Rosacea: History and Discovery
The flushed, ruddy face of rosacea has been noticed for more than six centuries. Medieval physicians called it gutta rosacea — the “rosy drop” — and Geoffrey Chaucer’s Canterbury Tales (around 1387) painted a red-faced, pimpled pilgrim, the Summoner, that later writers often cite as one of the earliest literary portraits of the condition. From the French surgeon Guy de Chauliac’s “goutterose” to the Victorian label “acne rosacea” (later dropped, because rosacea is not a form of acne), and from the unfair myth of the alcoholic “rum nose” to today’s map of mites, blood vessels, nerves, and immune peptides, this is the story of how a stubborn red face slowly became an understood disease.
Table of Contents
- What Rosacea Is — and What History Got Wrong
- Ancient Hints and the Medieval “Rosy Drop”
- Chaucer, Shakespeare, and the Red Face in Literature
- The Nineteenth Century: Willan, Bateman, and “Acne Rosacea”
- The Mite on the Face: Demodex Enters the Story
- Rhinophyma and the Unfair “Whiskey Nose” Stigma
- Modern Cause Theories: Vessels, Nerves, Immunity, and the Gut
- Modern Classification and Treatment (2002 to Today)
- Research Papers and References
- Connections
- Featured Videos
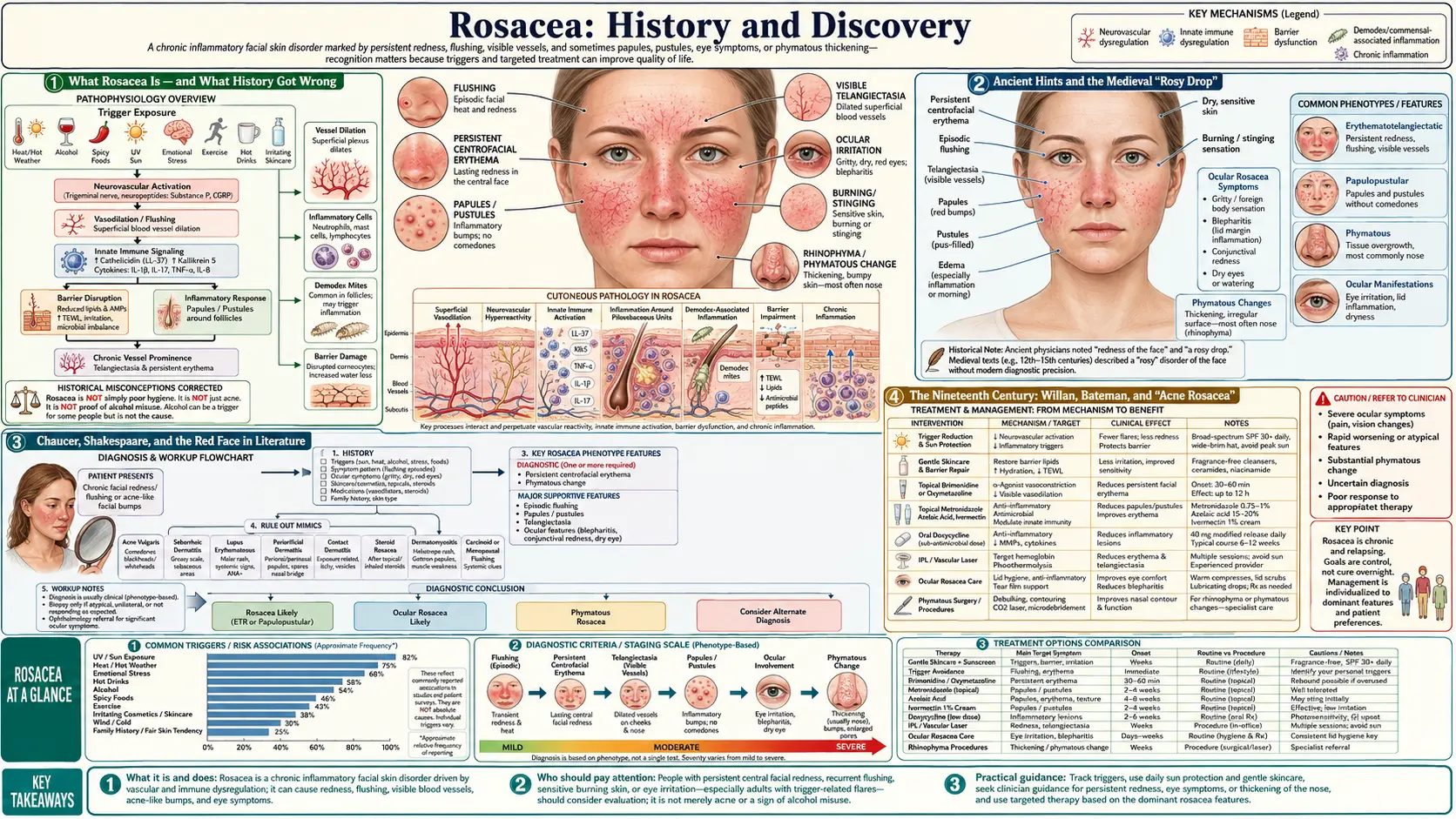
What Rosacea Is — and What History Got Wrong
Rosacea is a common, chronic inflammatory skin disorder that centers on the face — most often the cheeks, nose, chin, and forehead. Its hallmarks are persistent redness (erythema), flushing, visible small blood vessels (telangiectasia), and sometimes acne-like bumps and pustules. In some people the eyes are affected (ocular rosacea), and in a minority the skin of the nose thickens into the knobby enlargement called rhinophyma. It tends to favor fair-skinned adults of northern and western European ancestry, which is one reason its history is so densely recorded in European art and literature.
Reading old descriptions of rosacea calls for care, because three different things are easily tangled together: the historical names for the visible redness (gutta rosacea, goutterose, couperose, acne rosacea); the modern medical entity we now define by specific signs and subtypes; and the long list of cause theories people have proposed, from bad blood to bad wine to a face mite. Many of those old explanations were wrong, and some did real harm by attaching shame to a medical condition. This page keeps the three threads separate — we will note when a historical writer was simply observing a red face, when they were guessing at a cause, and where the modern evidence actually stands.
One theme runs through the whole story. For most of recorded history, a chronically red, swollen, or pimpled face was read as a sign of character — of intemperance, of drink, of sin — rather than as a sign of a blood-vessel and immune disorder. Untangling rosacea from that moral judgment, and especially separating the bulbous nose of rhinophyma from the myth of the “drinker’s nose,” is one of the most important corrections modern dermatology has made.
