Peptic Ulcer Disease: History and Discovery
For most of the twentieth century, peptic ulcers were blamed on stress, spicy food, and excess stomach acid — captured in the famous clinical maxim "no acid, no ulcer." Treatment meant antacids, bland diets, acid-suppressing drugs such as the H2-blocker cimetidine (first marketed in 1976), and, for severe cases, stomach surgery. Then two researchers in Perth, Western Australia — the pathologist Robin Warren and the young physician Barry Marshall — found spiral bacteria, later named Helicobacter pylori, living in the stomachs of ulcer patients. Warren had been seeing the organisms since 1979; the two began their formal partnership in 1981–1982 and published landmark papers in The Lancet in 1983 and 1984. Met with deep skepticism, in 1984 Marshall famously drank a culture of the bacterium, gave himself gastritis, and then cured it with antibiotics — helping prove that microbes, not stress, cause most ulcers. In 2005 Warren and Marshall received the Nobel Prize in Physiology or Medicine. Today the great majority of peptic ulcers are cured with a short course of antibiotics; most of the rest are caused by NSAID painkillers. Strikingly, earlier observers had glimpsed these same bacteria for nearly a century — only to be doubted, ignored, and forgotten.
Table of Contents
- What a Peptic Ulcer Is
- The Acid Era: "No Acid, No Ulcer"
- The Forgotten Observers (1875–1940)
- Warren and Marshall in Perth
- The Self-Experiment of 1984
- Skepticism and the Slow Turning of the Tide
- A Paradigm Shift and the 2005 Nobel Prize
- Modern Treatment and What History Teaches
- Research Papers and References
- Connections
- Featured Videos
What a Peptic Ulcer Is
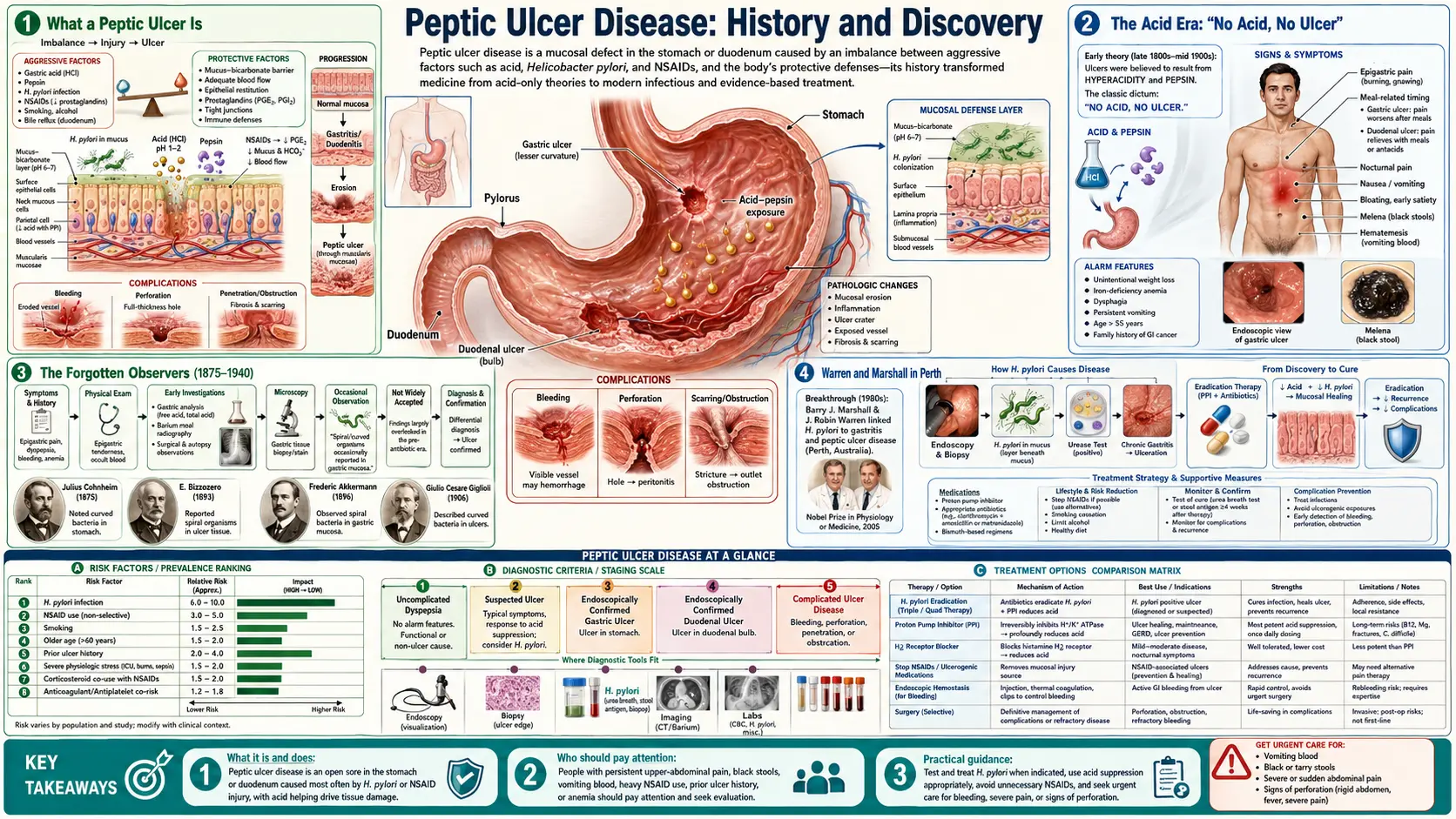
A peptic ulcer is an open sore in the lining of the upper digestive tract, where the protective mucous barrier has been breached and the underlying tissue is exposed to corrosive stomach acid and the digestive enzyme pepsin — the word peptic comes from pepsin. When the sore sits in the stomach itself it is called a gastric ulcer; when it sits just beyond, in the first part of the small intestine, it is a duodenal ulcer. Both have plagued humanity for as long as records exist, producing the classic gnawing or burning pain in the upper abdomen, and, in their dangerous forms, internal bleeding or a perforation that lets stomach contents leak into the abdominal cavity — a surgical emergency that, before modern care, was frequently fatal.
