Clostridium difficile (C. diff): History and Discovery
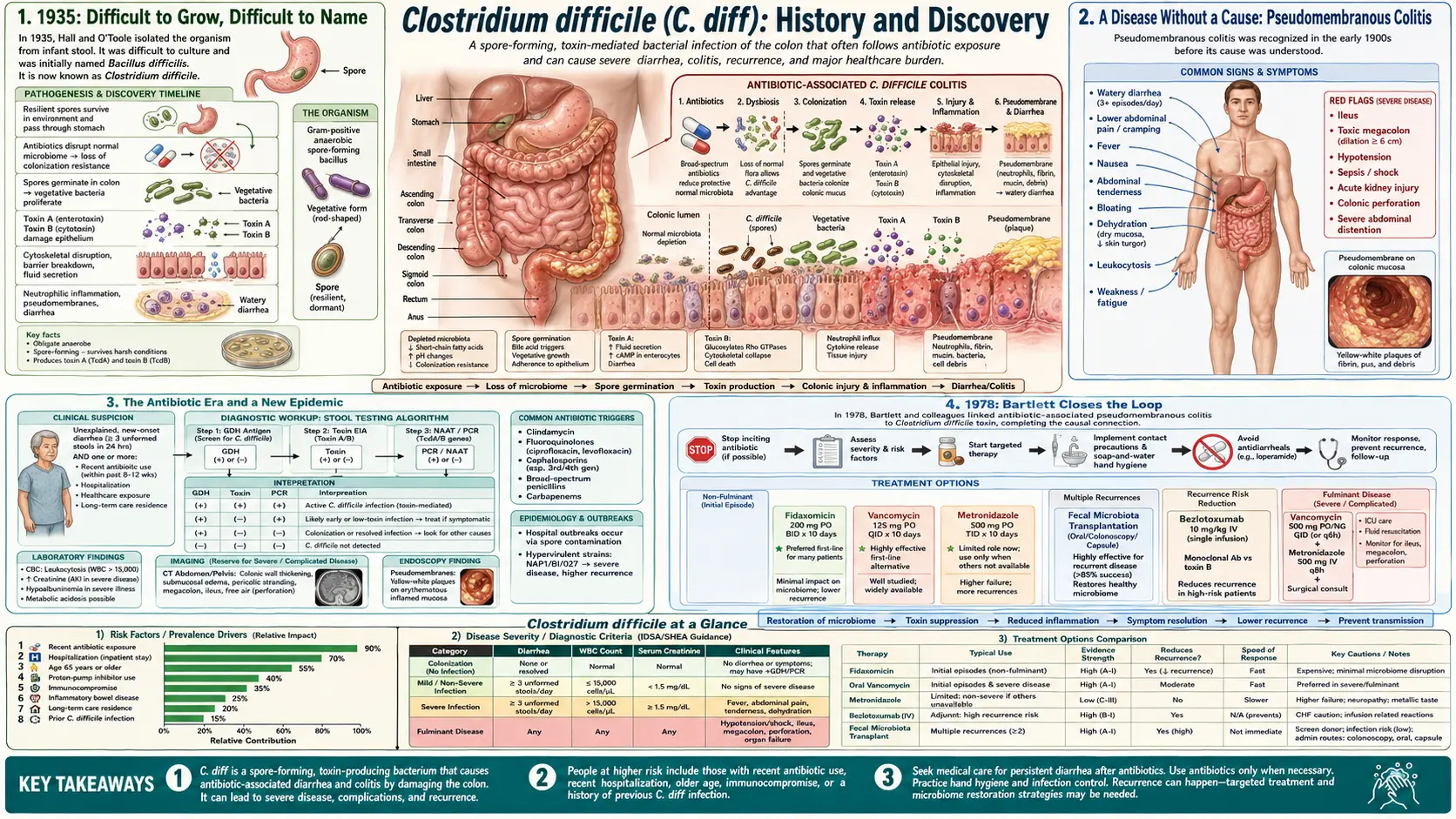
Clostridioides difficile (formerly Clostridium difficile, and almost universally called C. diff) is a spore-forming, toxin-producing bacterium that causes antibiotic-associated diarrhea and its most dangerous form, pseudomembranous colitis. Its history is unusually circuitous: the organism was first isolated in 1935 by Ivan C. Hall and Elizabeth O'Toole from the stool of perfectly healthy newborn babies — and named "Bacillus difficilis" precisely because it was so difficult to isolate and grow. For more than forty years it was regarded as a harmless intestinal curiosity. Not until 1978 did John G. Bartlett and colleagues prove that this same organism, through a toxin, was the cause of the deadly pseudomembranous colitis that antibiotics could trigger — a disease that had been described clinically as far back as 1893 but whose cause had remained a mystery. The modern chapters of the story are dramatic in their own right: the discovery of the two main toxins, the rise of the hypervirulent NAP1/027 epidemic strain in the 2000s, the recognition that disrupting the gut's own bacteria is what lets C. diff take hold, and the remarkable success of fecal microbiota transplantation (FMT) for stubborn, recurrent infection. The genus was formally renamed Clostridioides in 2016.
