Meningococcemia and Purpura Fulminans: Sepsis and the Non-Blanching Rash
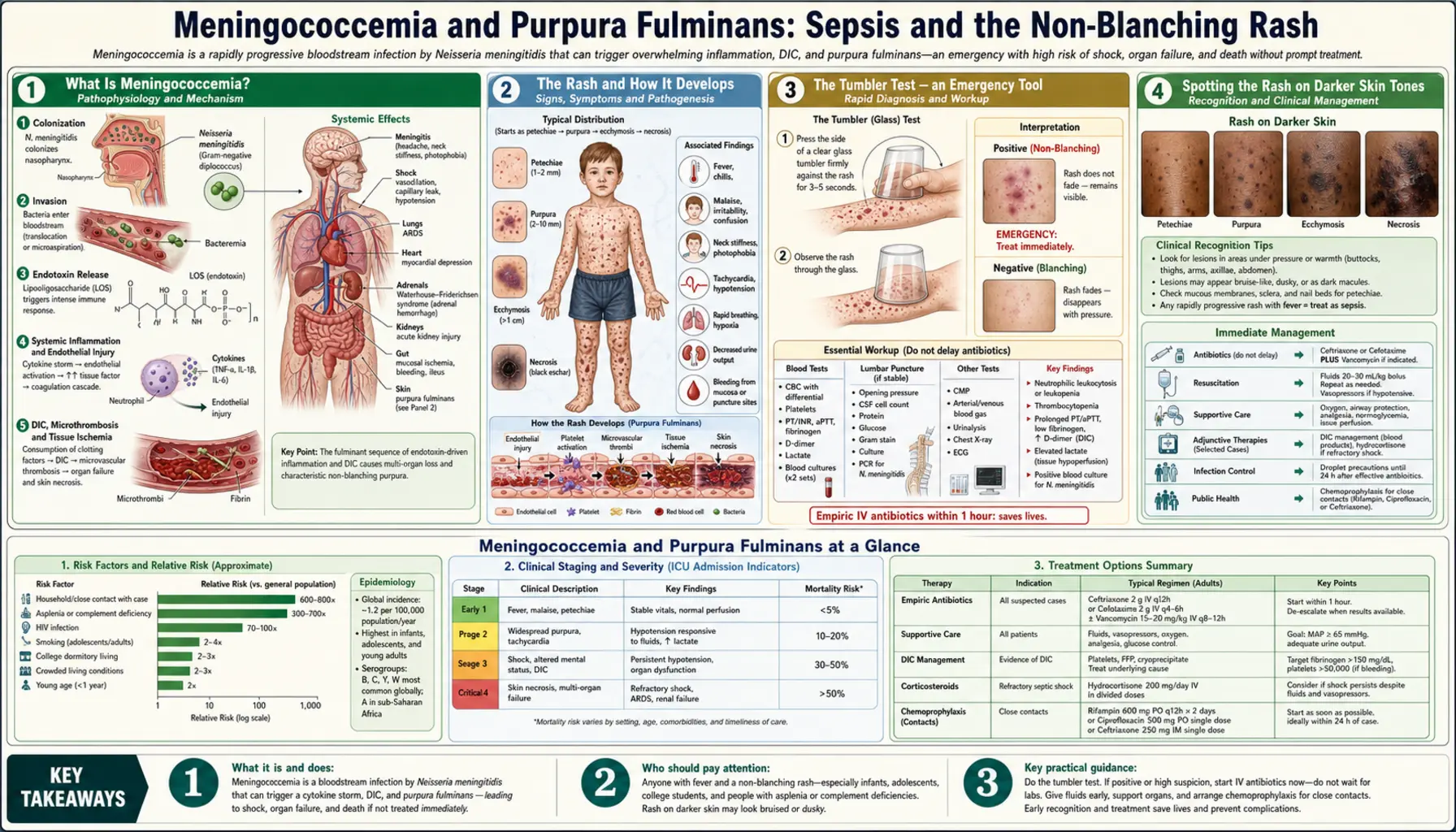
Table of Contents
- What Is Meningococcemia?
- The Rash and How It Develops
- The Tumbler Test — an Emergency Tool
- Spotting the Rash on Darker Skin Tones
- Pathophysiology of Purpura Fulminans
- Waterhouse-Friderichsen Syndrome
- Limb Ischaemia and Amputation
- Managing Septic Shock — What Happens in the ICU
- Outcomes With and Without Treatment
- Key Research Papers
- Connections
- Featured Videos
What Is Meningococcemia?