For centuries the ulcer was one of medicine's most familiar yet most baffling afflictions. Physicians could see the damage at autopsy and feel the misery in their patients, but the underlying cause stayed out of reach. The story of how that cause was finally found is one of the great detective stories of modern medicine — and a cautionary tale about how a confident, plausible, deeply entrenched theory can blind a profession to the truth sitting in plain sight under its microscopes.
The Acid Era: "No Acid, No Ulcer"
By the early twentieth century, medicine had settled on a tidy and self-evident explanation. Ulcers occurred where stomach acid met tissue; therefore acid — together with the stress and rich, spicy food thought to drive its overproduction — was the culprit. The principle was crystallized in 1910 by the German surgeon Karl Schwarz in the dictum "ohne sauren Magensaft kein peptisches Geschwür" — "no acid, no ulcer." It was simple, it was logical, and it fit the chemistry everyone could measure. The idea that bacteria might be involved was dismissed almost out of hand, because of a powerful and reasonable-sounding assumption: surely nothing could survive in the brutally acidic bath of the human stomach. The stomach was held to be essentially sterile.
Treatment followed directly from the theory. Patients were prescribed antacids to neutralize acid, milk and bland "ulcer diets" to soothe it, bed rest, and instructions to avoid stress, coffee, alcohol, and spicy food. A genuine pharmacological breakthrough arrived in the 1970s: Sir James Black's team developed the histamine H2-receptor antagonists, drugs that switched off acid secretion at its source. The first, cimetidine (brand name Tagamet), was first marketed in 1976 and became one of the world's best-selling drugs; ranitidine followed. Later still came the even more powerful proton-pump inhibitors. These drugs were a real advance — they reliably healed ulcers and relieved suffering on a scale never seen before.
But there was a stubborn problem hiding inside this success. Acid-suppressing drugs healed ulcers, yet once the medication stopped, the ulcers very often came back. Patients faced relapse after relapse, and many were placed on acid-suppressing pills indefinitely, or sent to surgeons who cut the vagus nerve (vagotomy) or removed part of the stomach to curb acid for good. The treatments managed the symptom brilliantly but never touched the cause — a clue, in plain view, that the "no acid, no ulcer" story was incomplete.