Table of Contents
- 1935: Difficult to Grow, Difficult to Name
- A Disease Without a Cause: Pseudomembranous Colitis
- The Antibiotic Era and a New Epidemic
- 1978: Bartlett Closes the Loop
- The Toxins: A and B
- The NAP1/027 Hypervirulent Strain
- Fecal Microbiota Transplantation
- 2016: From Clostridium to Clostridioides
- Legacy and Open Questions
- Research Papers and References
- Connections
- Featured Videos
1935: Difficult to Grow, Difficult to Name
The bacterium now feared on hospital wards worldwide was first met not in a sick patient but in the diapers of healthy infants. In 1935, the American microbiologists Ivan C. Hall and Elizabeth O'Toole published a study of the developing intestinal flora of normal, breast-fed newborns, following the day-by-day changes in the bacteria of their stools through the first ten days of life. Among the organisms they recovered was a previously undescribed strict anaerobe, which they proposed as a new species. Their paper, titled "Intestinal flora in new-born infants: with a description of a new pathogenic anaerobe, Bacillus difficilis," appeared in the American Journal of Diseases of Children.
The name they chose has become one of the most quietly honest in all of microbiology. The Latin difficilis means "difficult," and Hall and O'Toole used it because the organism was extraordinarily hard to isolate and slow to grow in pure culture — an oxygen-intolerant anaerobe that resisted the cultivation methods of the day. The genus name Bacillus was a placeholder reflecting its rod shape; the organism was later moved into the genus Clostridium by André Prévot in 1938, giving the familiar combination Clostridium difficile — with authority commonly written as "(Hall and O'Toole 1935) Prévot 1938."
Crucially, although Hall and O'Toole noted that the organism could produce a toxin lethal to laboratory animals, they found it in healthy babies and could not connect it to any human disease. For the next several decades it was filed away as an obscure, commonly carried member of the infant gut — a piece of normal anatomy rather than a pathogen. That mistaken sense of harmlessness is a recurring theme in the C. diff story, and it delayed recognition of the organism's true danger for more than a generation.
A Disease Without a Cause: Pseudomembranous Colitis
While the bacterium sat unrecognized in the laboratory, the disease it causes had already been described — under a different name and with no known cause. As early as 1893, the American surgeon J. M. T. Finney, working at Johns Hopkins Hospital under the famed physician William Osler, reported a fatal case of severe membrane-forming colitis following stomach surgery. Finney called it "diphtheritic colitis," borrowing the language of diphtheria because the inflamed bowel was coated with a tough, adherent membrane. This is generally credited as the first clinical description of what we now call pseudomembranous colitis.
The defining feature of the condition is visible to the naked eye and through the colonoscope: raised, yellowish-white plaques — the "pseudomembranes" — scattered over an inflamed colon, made of fibrin, mucus, dead cells, and inflammatory debris. Through the first half of the twentieth century, this dramatic and often fatal picture was seen sporadically, usually after surgery or serious illness, and its cause was genuinely unknown. For a time the prime suspect was Staphylococcus aureus, which was sometimes cultured from these patients, and so the disease was often blamed on a staph overgrowth of the bowel.
