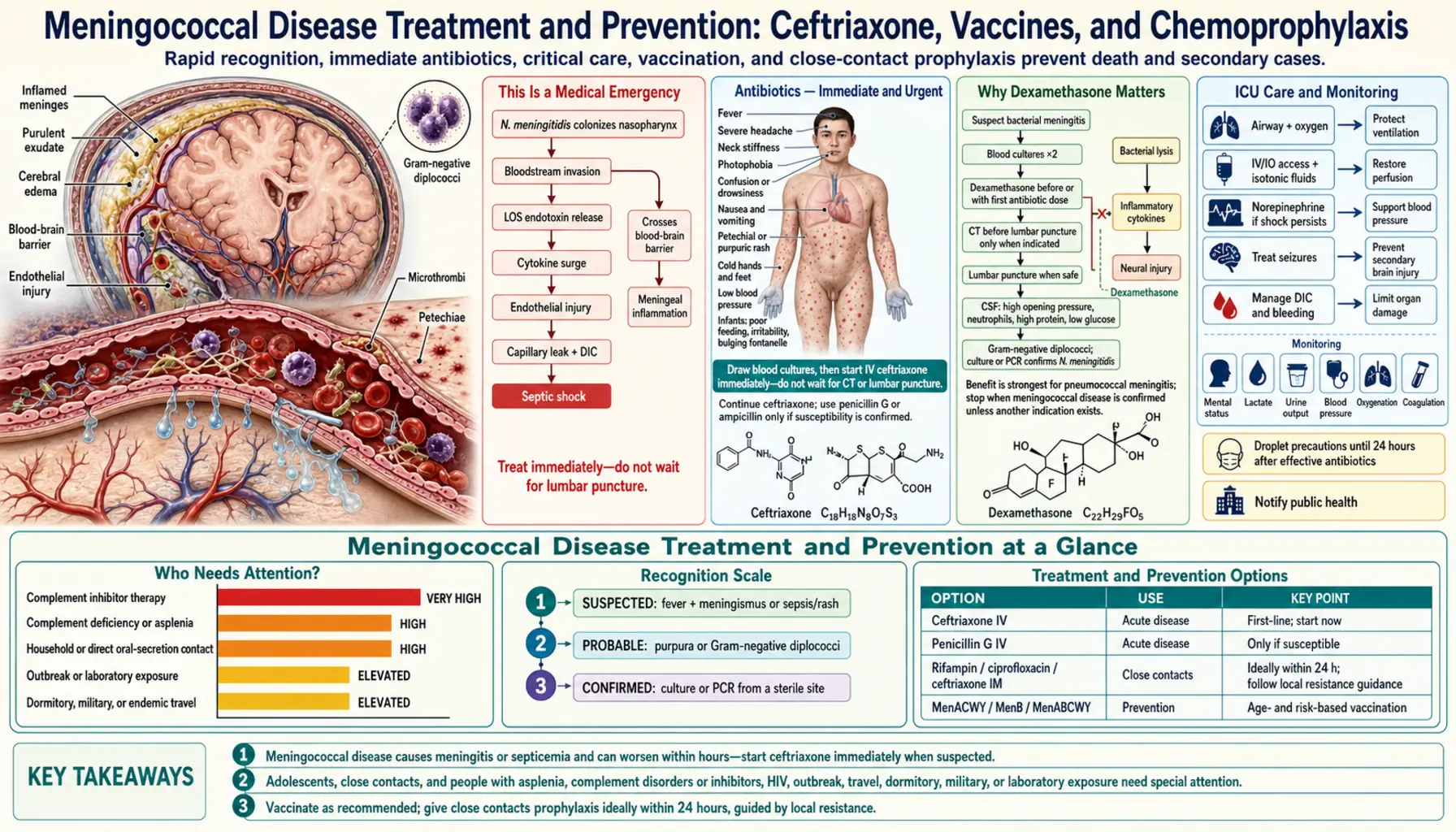
Meningococcal Disease Treatment and Prevention: Ceftriaxone, Vaccines, and Chemoprophylaxis
Meningococcal disease is one of the few bacterial infections that can kill a healthy young person in less than 24 hours. The speed of treatment is the single most important factor determining whether a patient lives, and whether they survive without permanent damage. This page explains the three pillars of treatment — antibiotics, anti-inflammatory steroids, and intensive care — plus how to protect the people around the patient and prevent the disease from striking in the first place.