The Forgotten Observers (1875–1940)
One of the most sobering parts of this history is that the bacteria were not new in 1982. They had been seen, described, and even illustrated repeatedly across the preceding century — and then forgotten each time. Spiral organisms in the stomachs of animals were reported by several nineteenth-century investigators, and the Italian pathologist Giulio Bizzozero famously described spiral bacteria living in the acidic gastric glands of dogs in 1893. In humans, spiral organisms in the gastric mucosa were noted early in the twentieth century — commonly credited to Walery Krienitz in 1906 — and a notably thorough study was published in 1939 by the American pathologist J. L. Doenges, who reported finding spiral organisms in a large fraction of human stomachs examined at autopsy.
Why did these findings sink without trace? Partly because no one could grow the fastidious organism in culture, so it could not be properly studied, named, or shown to cause anything. Partly because the bacteria were easy to dismiss as harmless passengers, or as contamination that crept in after death. And overwhelmingly because they collided head-on with the reigning dogma: the stomach was "known" to be sterile and ulcers were "known" to be caused by acid, so observations to the contrary were quietly filed away as curiosities. Each generation of observers was, in effect, talking into a wind of settled opinion that carried their words away.
This is the crucial backdrop to what Warren and Marshall accomplished, and it is why their contribution is rightly called a discovery despite those earlier sightings. Seeing an organism is not the same as proving what it does. The lasting achievement of the Perth team was not merely to look down a microscope, but to culture the bacterium, characterize it, link it systematically to disease, and ultimately demonstrate cause and cure — turning a century of ignored observations into established medical fact.
Warren and Marshall in Perth
In 1979, J. Robin Warren, a pathologist at Royal Perth Hospital in Western Australia, noticed something his training told him should not be there: curved, spiral bacteria colonizing the lining of stomach biopsies, consistently clustered where the tissue was inflamed. Rather than dismiss them as artifacts, Warren paid careful attention, documenting the association between the bacteria and active gastritis over the following years. In 1981 he was joined by Barry J. Marshall, a young internal-medicine trainee looking for a research project. Where Warren brought the patient, methodical eye of the pathologist, Marshall brought relentless energy and a willingness to push the idea to its limits.
Together they studied biopsies from a series of roughly a hundred patients and found the spiral bacteria present in the overwhelming majority of those with gastritis and peptic ulcers. The breakthrough on the laboratory side came in 1982, and partly by luck: the organism is slow-growing and had defeated earlier attempts to culture it, but a set of culture plates left in the incubator over the Easter long weekend — far longer than the usual two days — finally yielded visible colonies. Marshall had cultured the elusive bacterium. It was eventually given the name Helicobacter pylori ("spiral bacterium of the pylorus"), reflecting both its corkscrew shape and its home near the stomach's outlet.
The pair published their findings as two letters in The Lancet in June 1983, and then in a fuller 1984 paper titled "Unidentified Curved Bacilli in the Stomach of Patients with Gastritis and Peptic Ulceration." Their proposal was radical: that a bacterial infection — not stress, not diet, not acid alone — was the real driver of chronic gastritis and most peptic ulcers, and that ulcers might therefore be cured with antibiotics. At this stage the central claim was an hypothesis: a strong, well-supported one, but one that still had to satisfy a skeptical scientific world that the bacteria were the cause of the disease and not merely innocent bystanders found at the scene.
The Self-Experiment of 1984
The biggest obstacle was Koch's postulates — the classic nineteenth-century criteria for proving that a particular microbe causes a particular disease. One demands that the organism, introduced into a healthy host, reproduce the illness. The ethical route, deliberately infecting healthy people's stomachs, was unthinkable; and the bacterium did not reliably infect the usual laboratory animals. Frustrated by the wall of doubt and unable to wait, Barry Marshall took the most direct subject available: himself.
In 1984, after an endoscopy confirmed his own stomach lining was healthy, Marshall drank a cloudy broth containing a culture of Helicobacter pylori taken from a patient. Within days he became unwell — nauseated, with bad breath and vomiting. A repeat endoscopy and biopsy about a week later showed exactly what the hypothesis predicted: his once-normal stomach lining was now inflamed with active gastritis, and the bacterium was present in the tissue. He had given himself the disease. He then took antibiotics together with bismuth, his symptoms resolved, and the infection cleared. By infecting himself, producing the illness, and then curing it, Marshall had provided dramatic, headline-grabbing evidence that the bacterium was a genuine cause of gastric disease — not a harmless passenger.