Meningococcemia — sometimes written as meningococcaemia — is the form of meningococcal disease in which Neisseria meningitidis multiplies in the bloodstream itself. This is distinct from meningitis, where the primary site of infection is the brain's surrounding membranes. Meningococcemia can occur without meningitis, with meningitis, or it can progress to a combined picture. When it occurs without meningitis, the disease can be even more rapidly lethal, because there is no blood-brain barrier to slow the pace of bacterial multiplication and there may be no warning headache or neck stiffness to prompt early concern.
The driver of the system-wide disaster in meningococcemia is the bacterial outer membrane, specifically a toxic molecule called lipooligosaccharide (LOS) — essentially an endotoxin. As bacteria multiply and die in the bloodstream, they release LOS in large quantities. LOS binds to receptors on immune cells, triggering a massive, dysregulated inflammatory response that spirals far beyond what is needed to kill the bacteria. This systemic inflammatory cascade is the engine driving the catastrophic decline.
The Rash and How It Develops
The characteristic rash of meningococcemia is one of the most recognisable — and most feared — in medicine. Understanding how it develops helps explain why it looks the way it does and why it signals such danger.
The rash begins as petechiae — tiny, 1-2 millimetre flat spots that are red or dark purple, looking like pinpoint bruises. They most commonly appear first on the trunk, ankles, and wrists. These tiny spots are caused by blood leaking out of small damaged blood vessels (capillaries) into the skin tissue — a sign that the coagulation system is already failing.
As the disease progresses, petechiae enlarge and coalesce into larger, irregular patches called purpura. These look like bruises but are not caused by injury — they are caused by widespread haemorrhage into the skin from blood vessels destroyed by the inflammatory storm. The progression from petechiae to purpura can be dramatic: some patients develop new spots every few minutes during the acute phase. The rate of spread of the rash across the body is itself a clinical indicator of disease severity — rapid spread correlates with more severe DIC and worse outcomes.
In the most severe form, purpura fulminans develops: large areas of skin and underlying tissue undergo complete necrosis (death) as the blood supply is cut off. These areas turn black, become necrotic, and are unmistakable signs of impending tissue loss.
The Tumbler Test — an Emergency Tool
The tumbler test (also called the "glass test") is a simple tool that anyone — not just medical professionals — can use to identify a non-blanching rash in a febrile person. The principle is based on a fundamental property of blood that has leaked out of blood vessels versus blood that is simply in dilated capillaries close to the skin surface.
Here is how to perform it:
- Take a clear glass tumbler or drinking glass — the clearer the better.
- Press the glass firmly and flatly against the rash, pressing hard enough to squeeze the blood out of normal skin capillaries.
- While pressing, look through the glass at the spots.
A blanching rash — found in the vast majority of rashes, including viral rashes — turns white under the glass. The pressure forces blood out of the dilated capillaries, and the skin pales. When you release the pressure, the colour returns. This is reassuring.
A non-blanching rash does not change colour at all. The spots remain visible because the blood is not inside capillaries that can be compressed — it is already outside the blood vessels, in the skin tissue itself. You cannot compress blood that is no longer in a vessel. A non-blanching rash in a febrile person is a medical emergency. Call 999 or 911 immediately.
Do NOT wait to see if more spots develop. Do NOT wait until morning. If the rash does not blanch under the glass, call emergency services now.
Spotting the Rash on Darker Skin Tones
A critically important and historically under-discussed aspect of meningococcal rash recognition is that petechiae and purpura can be very difficult or impossible to see on darker skin tones, particularly in artificial lighting. The classic descriptions of "red or purple spots on fair skin" are essentially useless for families and clinicians working with patients of African, South Asian, Middle Eastern, or other backgrounds with darker skin pigmentation.
Several strategies can help:
- Use natural daylight if possible — the colour contrast is better than under incandescent or fluorescent lighting.
- Check mucous membranes — look inside the lips and along the gumline, and look at the inner surface of the lower eyelids (conjunctivae). These areas have a thin overlying epithelium and less melanin, so petechiae are visible as tiny dark or red spots even on very dark skin.
- Check palms and soles — the palms of the hands and soles of the feet have a thinner melanin-containing layer, and petechiae may be visible here when they are invisible elsewhere on the body.
- Check the nail beds — look under the fingernails and toenails for dark discolouration.
Any tiny dark spots on these areas in a febrile, unwell person warrant immediate emergency evaluation. If in doubt, call emergency services. A false alarm is always better than a missed diagnosis.