- This Is a Medical Emergency
- Antibiotics — Immediate and Urgent
- Why Dexamethasone Matters
- ICU Care and Monitoring
- Chemoprophylaxis — Protecting Household Contacts
- Meningococcal Vaccines — the Best Prevention
- Who Needs Vaccines Urgently
- Managing Long-Term Complications
- What to Do If You Are a Household Contact
- Key Research Papers
- Connections
This Is a Medical Emergency
Meningococcal disease can move from first symptoms to death in under 24 hours. In children, it can progress even faster — a child who is unwell at breakfast can be in septic shock by noon. There is no time to wait and see.
If meningococcal disease is suspected — a stiff neck, sensitivity to light, a rash that does not fade under pressure, altered consciousness, or sudden severe headache — the single most important action is to give intravenous (IV) ceftriaxone as fast as possible. You do not need to wait for blood results. You do not need to wait for a lumbar puncture. Treat first, confirm later.
The three pillars of treatment are:
- Antibiotics: IV ceftriaxone kills the bacteria. Speed of administration is directly linked to survival.
- Dexamethasone: This corticosteroid reduces the violent inflammatory reaction that causes hearing loss, brain damage, and brain swelling. It must be given with or before the first antibiotic dose to be effective.
- Intensive care support: Most patients with meningococcal disease need ICU admission to manage brain pressure, low blood pressure, organ failure, and blood clotting problems.
Studies have shown that every hour of delay in giving antibiotics significantly increases the risk of death. A delay of even six hours roughly doubles mortality compared with treatment given at presentation.
Antibiotics — Immediate and Urgent
The antibiotic of choice for meningococcal disease is ceftriaxone, a third-generation cephalosporin given intravenously. The standard adult dose is 2 grams every 12 hours. For children, the dose is weight-based.
Ceftriaxone is chosen for three reasons:
- It crosses the blood-brain barrier and reaches effective concentrations in the fluid surrounding the brain (cerebrospinal fluid).
- It covers Neisseria meningitidis reliably across all serogroups.
- Because the diagnosis cannot always be confirmed immediately, ceftriaxone also covers other common causes of bacterial meningitis — Streptococcus pneumoniae and (in older adults and immunocompromised patients) Listeria monocytogenes.
If ceftriaxone is unavailable, penicillin G is an acceptable alternative when the organism is known to be penicillin-sensitive. However, because resistance patterns vary and the diagnosis may not yet be confirmed, ceftriaxone remains the safer first choice.
If a patient reports a penicillin allergy, the severity of that allergy matters. A mild skin rash from amoxicillin in childhood is not a contraindication to ceftriaxone. A documented anaphylactic reaction to a penicillin is more concerning, though cross-reactivity between penicillins and third-generation cephalosporins is low (under 2%). In a life-threatening emergency, the risk of withholding antibiotics far outweighs the risk of a cross-reaction.
For detailed dosing regimens, antibiotic duration, and monitoring parameters, see the Antibiotic Treatment sub-article.
Why Dexamethasone Matters
When antibiotics kill meningococcal bacteria, the dying bacteria release large amounts of toxins. The immune system reacts violently, flooding the brain and its surrounding membranes with inflammatory chemicals. This inflammatory surge — not the bacteria themselves — causes much of the permanent damage: hearing loss, brain damage, and increased pressure inside the skull that can herniate the brainstem.
Dexamethasone is a corticosteroid that blunts this inflammatory response. The landmark 2002 New England Journal of Medicine trial by de Gans and van de Beek showed that giving dexamethasone just before or with the first antibiotic dose cut the rate of death from bacterial meningitis by more than half in adults with pneumococcal meningitis, and significantly reduced unfavorable outcomes across all causes of bacterial meningitis.