That this disease and Hall and O'Toole's difficult-to-grow infant bacterium were one and the same was not even suspected. The two strands of the story — a named-but-uncultured disease and a cultured-but-unexplained organism — would run in parallel for decades. What finally brought them together was an unintended consequence of one of medicine's greatest triumphs: the antibiotic.
The Antibiotic Era and a New Epidemic
With the widespread introduction of antibiotics from the 1940s onward, and especially of broad-spectrum agents in the 1950s, 1960s, and 1970s, clinicians began to notice a troubling new pattern: patients who had received antibiotics — sometimes for a trivial infection — could develop severe, watery, and occasionally pseudomembranous diarrhea. The phenomenon acquired the plain descriptive label antibiotic-associated colitis, and one antibiotic in particular became so notorious for triggering it that the condition was nicknamed "clindamycin colitis."
The paradox was striking: the very drugs that cured infection were causing a dangerous new bowel disease. Two leading hypotheses competed. The older idea blamed a staphylococcal overgrowth. The newer and ultimately correct intuition was that antibiotics, by wiping out the normal protective bacteria of the colon, allowed some other, resistant organism to flourish and do harm — an early articulation of what we now call disruption of the gut microbiome, or loss of "colonization resistance." The missing piece was the identity of that organism.
The decisive experimental breakthrough came from an animal model. Researchers found that giving clindamycin to hamsters reliably produced a fatal colitis that closely mirrored the human disease. This reproducible model — advanced especially in the United States by John G. Bartlett, Robert Fekety, Sherwood Gorbach, and their colleagues, with parallel work by groups in the United Kingdom — turned a clinical mystery into a solvable laboratory problem. The animals' diseased intestines, it turned out, were full of a clostridial toxin.
1978: Bartlett Closes the Loop
The pivotal year is 1978. In a now-classic paper in the New England Journal of Medicine, John G. Bartlett and colleagues reported that the stool of patients with antibiotic-associated pseudomembranous colitis contained a cytotoxin — a substance that killed cells in tissue culture — and that this toxin was produced by a clostridium. Just as importantly, the toxic activity could be neutralized by gas-gangrene (clostridial) antitoxin, the experimental fingerprint that tied the disease firmly to a toxin-producing Clostridium. The species responsible was identified as Clostridium difficile — the same organism Hall and O'Toole had named, and dismissed as harmless, forty-three years earlier.
This work rested on a precise chain of evidence assembled over the preceding year. A 1977 study by Bartlett, Onderdonk, Cisneros, and Kasper had already shown in the hamster model that clindamycin-associated colitis was caused by a toxin-producing species of Clostridium, with the same antitoxin-neutralization signature. The 1978 papers then connected that animal finding directly to human patients, fulfilling, in effect, a modern version of Koch's postulates for a toxin-mediated disease: the organism was present in the sick, it produced a toxin, the toxin reproduced the disease, and an antitoxin blocked it.
The consequences were immediate and lasting. The discovery explained why antibiotics could cause colitis (they cleared the way for C. diff), unmasked the long-mysterious cause of pseudomembranous colitis described back in 1893, and overturned the staphylococcal theory. It also established C. diff as a major healthcare-associated pathogen — one spread by hardy spores that survive on surfaces and resist many disinfectants — and it laid the groundwork for diagnostic testing, for the use of oral vancomycin and metronidazole as treatments, and for the toxin biology that would dominate the next phase of research.
The Toxins: A and B
Once C. diff was identified as a toxin-producing organism, attention turned to the toxins themselves. Two large protein toxins were characterized and named toxin A (TcdA) and toxin B (TcdB). In the early framework, TcdA was classed primarily as an "enterotoxin" (causing fluid secretion and tissue damage in the bowel) and TcdB as a more potent "cytotoxin" (the activity Bartlett's team had detected in tissue culture). Later work refined this picture, showing that both toxins damage cells by the same fundamental trick.