The self-experiment did not prove the whole story by itself — gastritis is a step on the road to ulcers rather than an ulcer outright, and a single human subject is not a clinical trial. But its scientific and rhetorical power was enormous. It was vivid, brave, and impossible to ignore, and it forced a complacent field to take the bacterial hypothesis seriously. It has since become one of the most celebrated acts of self-experimentation in the history of medicine, a story told to students precisely because it shows how far a researcher may have to go to dislodge an entrenched idea.
Skepticism and the Slow Turning of the Tide
It is hard to overstate how unwelcome this idea was at first. The notion that a bacterium caused ulcers contradicted decades of textbooks, the entire acid-centered model of the disease, and the "sterile stomach" assumption that nearly everyone took for granted. There were also powerful interests aligned with the status quo: acid-suppressing drugs were among the best-selling medications in the world, and an industry of long-term ulcer management had grown up around them. A cheap two-week course of antibiotics that could cure the disease outright was, to put it mildly, a disruptive proposition.
So the medical establishment resisted, often dismissively. Marshall later recalled the period with some bitterness, describing how their work was met with disbelief and how he struggled to be taken seriously. But the evidence kept accumulating from his and Warren's laboratory and, crucially, from other groups around the world who began to confirm the findings: H. pylori was present in the great majority of duodenal ulcers and a large share of gastric ulcers, and — the decisive point — eradicating the bacterium with antibiotics dramatically reduced the relentless relapses that had defined the disease. Curing the infection, it turned out, could cure the ulcer for good.
The institutional turning point came in 1994, when a United States National Institutes of Health Consensus Development Conference concluded that H. pylori was causally linked to peptic ulcer disease and recommended antibiotic treatment for infected ulcer patients. From that moment the new understanding moved rapidly from heresy to standard of care, and a generation of patients who would once have faced lifelong pills or surgery were instead simply cured.
A Paradigm Shift and the 2005 Nobel Prize
The Helicobacter pylori story is regularly cited as a textbook example of a scientific paradigm shift — one of those rare moments when a field abandons a long-held framework and rebuilds its understanding from a new foundation. Within a couple of decades, peptic ulcer disease went from being seen as a chronic, lifestyle-driven, acid-related condition to being recognized, in most cases, as a curable bacterial infection. Few changes in medicine have been so complete, so rapid, or so directly beneficial to patients.
The recognition was sealed in October 2005, when the Nobel Assembly at the Karolinska Institute awarded the Nobel Prize in Physiology or Medicine to Barry J. Marshall and J. Robin Warren — in the committee's words, "for their discovery of the bacterium Helicobacter pylori and its role in gastritis and peptic ulcer disease." The Nobel committee explicitly praised the pair for tenacity and intellectual courage in challenging prevailing dogma, a rare and pointed acknowledgment that the obstacle they overcame was not only scientific but cultural — the resistance of a confident establishment to an inconvenient truth.
The discovery's reach extends beyond ulcers. H. pylori is now understood to be a major cause of chronic gastritis and a recognized risk factor for stomach (gastric) cancer; the bacterium has been classified as a carcinogen, making its eradication a measure of cancer prevention as well as ulcer cure. What began as a stubborn pathologist's refusal to ignore something odd under his microscope ended by reshaping the prevention of one of the world's most common cancers.
Modern Treatment and What History Teaches
Today, when a peptic ulcer is found, the first question is whether Helicobacter pylori is present — tested by a breath test, a stool antigen test, a blood antibody test, or a biopsy taken during endoscopy. If the infection is found, the standard cure is a short course of combination therapy: typically two antibiotics plus a proton-pump inhibitor (and often bismuth), taken for one to two weeks, regimens that evolved directly from Marshall's original antibiotic-plus-bismuth approach. For the substantial minority of ulcers not caused by the bacterium, the leading culprit is regular use of nonsteroidal anti-inflammatory drugs (NSAIDs) such as aspirin and ibuprofen, which erode the stomach's protective defenses; these ulcers are managed by stopping the offending drug where possible and suppressing acid to let the lining heal.