Ancient Hints and the Medieval “Rosy Drop”
Possible references to a rosacea-like red face reach back to antiquity. Some authors point to the Greek poet Theocritus (3rd century BCE) and to scattered classical mentions of red, flushed faces, and a number of antique sculptures and portraits show the swollen, reddened nose that looks very much like rhinophyma. These are intriguing but should be read as possible early depictions rather than firm diagnoses — we cannot examine a marble bust or a line of verse the way a dermatologist examines a patient, so any ancient “case” of rosacea is an educated guess.
The first clear medical description belongs to the 14th century and to the great French surgeon Guy de Chauliac (c. 1300–1368), author of the influential surgical text Chirurgia Magna (1363). De Chauliac described the red lesions he saw on the cheeks and nose of certain patients and gave the condition the names “goutterose” (a “rosy drop” or “pink droplet”) and “couperose,” the latter still used as the everyday French word for rosacea today. The same condition appears in Latin as gutta rosa or gutta rosacea — literally the “rosy drop” — the phrase from which the modern word rosacea ultimately descends.
The medieval understanding of the cause was, by modern standards, mistaken, and the treatments followed from it. Working within the humoral medicine of his day, de Chauliac attributed the redness to disordered blood and recommended such measures as a cooling diet, bloodletting from a vein in the forehead, applying leeches inside the nostrils, and purging. None of this addressed the real biology of rosacea, but the name he supplied — the “rosy drop” — was durable, and it fixed in European medicine the idea that this particular facial redness was a distinct, nameable complaint.
Chaucer, Shakespeare, and the Red Face in Literature
Some of the most vivid early evidence for rosacea is literary rather than medical. In Geoffrey Chaucer’s The Canterbury Tales (written around 1387–1400), the pilgrim known as the Summoner is described with a fire-red, pimpled, lumpy face so inflamed and unsightly that children are said to be frightened of him — a face no ointment could cure. Modern commentators frequently read this portrait as one of the earliest detailed literary depictions of severe rosacea, though it is worth noting honestly that Chaucer was writing satire, not a clinical chart: scholars have also proposed scabies, late-stage syphilis, or other disfiguring skin disease, and “gutta rosacea” is one interpretation among several. As a piece of historical evidence it shows that a chronically red, pustular face was a recognizable human type in the 1300s — and, tellingly, already a stigmatized one.