At the molecular level, both TcdA and TcdB are glucosyltransferases: once inside a host cell they chemically modify (glucosylate) a family of small regulatory proteins called Rho-family GTPases. These GTPases govern the cell's internal scaffolding, the actin cytoskeleton. Disabling them causes the lining cells of the colon to round up, lose their tight junctions, and die, breaking down the gut barrier and producing the intense inflammation and the characteristic pseudomembranes. The genes for both toxins, together with their regulators, sit in a defined chromosomal segment called the pathogenicity locus (PaLoc), whose regulatory genes (including tcdR and tcdC) control how much toxin a given strain produces.
Understanding the toxins reshaped both diagnosis and the long search for prevention. Detecting the toxins (or their genes) in stool became central to laboratory diagnosis, and the toxins are the targets of monoclonal-antibody therapy — bezlotoxumab, an antibody against toxin B, was developed to reduce recurrence — and of vaccine efforts aimed at neutralizing them. The balance of which toxin matters most has been debated, with substantial evidence pointing to toxin B as the dominant driver of disease, but for clinical and historical purposes the key fact is simple: no toxin, no disease. Non-toxigenic strains of C. diff can colonize the gut without causing colitis.
The NAP1/027 Hypervirulent Strain
For two decades after 1978, C. diff was a familiar but largely manageable hospital problem. That changed sharply in the early 2000s, when hospitals in North America — most visibly in the Canadian province of Quebec — and then in Europe experienced outbreaks of unusually severe, frequently fatal disease. The culprit was a single emergent strain known by several overlapping laboratory names: NAP1 (North American pulsed-field type 1), ribotype 027, and restriction-endonuclease group BI — together written BI/NAP1/027.
Two landmark 2005 reports in the New England Journal of Medicine defined the threat. Loo and colleagues described a predominantly clonal, multi-institutional Quebec outbreak with high morbidity and mortality, identifying a fluoroquinolone-resistant strain carrying binary toxin and a partial deletion of the tcdC regulatory gene. McDonald and colleagues independently characterized this "epidemic, toxin gene-variant strain" spreading across the United States. The strain's dangerous features clustered together: greatly increased production of toxins A and B (linked in part to the tcdC deletion that normally restrains them), an additional toxin called binary toxin (CDT), and high-level resistance to fluoroquinolone antibiotics — the last of which both promoted the disease (by clearing competing flora) and helped the strain spread through hospitals where those drugs were heavily used.
The NAP1/027 epidemic transformed C. diff from a nuisance into a public-health emergency and drove lasting change. It pushed antibiotic stewardship (especially restraint with fluoroquinolones), tougher infection control against spores, and a search for better treatments — ultimately including the antibiotic fidaxomicin and the renewed interest in restoring the gut microbiome directly. Although the dominance of ribotype 027 has waned in many regions since its peak, its emergence remains the defining modern chapter in the organism's history and a textbook example of how antibiotic pressure can select a more dangerous pathogen.
Fecal Microbiota Transplantation
If antibiotics cause C. diff disease by destroying the protective community of gut bacteria, then a logical — if startling — cure is to put that community back. This is the principle behind fecal microbiota transplantation (FMT): transferring stool, and with it a healthy donor's entire microbial ecosystem, into the gut of a patient with stubborn, recurrent C. diff. The idea is far older than the modern understanding that justifies it. In 1958, the Denver surgeon Ben Eiseman and colleagues reported in the journal Surgery that fecal enemas from healthy donors produced rapid recovery in four patients with life-threatening pseudomembranous enterocolitis — at a time when that disease was still blamed on staphylococci and carried a high mortality. Only decades later was it understood that the disease they had treated was, in most such cases, caused by C. diff, and that what cured it was the restoration of normal flora displacing the pathogen.
The modern scientific case for FMT was sealed by a single, decisive trial. In 2013, van Nood and colleagues published in the New England Journal of Medicine the first randomized controlled trial of donor-feces infusion for recurrent C. diff. Patients received either a duodenal infusion of donor stool (after a short course of vancomycin and a bowel lavage) or standard vancomycin therapy alone. The result was so lopsided — the great majority of FMT patients were cured versus only about a third of those on antibiotics alone — that the trial was stopped early on ethical grounds, because withholding the transplant from the control group could no longer be justified. The study also showed that FMT restored the patients' gut bacterial diversity toward that of healthy donors.