This is a genuinely happy ending in medicine. A disease that once meant chronic pain, repeated bleeding, lifelong medication, and sometimes major stomach surgery is now, in most cases, straightforwardly curable — often permanently — with inexpensive pills. The old advice to manage ulcers chiefly by reducing stress and eating bland food has been retired as a cause-and-cure story, though stress and certain foods can still aggravate symptoms and NSAIDs remain genuinely important. The center of gravity moved from soothing the acid to eliminating the infection.
The deeper lesson of this history reaches past gastroenterology. The bacteria that cause ulcers were visible under microscopes for roughly a hundred years before anyone acted on them, because a plausible, profitable, deeply entrenched theory taught a whole profession not to see what was in front of it. It took careful observation, a willingness to question authority, hard laboratory work, an act of personal courage, and years of patient confirmation to overturn that consensus. For a free public-knowledge resource, that is the story worth remembering: settled science is sometimes wrong, evidence must be allowed to win, and the humility to doubt our own certainties is itself a tool of healing.
Research Papers and References
The references below combine the landmark primary papers by Warren and Marshall, the 2005 Nobel Prize materials, and authoritative reviews of the history of Helicobacter pylori and peptic ulcer disease. Where a stable identifier is available, a DOI, PMID, or PubMed Central link is given; the remaining entries are curated PubMed topic searches into the historical and clinical literature. Each link opens at its source (National Library of Medicine or the publisher) in a new tab. Historical priority claims (Bizzozero 1893, Krienitz 1906, Doenges 1939, Schwarz's 1910 "no acid, no ulcer") are described in the article as historical sources.
- Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet. 1984;1(8390):1311-1315. — doi:10.1016/S0140-6736(84)91816-6 · PMID 6145023
- Warren JR, Marshall B. Unidentified curved bacilli on gastric epithelium in active chronic gastritis. Lancet. 1983;1(8336):1273-1275. — PMID 6134060
- Marshall BJ, Armstrong JA, McGechie DB, Glancy RJ. Attempt to fulfil Koch's postulates for pyloric Campylobacter. Medical Journal of Australia. 1985;142(8):436-439 (Marshall's self-ingestion experiment). — PMID 3982345
- The Nobel Prize in Physiology or Medicine 2005 — Barry J. Marshall and J. Robin Warren (official press release and prize information). — NobelPrize.org — 2005 Press Release
- Barry J. Marshall — Nobel Lecture (2005): "Helicobacter Connections." — NobelPrize.org — Marshall Nobel Lecture
- NIH Consensus Development Panel. Helicobacter pylori in peptic ulcer disease. JAMA. 1994;272(1):65-69. — PMID 8007082
- Kidd M, Modlin IM. A century of Helicobacter pylori: paradigms lost — paradigms regained. Digestion. 1998;59(1):1-15. — PMID 9468093
- Pajares JM, Gisbert JP. Helicobacter pylori: its discovery and relevance for medicine. Revista Española de Enfermedades Digestivas. 2006;98(10):770-785. — PubMed: history of H. pylori discovery
- Konturek JW. Discovery of Helicobacter pylori and its role in gastroduodenal disease (historical review). — PubMed: Helicobacter pylori history of discovery
- Giulio Bizzozero and the early history of gastric spiral organisms (1893). — PubMed: Bizzozero and gastric spiral bacteria
- Barry Marshall's self-experimentation and Koch's postulates (historical accounts). — PubMed: Marshall self-experiment and Koch's postulates
- Helicobacter pylori as a carcinogen and risk factor for gastric cancer. — PubMed: H. pylori and gastric cancer
- Cimetidine, H2-receptor antagonists, and the history of acid-suppression therapy. — PubMed: cimetidine and acid-suppression history
- Modern eradication therapy for Helicobacter pylori in peptic ulcer disease. — PubMed: H. pylori eradication therapy
External Authoritative Resources
- NobelPrize.org — The Nobel Prize in Physiology or Medicine 2005
- NIDDK (NIH) — Peptic Ulcers (Stomach Ulcers)
- PubMed — All research on H. pylori and peptic ulcer history
Connections
- Gastroenterology
- Peptic Ulcer Disease
- Gastroesophageal Reflux Disease (GERD)
- Small Intestinal Bacterial Overgrowth (SIBO)
- All Conditions