Two centuries later, William Shakespeare gave the theme its most famous comic face. In Henry IV and Henry V the character Bardolph is mocked for his fiery, carbuncled, glowing-red nose — a description that matches rhinophyma and the flushing of rosacea, and which Shakespeare, like the culture around him, ties firmly to heavy drinking. Bardolph’s “bardolph nose” entered the language as shorthand for the red nose of the tippler, helping cement a connection between a swollen red nose and alcohol that medicine would spend centuries trying to correct.
These literary portraits matter for two reasons. First, they are precious historical documentation: long before dermatology existed as a field, writers were recording, in close detail, the signs we now group under rosacea. Second, they reveal the attitude that shadowed the disease — the red face as a moral verdict, a visible sign of gluttony or drink. That stigma, more than any medical theory, is what later patients had to live with.
The Nineteenth Century: Willan, Bateman, and “Acne Rosacea”
Rosacea became a properly classified medical condition in the early 19th century, as British physicians built the first systematic taxonomy of skin disease. Robert Willan (1757–1812), often called a founder of modern dermatology, pioneered an approach that classified skin diseases by the form of their lesions rather than by supposed internal causes; he is credited with giving one of the first accurate descriptions of this condition. His pupil and successor Thomas Bateman (1778–1821) carried the work forward, and it is in Bateman’s widely read English text of 1812 that the term “acne rosacea” appears in print — accompanied by Bateman’s candid and oft-quoted admission that “the perfect cure of acne rosacea is, in fact, never accomplished.”
The label “acne rosacea” reflected the visible overlap with acne — both conditions can produce papules and pustules on the face — and through the Victorian era it became the standard English name, used by the prominent dermatologists of the day. (The earlier French and Latin terms, goutterose and gutta rosa, faded as “acne rosacea” took hold.) Nineteenth-century atlases, including the hand-colored illustrations associated with Willan and Bateman’s On Cutaneous Diseases, gave physicians some of the first standardized images of the disorder, helping move diagnosis from anecdote toward shared visual definition.
Over the following century, doctors came to understand that the resemblance to acne was misleading. Acne is fundamentally a disorder of the oil glands and follicles driven by sebum, bacteria, and clogged pores, whereas rosacea is centered on flushing, blood-vessel changes, and inflammation, and notably lacks the comedones (blackheads and whiteheads) that define acne. Because the two are distinct diseases with different mechanisms and treatments, the “acne” qualifier was eventually dropped and the condition came to be called simply rosacea — the name in standard use today.
The Mite on the Face: Demodex Enters the Story
One of the most enduring questions about rosacea concerns a microscopic resident of human skin: the hair-follicle mite Demodex folliculorum. The mite itself was discovered at the dawn of microscopy — first reported by the German anatomist Jakob Henle in 1841, then described in detail in 1842 by the German dermatologist Gustav Simon, who spotted the creatures moving in follicle samples while studying acne; the English naturalist Richard Owen gave the genus the name Demodex the following year. Demodex mites are normal inhabitants of human facial skin, living harmlessly in the follicles of most adults.
What links them to rosacea is abundance. Researchers have repeatedly found that people with rosacea — particularly the papulopustular form — tend to carry markedly higher densities of Demodex mites in their facial skin than people without the condition. This has led to the long-standing hypothesis that the mites, or the bacteria they harbor (such as Bacillus oleronius), provoke the immune inflammation of rosacea. It remains genuinely unresolved which way the arrow points: it is not yet settled whether the mites help cause rosacea, or whether the inflamed, altered skin of rosacea simply makes a more welcoming home in which the mites multiply — a classic chicken-and-egg problem.
The mite hypothesis is more than academic. It underpins one of the modern era’s most useful treatments — topical ivermectin, an anti-parasitic that reduces Demodex numbers and calms inflammation, approved for papulopustular rosacea in 2014 (discussed below). So while “Demodex causes rosacea” should be presented strictly as an unproven hypothesis, the mite is unquestionably part of the picture for many patients, and targeting it can help.