That trial moved FMT from medical folklore into mainstream practice for recurrent C. diff, and it accelerated the development of standardized, regulated successors: screened stool banks, encapsulated "crapsules," and defined microbiome-based products that have since been approved to prevent recurrence. FMT is not without risk — donor screening is essential, and at least one fatal transmission of a drug-resistant organism through FMT has been reported — but for patients trapped in cycles of relapse, it has been genuinely transformative, and it stands as one of the clearest demonstrations that the gut microbiome is itself a treatable organ. Practical detail on prevention of relapse appears in the related small-intestinal microbiome literature and on the main C. difficile page.
2016: From Clostridium to Clostridioides
The most recent twist in the story is taxonomic. As bacterial classification moved from physical traits to genetic-sequence comparison, it became clear that the sprawling genus Clostridium was not a tidy natural grouping, and that C. difficile sat well apart from the genus's true core (built around Clostridium butyricum). In 2016, Lawson, Citron, Tyrrell, and Finegold proposed reclassifying the organism into a brand-new genus, publishing "Reclassification of Clostridium difficile as Clostridioides difficile (Hall and O'Toole 1935) Prévot 1938" in the journal Anaerobe.
The new genus name Clostridioides — literally "Clostridium-like" — was chosen with deliberate care. By keeping the same opening letter C and much of the old spelling, the abbreviation "C. diff" survives unchanged, sparing clinicians, laboratories, and patients from confusion while still reflecting the genuine genetic distance from the rest of Clostridium. Note that the original authority — "(Hall and O'Toole 1935) Prévot 1938" — is carried forward in the formal name, a small piece of nomenclatural courtesy that preserves the 1935 discovery within the organism's official title.
Today, Clostridioides difficile is the validly published, recommended name in the scientific and medical literature, though the older Clostridium difficile remains common in everyday use and in older sources. Both refer to exactly the same bacterium. For a general audience the practical message is reassuring: the rename was a matter of more accurate biological bookkeeping, not the discovery of a new germ — the bug, the disease, and the trusty nickname are all unchanged.
Legacy and Open Questions
The arc of C. diff's history is a parable about the double-edged power of antibiotics. The drugs that conquered infectious disease also created the conditions for this opportunist to flourish, by stripping away the gut's own microbial defenses. From a misfiled infant commensal in 1935, to the unmasked villain of pseudomembranous colitis in 1978, to a hypervirulent epidemic strain in the 2000s, the organism has repeatedly forced medicine to think more carefully about how it uses antibiotics and how it protects, rather than merely sterilizes, the human gut.
Several active questions still shape research and practice. How can recurrence — the central clinical frustration of C. diff — best be prevented, using narrow-spectrum antibiotics like fidaxomicin, toxin-targeting antibodies, defined microbiome products, or full FMT? Why do some people carry toxigenic C. diff without ever getting sick (asymptomatic colonization), and what does that mean for testing and isolation? Can an effective vaccine against the toxins finally be achieved? And how should hospitals balance life-saving antibiotic use against the collateral damage to the microbiome that opens the door to C. diff in the first place?
What is certain is that the humble Latin word Hall and O'Toole reached for in 1935 — difficile, "difficult" — turned out to be prophetic in ways they could not have imagined. The organism was difficult to grow, difficult to recognize as a pathogen, and remains difficult to treat and to outsmart. Its history is one of the best illustrations in modern medicine of how a single microbe, and our changing relationship with the bacteria we carry, can reshape the way we practice care.
Research Papers and References
The references below trace the documented history of Clostridioides difficile from its 1935 description to the modern era of toxin biology, the NAP1/027 epidemic, fecal microbiota transplantation, and the 2016 reclassification. Where a stable DOI or PMID exists it is linked directly; older landmark papers that predate digital identifiers, and broader topic areas, are given as curated PubMed topic-search links. The 1893 description of pseudomembranous ("diphtheritic") colitis by J. M. T. Finney is named in the text as a historical primary source. Each link opens at the publisher or at PubMed (National Library of Medicine) in a new tab.