Pathophysiology of Purpura Fulminans
Purpura fulminans is the most extreme expression of DIC — disseminated intravascular coagulation — triggered by the meningococcal endotoxin. Understanding it requires understanding DIC, which is one of the most paradoxical and deadly processes in medicine.
Under normal circumstances, coagulation (blood clotting) is a localised, carefully controlled response to blood vessel injury — the body forms a clot to plug a wound and then dissolves it when healing is complete. In DIC triggered by meningococcal endotoxin, this system is activated in an uncontrolled, system-wide way. The endotoxin (LOS) triggers the simultaneous activation of the entire clotting cascade throughout every blood vessel in the body, while also triggering massive inflammation.
Two catastrophic processes happen simultaneously:
- Microthrombosis — countless tiny clots form in small blood vessels throughout the body. These clots block circulation to the tissues they supply. Skin, muscle, and organs begin to starve of oxygen. This is what causes the tissue necrosis of purpura fulminans and the organ failure of severe septic shock.
- Consumption coagulopathy — the clotting system uses up its clotting factors and platelets so rapidly and completely that it exhausts them. The person is simultaneously clotting everywhere AND running out of the ability to clot. The result is paradoxical bleeding — despite the clotting that is happening, the consumed platelets and clotting factors mean the person also bleeds from IV lines, mucous membranes, and into tissues.
This paradox — clotting and bleeding at the same time, in the same body — is why DIC is so difficult to treat and why purpura fulminans carries such high mortality.
Waterhouse-Friderichsen Syndrome
Waterhouse-Friderichsen syndrome is a specific complication of severe meningococcemia in which both adrenal glands undergo massive haemorrhage and infarction (tissue death). It was first described independently by British physician Rupert Waterhouse (1911) and Danish physician Carl Friderichsen (1918) and remains one of the most dramatic pathological findings in meningococcal disease.
The adrenal glands — small triangular organs that sit on top of each kidney — are particularly vulnerable to the effects of DIC because they have an "end-arterial" blood supply: the blood supply to the inner part of the adrenal gland comes from a single set of small arteries with no backup supply from a different direction. When DIC causes microthrombosis in these vessels, the entire gland can infarct simultaneously, and haemorrhage fills the necrotic tissue.
The clinical consequence is acute adrenal crisis — a sudden, complete failure of adrenal hormone production. The adrenal glands produce cortisol (essential for maintaining blood pressure and responding to stress) and aldosterone (essential for maintaining sodium balance and blood volume). Loss of these hormones in the context of severe septic shock creates a clinical picture of refractory hypotension — blood pressure that cannot be maintained despite large volumes of IV fluids. Recognising Waterhouse-Friderichsen syndrome and treating it with urgent intravenous corticosteroids (hydrocortisone) is essential and can be life-saving.
Limb Ischaemia and Amputation
One of the most devastating long-term consequences of severe meningococcemia is the loss of limbs — or parts of limbs — to ischaemic necrosis driven by purpura fulminans. This complication occurs in a subset of survivors of the most severe meningococcemic disease and can result in the need for single or multiple amputations.
The areas most commonly affected are those with relatively poor blood supply and limited collateral circulation: fingers, toes, the nose, and the ears. As DIC occludes the micro-vessels supplying these tissues, the tissue becomes starved of oxygen. Over hours and days, the affected areas progress from pale and cold, to blue-grey, to black — a progression from ischaemia to infarction to gangrene.
The management of this complication involves an agonising period of clinical assessment. Surgeons must wait until the boundary between viable and non-viable tissue has demarcated clearly — often taking days to weeks — before proceeding to surgical debridement or amputation. Operating too early risks removing tissue that might have been salvageable; waiting too long risks systemic infection from the dead tissue. The decision requires specialist surgical input and carries profound physical and psychological consequences for the patient.
Even with excellent intensive care, limb loss occurs in some patients with severe purpura fulminans. This is not a failure of care — it is the consequence of a disease process that sometimes cannot be stopped in time, even when treatment is started promptly. Rehabilitation services, prosthetic limbs, and psychological support are essential parts of long-term care for these patients.
Managing Septic Shock — What Happens in the ICU
The immediate management of meningococcemic septic shock is an orchestrated intensive care effort targeting several simultaneous problems:
- IV fluid resuscitation — large volumes of crystalloid (normal saline or balanced salt solutions) are given rapidly to restore circulating blood volume: typically 20-30mL per kilogram of body weight in boluses, with assessment after each bolus. Over-resuscitation can worsen outcomes by diluting clotting factors and causing fluid overload in the lungs.