Rhinophyma and the Unfair “Whiskey Nose” Stigma
Rhinophyma is the late, severe, phymatous form of rosacea in which the skin of the nose gradually thickens and the oil glands enlarge, producing a bulbous, knobby, often reddened nose. It develops over years, occurs far more often in men than women, and represents an advanced stage of long-standing, usually untreated rosacea. For centuries it carried — and to a damaging degree still carries — a different name in popular speech: the “rum nose,” “whiskey nose,” “drinker’s nose,” or “gin blossom.”
That association was reinforced by culture far more than by medicine. Shakespeare’s Bardolph (above) is the literary archetype, and in the early 20th century the American comedian W.C. Fields, whose prominent bulbous nose became part of his public persona, famously joked about his “gin blossoms” — cementing in the popular imagination the idea that a big red nose means a big drinker. The result was a cruel and lasting stigma: people with rhinophyma were widely assumed to be alcoholics on sight.
The modern evidence shows this stigma to be largely mistaken. Rhinophyma is a manifestation of rosacea, not a product of alcohol; studies indicate it occurs in people who drink little or no alcohol as well as in those who drink, and it is driven by the underlying rosacea (with genetic susceptibility), not by drinking. The honest, evidence-based nuance is this: alcohol does not cause rosacea or rhinophyma, but because alcohol — like heat, spicy food, sun, and stress — is a common trigger of facial flushing, it can aggravate redness in someone who already has the condition. (One recent study did report that, among people who already have rhinophyma, heavier drinking was associated with greater severity, but that is a far cry from alcohol being the cause.) Correcting the “drinker’s nose” myth is one of the clearest public-health messages in the whole history of rosacea: a bulbous red nose is a treatable medical sign, not a confession.
Modern Cause Theories: Vessels, Nerves, Immunity, and the Gut
For all its long history of description, rosacea’s underlying cause is still not fully settled, and the modern view is that it is multifactorial — the end result of several interacting problems rather than one single cause. In a genetically susceptible person, the leading model combines a dysregulated innate immune system, abnormal neurovascular signaling (over-reactive blood vessels and nerves that drive flushing and lingering redness), and contributions from skin microorganisms such as Demodex mites. A landmark advance came in 2007, when researchers reported that people with rosacea have abnormally high levels of cathelicidin — an antimicrobial peptide of the innate immune system — and process it into inflammatory fragments, linking the redness and bumps to a specific immune pathway. This cathelicidin finding is one of the firmer pieces of modern rosacea biology and helped reframe the disease as fundamentally inflammatory.
A separate and much-discussed line of inquiry connects rosacea to the gut — the so-called gut–skin axis. Two associations in particular get attention, and both should be presented as hypotheses under active study, not established cause. The first is Helicobacter pylori, the stomach bacterium behind many ulcers: some studies have reported higher H. pylori rates in rosacea patients and improvement after eradication, but the literature is genuinely conflicting, with other controlled studies finding no such link, so the connection remains debated. The second is small intestinal bacterial overgrowth (SIBO): a frequently cited study found SIBO more common in people with rosacea and reported notable skin clearing after treatment, yet other work has not confirmed a statistically robust association, and testing methods vary widely. The fair summary is that an intriguing gut connection keeps surfacing in the data, but it has not been proven to cause rosacea.
Other proposed contributors — ultraviolet sun damage, abnormalities of facial blood vessels and lymphatics, and reactive oxygen species — layer onto the same picture. The practical takeaway from a century of cause-hunting is that no one factor explains every case; rosacea is best understood as a convergence of immune, vascular, neural, microbial, and environmental influences, which is exactly why its treatment is aimed at several targets at once.
Modern Classification and Treatment (2002 to Today)
The modern era of rosacea care opened with a definition. In 2002, the National Rosacea Society Expert Committee published a Standard Classification of Rosacea (Wilkin and colleagues, in the Journal of the American Academy of Dermatology), which for the first time gave clinicians and researchers an agreed vocabulary. It described four subtypes: subtype 1, erythematotelangiectatic (flushing and persistent redness with visible vessels); subtype 2, papulopustular (the “acne-like” bumps and pustules); subtype 3, phymatous (skin thickening, including rhinophyma); and subtype 4, ocular (eye involvement). A 2017–2018 update by the same society refined this into a phenotype-based approach — diagnosing and treating by the individual features a patient actually has, since many people have a mix — but the 2002 framework remains the historical turning point that made rigorous study possible.