The timing is critical. Dexamethasone must be given before or simultaneously with the first antibiotic dose. If antibiotics have already been running for several hours, the initial inflammatory surge has already happened. Giving dexamethasone at that point provides little benefit and may suppress the immune response in ways that are no longer helpful.
The standard regimen is dexamethasone 0.15 mg/kg IV every 6 hours for 4 days, starting with the first antibiotic dose. For an average adult, this is typically 10 mg every 6 hours.
Because dexamethasone is most clearly beneficial in pneumococcal meningitis, some guidelines recommend discontinuing it after 24–48 hours if the cause is confirmed as meningococcal. However, in practice, when the diagnosis is not immediately confirmed, most clinicians complete the full 4-day course.
ICU Care and Monitoring
Antibiotics and dexamethasone treat the infection and the inflammatory response, but many patients develop serious complications that require moment-to-moment intensive care management:
- Raised intracranial pressure (ICP): Brain swelling can increase pressure inside the skull to dangerous levels, risking brainstem herniation and death. ICU teams monitor for signs of raised ICP and may use osmotherapy (mannitol or hypertonic saline) or controlled ventilation to manage it.
- Septic shock: Meningococcemia (bacteria in the blood) can cause blood vessels to dilate inappropriately, dropping blood pressure to dangerously low levels. Patients often require IV fluids and vasopressor medications (such as norepinephrine) to maintain blood pressure and organ perfusion.
- Disseminated intravascular coagulation (DIC): Meningococcal endotoxins trigger widespread abnormal clotting inside blood vessels, paradoxically leading to both clotting and bleeding. This is the mechanism behind the purpuric skin rash and the limb amputations that are a devastating complication of severe meningococcemia.
- Adrenal failure: In severe meningococcemia, the adrenal glands can be destroyed by hemorrhage (Waterhouse-Friderichsen syndrome), causing life-threatening adrenal insufficiency that requires replacement corticosteroids.
- Acute kidney injury: Septic shock reduces blood flow to the kidneys; some patients require temporary dialysis.
For a detailed account of ICU management and monitoring protocols, see the Antibiotic Treatment sub-article.
Chemoprophylaxis — Protecting Household Contacts
Meningococcal bacteria live harmlessly in the back of the throat (nasopharynx) of around 10% of the general population at any given time. Most carriers never get sick. But the bacteria can spread to others through prolonged close contact — living together, sharing the same bed, or kissing.
When a case of meningococcal disease is confirmed, everyone who has had close contact with the patient in the preceding 7 days must receive antibiotic prophylaxis — even if they feel completely well. The purpose is to clear any meningococcal bacteria they may be carrying in their throats before those bacteria can cause disease.
Close contacts who require prophylaxis include:
- Everyone living in the same household.
- Anyone who slept in the same building regularly (e.g. a boarding school dormitory).
- Anyone who kissed the patient on the mouth in the preceding week.
- Healthcare workers who performed mouth-to-mouth resuscitation or unprotected intubation.
The preferred antibiotic regimens for prophylaxis are:
- Ciprofloxacin: A single 500 mg oral dose. This is preferred in most adults because it is a single dose with good nasopharyngeal penetration and high efficacy. Not recommended in pregnancy.
- Rifampicin: 600 mg twice daily for 2 days in adults; 10 mg/kg twice daily for 2 days in children over 1 month. Rifampicin is effective but interacts with many medications (including the contraceptive pill) and turns urine and contact lenses orange.
- Ceftriaxone IM: A single intramuscular injection of 250 mg (adults) or 125 mg (children under 15). Safe in pregnancy and in patients who cannot take oral medications.
Prophylaxis should ideally be given within 24 hours of the index case being identified. After 2 weeks, the benefit is much reduced. Public health departments coordinate the identification and contacting of all close contacts.
For full details on resistance patterns and prophylaxis in special populations, see the Chemoprophylaxis sub-article.