- Vasopressors — when blood pressure cannot be maintained with fluids alone, vasopressors are added. Norepinephrine (noradrenaline) is the first-line agent; it constricts blood vessels to maintain perfusion pressure to vital organs. Vasopressin is added in refractory cases.
- Corticosteroids — IV hydrocortisone is given in patients with features of adrenal insufficiency or in those whose shock is not responding adequately to vasopressors; this is essential in Waterhouse-Friderichsen syndrome.
- Managing DIC — fresh frozen plasma (FFP) provides replacement clotting factors consumed by DIC; platelet transfusions are given when platelet counts fall dangerously low; cryoprecipitate provides fibrinogen. These measures partially compensate for the ongoing consumption without treating its underlying cause.
- Monitoring — an arterial line (a thin tube placed in a wrist artery) provides continuous blood pressure monitoring and easy blood sampling; a central venous catheter measures central venous pressure; urine output via a urinary catheter tracks renal perfusion; regular blood tests monitor organ function, blood counts, and clotting.
- ECMO — extracorporeal membrane oxygenation, a machine that takes over the function of the heart and lungs, is considered in the most refractory cases of septic shock that do not respond to maximal conventional treatment. Its use in meningococcal disease remains rare but has been reported in individual case series.
Outcomes With and Without Treatment
The contrast between treated and untreated meningococcemia is stark. Without antibiotic treatment, meningococcemia is one of the most lethal acute infections known — historical series from the pre-antibiotic era describe fatality rates approaching or exceeding 80-90% in the most severe septicaemic form.
With modern intensive care in a high-income setting, overall case fatality rates for all forms of meningococcal disease (including the less severe forms) are approximately 10-15%. For the pure septicaemia form — the most dangerous — mortality rates are typically higher, in the range of 15-25% even with optimal care. These figures represent real people who die despite receiving the best available treatment; meningococcemia remains one of the most challenging acute sepsis syndromes in intensive care.
Permanent sequelae occur in an additional 10-20% of survivors: limb loss, skin necrosis requiring grafting, hearing loss, cognitive changes, and psychological trauma. Prompt treatment — particularly rapid antibiotic administration before the bacterial burden becomes overwhelming — remains the single most important modifiable factor determining whether a patient lives and what long-term consequences they face. Every hour without antibiotics allows bacterial numbers, endotoxin release, and organ damage to compound. This is why early recognition and early treatment cannot be overstated.
Key Research Papers
- Brandtzaeg P, et al. Plasma endotoxin as a predictor of multiple organ failure and death in systemic meningococcal disease. J Infect Dis. 1989;159(2):195-204. — Search PubMed
- van Deuren M, Brandtzaeg P, van der Meer JW. Update on meningococcal disease with emphasis on pathogenesis and clinical management. Clin Microbiol Rev. 2000;13(1):144-66. PMID 10627495
- Stephens DS, et al. Epidemic meningitis, meningococcaemia, and Neisseria meningitidis. Lancet. 2007;369(9580):2196-2210. PMID 17604802
- Riordan FA, et al. Admission cortisol and adrenocorticotrophic hormone levels in children with meningococcal disease. Arch Dis Child. 1999;80(5):438-40. — Search PubMed
- Rosenstein NE, et al. Meningococcal disease. N Engl J Med. 2001;344(18):1378-1388. PMID 11333996
- Welch SB, Nadel S. Treatment of meningococcal infection. Arch Dis Child. 2003;88(7):608-14. PMID 12818909
- Lerolle N, et al. Histopathology of septic shock induced acute kidney injury: apoptosis and leukocytic infiltration. Intensive Care Med. 2010;36(3):471-8. — Search PubMed
- Voss LM, et al. Mortality and morbidity of meningococcal disease. J Paediatr Child Health. 2003;39(5):355-9. PMID 12887668
- Parrillo JE. Pathogenetic mechanisms of septic shock. N Engl J Med. 1993;328(20):1471-7. PMID 8479467
- Hermans PW, et al. Derangement of the hemostatic system in patients with severe meningococcal septicemia. Intensive Care Med. 1991;17(5):264-8. — Search PubMed
Connections
- All Bacteria
- Symptoms and Disease Overview
- Bacterial Meningitis Symptoms
- Diagnosis and Lumbar Puncture
- Antibiotic Treatment
- Neisseria meningitidis Overview
- Sepsis