, present in 40–60% of all melioidosis cases. Diabetes impairs neutrophil chemotaxis, phagocytic killing, and oxidative burst, allowing B. pseudomallei to evade immune clearance. Diabetic patients who acquire melioidosis have markedly higher mortality than non-diabetic patients.
- Chronic kidney disease — impairs immune response and commonly co-exists with diabetes in endemic populations.
- Alcoholism — causes immune suppression, nutritional deficiencies, and increases aspiration risk (relevant for pulmonary melioidosis).
- Thalassemia — very common in Southeast Asia; the mechanism appears to involve altered macrophage function and iron dysregulation.
- Immunosuppression — corticosteroids, TNF-alpha inhibitors (used for rheumatoid arthritis, inflammatory bowel disease), advanced HIV, and solid organ transplant recipients are all at elevated risk.
- Occupational exposure — farmers, rice paddy workers, and military personnel training in endemic areas are disproportionately affected.
Healthy, immunocompetent individuals can also be infected, particularly through intense aerosol exposure such as typhoons or military helicopter operations over contaminated terrain. However, severe disease is far more common in people with the risk factors listed above.
Clinical Manifestations
Melioidosis earns the title "the great mimicker" because no single presentation is pathognomonic. The disease can affect virtually any organ system, and its presentation overlaps with tuberculosis, typhoid fever, staphylococcal septicemia, and many other conditions.
Pulmonary Melioidosis
The most common form, accounting for 50–60% of cases. Severity ranges from mild pneumonia to life-threatening acute respiratory distress syndrome (ARDS). Upper lobe involvement with cavitation is characteristic and strongly mimics pulmonary tuberculosis — including on chest X-ray and CT scan, where consolidation, cavitation, and nodules are indistinguishable from TB. Any patient from an endemic region presenting with "TB-like" pneumonia that does not respond to standard antibiotics, or whose TB cultures are negative, should have melioidosis strongly considered.
Septicemia
Bacteremia with metastatic seeding to multiple organs. Without appropriate antibiotic therapy, septicemic melioidosis is nearly universally fatal. Even with treatment, mortality in resource-limited settings can exceed 50%. Features include high fever, rigors, and rapid clinical deterioration to septic shock and multi-organ failure.
Localized Infection
Skin and soft tissue infection presents as ulcers, cellulitis, or abscesses — often minimally tender or painless, which can mislead clinicians. Regional lymphadenopathy is common. A particularly characteristic presentation is parotid gland abscess in children in northeastern Thailand, where melioidosis is the most common cause of this finding.
Neurological Melioidosis
Brain abscess and, uniquely, a flaccid paraplegia or limb weakness caused by brainstem and spinal cord involvement. This predilection for the brainstem and spinal cord is unusual among bacterial pathogens and, when present, is highly suggestive of melioidosis in an endemic setting. Neurological melioidosis carries high mortality and significant long-term neurological disability in survivors.
Genitourinary Involvement
Prostatic abscess is recognized in 20–30% of melioidosis cases in Australia and is often the presenting manifestation, causing urinary retention or recurrent urinary tract infections. It must be identified by digital rectal examination, CT, or MRI and drained surgically or under imaging guidance — antibiotic therapy alone will not cure a walled-off abscess.
Septic Arthritis and Osteomyelitis
Bone and joint infection can occur as a metastatic focus during bacteremia. Long bones and vertebrae may be involved. Treatment requires both prolonged antibiotic therapy and often surgical debridement.
Relapse
Without completion of the full eradication phase of treatment (see Treatment section), relapse occurs in approximately 50% of patients within 12 months. Relapse may present as a different clinical form from the original infection — a patient whose primary illness was pneumonia may relapse with skin abscess or septicemia.
Incubation and Latency
The typical incubation period after exposure is 2 to 28 days, though most symptomatic cases present within 1–3 weeks. However, one of the most remarkable and clinically important features of melioidosis is its capacity for prolonged latency.
Burkholderia pseudomallei can remain dormant in host tissue — particularly the lungs and lymph nodes — for months to decades. The best-documented examples come from military veterans: US, UK, and Australian soldiers who served in Southeast Asia during the Vietnam War era (1960s–1980s) developed reactivation melioidosis up to 40 years after leaving endemic regions. Reactivation is typically triggered by a new immunosuppressive event — the onset of diabetes, initiation of corticosteroid therapy, cancer chemotherapy, or another serious illness.
The practical implication for clinicians everywhere: when evaluating unexplained sepsis, pneumonia, or abscess in any patient who spent time in an endemic region — even decades ago — melioidosis must remain on the differential diagnosis. A complete travel and military service history going back to childhood is always relevant.