- Hall IC, O'Toole E. Intestinal flora in new-born infants: with a description of a new pathogenic anaerobe, Bacillus difficilis. American Journal of Diseases of Children. 1935;49(2):390-402. (Original isolation and naming; predates DOI indexing.) — PubMed: Hall & O'Toole, Bacillus difficilis
- Bartlett JG, Chang TW, Gurwith M, Gorbach SL, Onderdonk AB. Antibiotic-associated pseudomembranous colitis due to toxin-producing clostridia. New England Journal of Medicine. 1978;298(10):531-534. (The 1978 paper linking C. difficile toxin to human pseudomembranous colitis.) — doi:10.1056/NEJM197803092981003
- Bartlett JG, Onderdonk AB, Cisneros RL, Kasper DL. Clindamycin-associated colitis due to a toxin-producing species of Clostridium in hamsters. Journal of Infectious Diseases. 1977;136(5):701-705. (The hamster-model precursor to the 1978 human discovery.) — doi:10.1093/infdis/136.5.701
- Loo VG, Poirier L, Miller MA, et al. A predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. New England Journal of Medicine. 2005;353(23):2442-2449. (Defining the Quebec NAP1/027 epidemic.) — doi:10.1056/NEJMoa051639
- McDonald LC, Killgore GE, Thompson A, et al. An epidemic, toxin gene-variant strain of Clostridium difficile. New England Journal of Medicine. 2005;353(23):2433-2441. (U.S. characterization of the BI/NAP1/027 strain.) — doi:10.1056/NEJMoa051590
- Eiseman B, Silen W, Bascom GS, Kauvar AJ. Fecal enema as an adjunct in the treatment of pseudomembranous enterocolitis. Surgery. 1958;44(5):854-859. (First modern fecal microbiota transplantation; predates DOI indexing.) — PubMed: Eiseman, fecal enema (1958)
- van Nood E, Vrieze A, Nieuwdorp M, et al. Duodenal infusion of donor feces for recurrent Clostridium difficile. New England Journal of Medicine. 2013;368(5):407-415. (First randomized controlled trial of FMT; stopped early for efficacy.) — doi:10.1056/NEJMoa1205037
- Lawson PA, Citron DM, Tyrrell KL, Finegold SM. Reclassification of Clostridium difficile as Clostridioides difficile (Hall and O'Toole 1935) Prévot 1938. Anaerobe. 2016;40:95-99. (The 2016 genus reclassification.) — doi:10.1016/j.anaerobe.2016.06.008
- History of Clostridium difficile infection: early description, diagnosis, and molecular strain typing — PubMed: C. difficile early history and diagnosis
- John G. Bartlett and the discovery of C. difficile antibiotic-associated diarrhea (historical commentary) — PubMed: Bartlett and the discovery of C. difficile diarrhea
- Pseudomembranous colitis — history, pathology, and causes (Finney "diphtheritic colitis," staphylococcal era, and the C. difficile link) — PubMed: pseudomembranous colitis history
- Clostridioides difficile toxins A and B and the pathogenicity locus (PaLoc) — structure and mechanism — PubMed: C. difficile toxins A and B / PaLoc
- The hypervirulent BI/NAP1/027 strain of Clostridium difficile — epidemiology and binary toxin — PubMed: NAP1/027 hypervirulent strain
- Fecal microbiota transplantation for recurrent Clostridioides difficile infection — history and evidence — PubMed: FMT for recurrent C. difficile
External Authoritative Resources
- CDC — C. diff (Clostridioides difficile) Infection
- StatPearls (NCBI Bookshelf) — Clostridioides difficile Infection
- PubMed — All research on the history of Clostridioides difficile
Connections
- Infectious Disease
- Clostridium difficile: Causes, Symptoms, Treatment and Prevention — the clinical page for the organism this history traces — how antibiotics open the door, severity grading, testing, vancomycin and fidaxomicin, and why soap beats alcohol gel against the spores.
- Clostridium difficile (C. diff) — Main Page
- All Conditions
- Sepsis
- Inflammatory Bowel Disease
- Irritable Bowel Syndrome
- SIBO (Small Intestinal Bacterial Overgrowth)