Meningococcal Vaccines — the Best Prevention
Vaccination is far more effective than any treatment — it prevents the disease from occurring in the first place. There are two types of meningococcal vaccine, targeting different serogroups of the bacterium:
MenACWY vaccines
These conjugate vaccines protect against serogroups A, C, W, and Y, which together account for the majority of meningococcal disease in the United States outside of serogroup B. In the US, Menactra and Menveo are the two available MenACWY vaccines. Routine vaccination is recommended at age 11–12, with a booster at age 16.
MenB vaccines
Serogroup B meningococcal disease is not covered by MenACWY vaccines because the group B capsular polysaccharide mimics human tissue and cannot be used as a vaccine antigen. Two MenB vaccines are available in the US: Bexsero and Trumenba. These are recommended for certain high-risk groups (see below) and may be given to adolescents aged 16–23 at the doctor's or patient's discretion.
Travel vaccination
Travelers to sub-Saharan Africa (the "meningitis belt") and pilgrims attending the Hajj in Saudi Arabia are at significantly elevated risk of meningococcal disease. MenACWY vaccination is required for Hajj, and strongly recommended for travelers to the meningitis belt, particularly during the dry season (December to June) when outbreaks are most common.
For detailed vaccine schedules, dosing intervals, and efficacy data, see the Meningococcal Vaccines sub-article.
Who Needs Vaccines Urgently
Some people face dramatically higher risks of meningococcal disease than the general population and should be vaccinated with both MenACWY and MenB vaccines regardless of age, and should receive booster doses throughout their lives:
- Complement-deficient patients: The complement system is the immune mechanism that kills Neisseria meningitidis in the bloodstream. People with inherited deficiencies of the terminal complement components (C5, C6, C7, C8, or C9) or properdin have a 1,000-fold higher lifetime risk of meningococcal disease. Eculizumab (a medication that blocks complement component C5, used for rare blood disorders) carries a similar risk and patients taking it must be vaccinated before starting.
- Asplenic patients: The spleen filters encapsulated bacteria from the blood. People without a functioning spleen — either surgically removed or functionally absent (as in sickle cell disease) — cannot clear meningococcal bacteria efficiently and are at high risk of overwhelming infection.
- College freshmen living in dormitories: The combination of close living quarters, new exposure to bacteria from different geographic origins, stress, and irregular sleep makes first-year students in residential halls a recognized high-risk group. Most US states require MenACWY vaccination for college entry.
- Military recruits: The same crowding and stress factors apply. Meningococcal outbreaks in military barracks were historically a serious problem before routine vaccination was introduced.
- HIV-positive individuals: HIV impairs the immune response, including complement function and antibody-mediated immunity, increasing susceptibility.
- Travelers to high-risk regions: See above.
Managing Long-Term Complications
Many survivors of meningococcal disease face significant long-term consequences. Identifying and managing these early greatly improves outcomes:
Hearing loss
Bacterial meningitis is one of the most common causes of acquired deafness in children. The inflammatory process in the fluid surrounding the brain damages the cochlea — the hearing organ. Damage can occur rapidly during the acute illness. Every patient who has recovered from bacterial meningitis should have a formal audiological assessment before or shortly after hospital discharge. Cochlear implants can restore hearing in children who lose it to meningitis, but the window for implantation narrows as the cochlea can ossify (fill with bone) within weeks of infection.
Limb loss and skin grafting
Severe meningococcemia can destroy tissue in the hands, feet, and legs through DIC and blood vessel inflammation. Some patients — particularly children — require amputation of fingers, toes, or limbs. Rehabilitation is intensive and long-term, involving prosthetics, occupational therapy, and physiotherapy. Skin grafting may be needed where the purpuric rash caused extensive tissue death.
Neurological complications
Brain damage from meningitis can cause cognitive difficulties, memory problems, learning disabilities, and behavioral changes, particularly in children. These may not be apparent immediately after discharge and can emerge over months. Neuropsychological testing and educational support are important follow-up steps.