Bioterrorism Potential
Burkholderia pseudomallei is classified as a CDC Category B biological agent, meaning it is considered a credible potential bioterrorism threat. The characteristics that make it a concern include:
- High virulence and a low infectious dose via the aerosol route
- Intrinsic resistance to many common antibiotics, limiting treatment options in a mass-casualty scenario
- Aerosol dispersal could cause an outbreak of severe pneumonia in a non-immune population with no prior exposure
- No licensed vaccine exists
- Historical evidence of weaponization research by the former Soviet bioweapons program
- Environmental stability — it can survive in soil for extended periods
The clinical implication is that infectious disease clinicians and public health authorities should suspect melioidosis in any unexplained cluster of severe pneumonia cases in a non-endemic region, particularly in the context of a recent mass gathering, conflict zone, natural disaster, or unusual environmental event. Any cluster of culture-positive B. pseudomallei outside the recognized endemic belt should trigger immediate notification of public health authorities.
Diagnosis
Diagnosis requires a high index of suspicion — the first step is simply thinking of melioidosis in the right clinical context. Ask about residence in or travel to endemic regions, occupational soil or water exposure, and underlying risk factors such as diabetes.
Culture (Gold Standard)
Culture remains the definitive diagnostic method. Collect blood cultures, sputum, urine, and swabs or aspirates from any accessible wound, ulcer, or abscess. B. pseudomallei grows on standard bacteriology media (blood agar, MacConkey agar) within 48–72 hours. Colonial morphology is characteristic: colonies are wrinkled with a metallic sheen, though they may appear smooth initially and develop the wrinkled appearance over 3–4 days of incubation. Ashdown's selective medium (containing gentamicin and crystal violet) improves sensitivity for non-sterile sites such as sputum and wound swabs.
Critical safety notice: Always notify the microbiology laboratory when melioidosis is suspected before sending specimens. B. pseudomallei is a BSL-3 pathogen, and processing it with standard open-bench techniques creates an aerosol hazard for laboratory personnel. This is a real-world risk — laboratory-acquired melioidosis infections have been documented in facilities that were not warned.
Rapid Diagnostics
- Lateral flow assay (LFA): A point-of-care antigen detection test that can be performed at the bedside or in resource-limited settings. Sensitivity is approximately 80% in bacteremic patients. It has been validated in Thailand and is increasingly deployed in endemic regions where culture infrastructure is limited.
- PCR: Highly sensitive in blood during active septicemia. Increasingly available in reference laboratories and hospital systems in high-income countries. Particularly useful for rapid confirmation when the LFA is positive or when clinical suspicion is very high.
Serology
The indirect hemagglutination (IHA) antibody test is widely used, particularly in Thailand. However, its utility is limited by high background seropositivity in endemic populations — up to 30–40% of healthy adults in northeastern Thailand have detectable antibodies from subclinical past exposure. A single high titer or a fourfold rise in paired samples is more informative. Serology is most useful in travelers and immigrants from non-endemic regions presenting with unexplained illness, where background seropositivity is zero.
Imaging
- Chest X-ray and CT: Look for upper lobe cavitation, nodules, and consolidation — patterns that mimic tuberculosis.
- CT of the abdomen and pelvis: Essential to detect splenic microabscesses, prostatic abscess, hepatic abscesses, and lymphadenopathy — findings that guide drainage decisions.
- MRI of the brain and spine: Required when neurological signs or symptoms suggest CNS involvement. Characteristically shows brainstem and spinal cord lesions in neurological melioidosis.
Treatment
Treatment of melioidosis is divided into two essential phases. Cutting either phase short — or skipping the eradication phase entirely — leads to relapse in approximately half of patients. The two-phase approach is non-negotiable.
Phase 1: Intensive (Intravenous) Phase
Duration: minimum 10–14 days for uncomplicated pulmonary disease; extended to 4–8 weeks for CNS infection, osteomyelitis, prostatic abscess, or deeply seated infection.
- Ceftazidime 2g IV every 6–8 hours — first-line agent. A third-generation cephalosporin with reliable activity against B. pseudomallei. The pivotal 1989 Lancet trial (White et al.) demonstrated that switching from co-trimoxazole-based regimens to ceftazidime halved mortality in severe melioidosis — one of the most impactful clinical trials in tropical infectious disease.
- Meropenem 1g IV every 8 hours — preferred over ceftazidime for CNS melioidosis (better blood-brain barrier penetration), critically ill patients in septic shock, and confirmed ceftazidime treatment failure. Imipenem is an alternative carbapenem but inferior to meropenem for CNS penetration.
Phase 2: Eradication (Oral) Phase
This is the phase most commonly abbreviated or abandoned — and the most common cause of relapse. Oral therapy must continue for 3 months (uncomplicated disease) or 6 months (bone, CNS, or prostatic involvement).
- Trimethoprim-sulfamethoxazole (TMP-SMX / co-trimoxazole): 8/40 mg/kg/day in two divided doses. Standard adult dosing is two double-strength tablets (each 800mg/160mg) twice daily. Monitor CBC and electrolytes monthly — TMP-SMX can cause rash, bone marrow suppression, and hyperkalemia, particularly in patients with underlying kidney disease.
- Amoxicillin-clavulanate 875/125mg twice daily can be added alongside TMP-SMX. This combination is particularly important in pregnancy, where TMP-SMX is contraindicated in the first trimester and near term due to teratogenicity and neonatal risks.