Treatment, too, has been transformed. Where de Chauliac offered leeches and bloodletting and Bateman frankly doubted a cure was possible, today’s clinician has an evidence-based toolkit. Mainstays include topical metronidazole and azelaic acid for inflammatory bumps; topical ivermectin (approved 2014), which targets Demodex and inflammation; sub-antimicrobial-dose oral doxycycline for its anti-inflammatory effect; and topical vasoconstrictors such as brimonidine (approved 2013) and oxymetazoline (approved 2017) to reduce the persistent redness of flushing. More recently a topical minocycline foam was added to the options.
For the visible blood vessels and fixed redness, light- and laser-based therapies — pulsed-dye lasers, intense pulsed light (IPL), and Nd:YAG lasers — can selectively target dilated vessels, while the thickened tissue of advanced rhinophyma can be reshaped surgically or with ablative lasers. Alongside the medications, modern care emphasizes identifying and avoiding personal triggers (sun, heat, spicy food, alcohol, stress), gentle skin care, and daily sun protection. The arc is striking: from a stigmatized “rosy drop” blamed on bad blood or strong drink, rosacea has become a defined, multifactorial, and — while not curable — very manageable condition. None of the treatments named here is a personal medical recommendation; anyone with rosacea should work with a qualified clinician to choose an approach.
Research Papers and References
The references below combine peer-reviewed sources on the history, classification, and biology of rosacea with curated PubMed topic-search links into the historical and clinical literature. Historical primary texts (Guy de Chauliac’s Chirurgia Magna, Chaucer’s Canterbury Tales, Shakespeare’s Henry IV, and Willan and Bateman’s On Cutaneous Diseases) are named in the article as historical sources rather than as modern citations. Each link opens in a new tab.
- Wilkin J, Dahl M, Detmar M, Drake L, Feinstein A, Odom R, Powell F. Standard classification of rosacea: report of the National Rosacea Society Expert Committee on the Classification and Staging of Rosacea. Journal of the American Academy of Dermatology. 2002;46(4):584-587. — doi:10.1067/mjd.2002.120625 (PMID 11907512)
- Gallo RL, Granstein RD, Kang S, et al. Standard classification and pathophysiology of rosacea: the 2017 update by the National Rosacea Society Expert Committee. Journal of the American Academy of Dermatology. 2018;78(1):148-155. — doi:10.1016/j.jaad.2017.08.037
- Yamasaki K, Di Nardo A, Bardan A, et al. Increased serine protease activity and cathelicidin promotes skin inflammation in rosacea. Nature Medicine. 2007;13(8):975-980. — doi:10.1038/nm1616
- Gravina A, Federico A, Ruocco E, et al. Helicobacter pylori infection but not small intestinal bacterial overgrowth may play a pathogenic role in rosacea. United European Gastroenterology Journal. 2015;3(1):17-24. — doi:10.1177/2050640614559262 (PMID 25653855)
- Daou H, Paradiso M, Hennessy K, Seminario-Vidal L. Rosacea and the microbiome: a systematic review. Dermatology and Therapy. 2021;11(1):1-12. — doi:10.1007/s13555-020-00460-1
- Two AM, Wu W, Gallo RL, Hata TR. Rosacea: part I. Introduction, categorization, histology, pathogenesis, and risk factors. Journal of the American Academy of Dermatology. 2015;72(5):749-758. — doi:10.1016/j.jaad.2014.08.028
- Guy de Chauliac and the early history / naming of rosacea (goutterose, couperose, gutta rosacea) — PubMed: rosacea history and early naming
- Medical history and representation of rosacea in the 19th century (Willan, Bateman, “acne rosacea”) — PubMed: rosacea in the 19th century
- Demodex folliculorum mites and the pathogenesis of rosacea — PubMed: Demodex and rosacea
- Rhinophyma, alcohol, and the “drinker’s nose” misconception — PubMed: rhinophyma and alcohol
- Topical ivermectin for papulopustular rosacea (anti-Demodex therapy) — PubMed: ivermectin for rosacea
- Rosacea, gut microbiome, SIBO, and the gut–skin axis — PubMed: rosacea and the gut–skin axis
- Treatment of rosacea: metronidazole, azelaic acid, doxycycline, brimonidine, laser — PubMed: rosacea treatment
External Authoritative Resources
- National Rosacea Society — All About Rosacea
- American Academy of Dermatology — Rosacea
- PubMed — All research on the history of rosacea