Psychological impact
Post-traumatic stress disorder is common among meningococcal disease survivors and their families. Parents who watched a child deteriorate rapidly — often in a matter of hours — frequently experience significant psychological distress. Psychological support, including counseling and peer support groups, should be offered as a routine part of follow-up care.
Other complications
Adrenal insufficiency (from Waterhouse-Friderichsen syndrome), chronic renal impairment, arthritis, and eye inflammation (uveitis) can all occur as sequelae of meningococcal disease. Regular review by a specialist familiar with post-meningococcal complications helps identify and manage these.
What to Do If You Are a Household Contact
If someone in your household or someone you have kissed has been diagnosed with meningococcal disease, do not wait to see if you feel unwell. Take these steps immediately:
- Contact your GP, local health department, or an emergency clinic today. Tell them you have been identified as a close contact of a confirmed meningococcal case. They will arrange antibiotic prophylaxis for you, usually within 24 hours.
- Get the antibiotic prophylaxis. Even if you feel completely well, take the full course or dose. You may be carrying the bacteria in your throat without any symptoms at all.
- Get vaccinated if you have not been vaccinated recently or if your vaccines are not up to date. Prophylactic antibiotics clear current carriage, but they do not protect you from future exposure. Vaccination does.
- Monitor yourself and family members closely for 10 days after exposure. Secondary cases — while uncommon — can occur. Know the warning signs: sudden high fever, severe headache, stiff neck, sensitivity to light, a rash that does not fade when pressed with a glass (the "glass test"). If any of these appear, call emergency services immediately — do not drive yourself to the hospital.
- Do not share the story publicly in ways that identify the patient without their consent. Public health departments will handle formal notification of other contacts in a controlled way.
The risk to a household contact who receives prophylaxis is very low. The antibiotic clears nasopharyngeal carriage reliably in over 90% of cases. The greater risk is to contacts who are not identified and do not receive prophylaxis.
Key Research Papers
- Tunkel AR, et al. Practice guidelines for the management of bacterial meningitis. Clin Infect Dis. 2004;39(9):1267–84. PMID 15494903
- de Gans J, van de Beek D. Dexamethasone in adults with bacterial meningitis. N Engl J Med. 2002;347(20):1549–56. PMID 12432041
- Proulx N, et al. Delays in the administration of antibiotics are associated with mortality from adult acute bacterial meningitis. QJM. 2005;98(4):291–8. PMID 15760921
- Brouwer MC, Tunkel AR, van de Beek D. Epidemiology, diagnosis, and antimicrobial treatment of acute bacterial meningitis. Clin Microbiol Rev. 2010;23(3):467–492. PMID 20610819
- Stephens DS, et al. Epidemic meningitis, meningococcaemia, and Neisseria meningitidis. Lancet. 2007;369(9580):2196–2210. PMID 17604802
- Rosenstein NE, et al. Meningococcal disease. N Engl J Med. 2001;344(18):1378–1388. PMID 11333996
- Cohn AC, et al. Prevention and control of meningococcal disease: recommendations of ACIP. MMWR Recomm Rep. 2013;62(RR-2):1–28. — Search PubMed
- Tan LK, Carlone GM, Borrow R. Advances in the development of vaccines against Neisseria meningitidis. N Engl J Med. 2010;362(16):1511–20. PMID 20410516
- Edmond K, et al. Global and regional risk of disabling sequelae from bacterial meningitis. Lancet Infect Dis. 2010;10(5):317–28. PMID 20417414
- Zalmanovici Trestioreanu A, et al. Antibiotics for preventing meningococcal infections. Cochrane Database Syst Rev. 2011;(8):CD004785. — Search PubMed
- Welch SB, Nadel S. Treatment of meningococcal infection. Arch Dis Child. 2003;88(7):608–14. PMID 12818909
Connections
- Antibiotic Treatment: Ceftriaxone and Dexamethasone
- Meningococcal Vaccines
- Chemoprophylaxis and Antibiotic Resistance
- Symptoms and Diagnosis Hub
- Neisseria Meningitidis Overview
- Meningitis
- Sepsis
- All Bacteria