Antibiotics to Avoid
The following antibiotics are ineffective against B. pseudomallei due to intrinsic resistance and should never be used as primary therapy:
- Penicillin G, ampicillin, amoxicillin alone
- First and second generation cephalosporins: cephalexin, cefazolin, cefuroxime
- Macrolides: azithromycin, clarithromycin
- Aminoglycosides: gentamicin, tobramycin
- Colistin
This is why unrecognized melioidosis so often leads to death in endemic regions — patients present with sepsis or pneumonia and are treated with penicillin-based or macrolide-based empirical regimens that are standard for bacterial pneumonia and sepsis worldwide but completely inactive against this pathogen.
Surgical Management
Drain all accessible abscesses: prostatic, parotid, splenic, and hepatic abscesses require either image-guided drainage or surgical drainage. Antibiotic therapy alone will not sterilize a walled-off abscess. Bone and joint infection (osteomyelitis, septic arthritis) often requires surgical debridement alongside prolonged antibiotics.
Prevention and Prognosis
Prevention
- No licensed vaccine is available. Vaccine development is an active research priority given the global burden and bioterrorism classification, but no candidate has completed phase 3 trials.
- Personal protective equipment: Agricultural and soil workers in endemic regions should wear footwear and protective gloves, particularly during the wet season. Avoiding barefoot work in rice paddies significantly reduces skin inoculation risk.
- Diabetes management: Optimizing blood glucose control in diabetic patients living in or traveling to endemic regions reduces both the risk of acquiring infection and the severity of disease if infection occurs.
- Chemoprophylaxis: No routine chemoprophylaxis is recommended for travelers. Doxycycline prophylaxis has been discussed for military personnel with extreme exposure scenarios but is not a standard recommendation and has limited evidence.
- Water safety: Avoiding consumption of untreated surface water in endemic areas reduces ingestion-route exposure.
Prognosis
Outcomes depend heavily on healthcare setting, speed of diagnosis, and underlying risk factors:
- Australia (optimized ICU care, rapid diagnosis): Overall case fatality rate of 10–20%.
- Thailand and most developing-world settings: Case fatality rate of 40–75%, primarily due to diagnostic delay, empirical antibiotics that are ineffective, and limited intensive care capacity.
- Septicemic melioidosis without ICU-level supportive care: Mortality exceeds 90%.
- CNS melioidosis: High mortality and significant permanent neurological disability in survivors even with appropriate therapy.
- Relapse: Approximately 50% of patients who do not complete the full eradication phase relapse within 12 months. Relapse is treatable — a full second course of intensive followed by eradication therapy is effective — but each episode of severe disease carries its own mortality risk, particularly in patients with diabetes or other comorbidities.
The most important prognostic intervention is early recognition: melioidosis diagnosed and treated promptly with appropriate intravenous antibiotics has far better outcomes than cases treated initially with ineffective agents and corrected only after culture results return days later.
References
- Limmathurotsakul D, et al. Predicted global distribution of Burkholderia pseudomallei and burden of melioidosis. Nat Microbiol. 2016;1:15008 — Search PubMed
- Wiersinga WJ, et al. Melioidosis. Nat Rev Dis Primers. 2018;4:17107 — Search PubMed
- Dance D. Treatment and prophylaxis of melioidosis. Int J Antimicrob Agents. 2014;43(4):310–8 — Search PubMed
- Pitman MC, et al. Intravenous therapy duration and outcomes in melioidosis: a new treatment paradigm. PLoS Negl Trop Dis. 2015;9(3):e0003586 — Search PubMed
- White NJ, et al. Halving of mortality of severe melioidosis by ceftazidime. Lancet. 1989;2(8665):697–701. PMID 2570956
- Cheng AC, Currie BJ. Melioidosis: epidemiology, pathophysiology, and management. Clin Microbiol Rev. 2005;18(2):383–416. PMID 15831829
- Currie BJ, et al. The epidemiology and clinical spectrum of melioidosis: 540 cases from the 20 year Darwin prospective study. PLoS Negl Trop Dis. 2010;4(11):e900. PMID 21152057
- Lipsitz R, et al. Workshop on treatment of and postexposure prophylaxis for Burkholderia pseudomallei and B. mallei infection, 2010. Emerg Infect Dis. 2012;18(12):e2 — Search PubMed
- Schweizer HP. Mechanisms of antibiotic resistance in Burkholderia pseudomallei: implications for treatment of melioidosis. Future Microbiol. 2012;7(12):1389–99 — Search PubMed
- Chierakul W, et al. Melioidosis in 6 travelers returning from Thailand. Clin Infect Dis. 2005;41(8):e76–9 — Search PubMed
- Currie BJ, Fisher DA, Howard DM, et al. Neurological melioidosis. Acta Trop. 2000;74(2–3):145–51 — Search PubMed
- Peacock SJ. Melioidosis. Curr Opin Infect Dis. 2006;19(5):421–8 — Search PubMed
Connections
- Infectious Disease
- Leptospirosis
- Strongyloidiasis
- Leishmaniasis
- Chagas Disease
- Tuberculosis
- Sepsis
- Type 2 Diabetes
- Lab Tests