Meningococcal Meningitis: Symptoms and Clinical Presentation
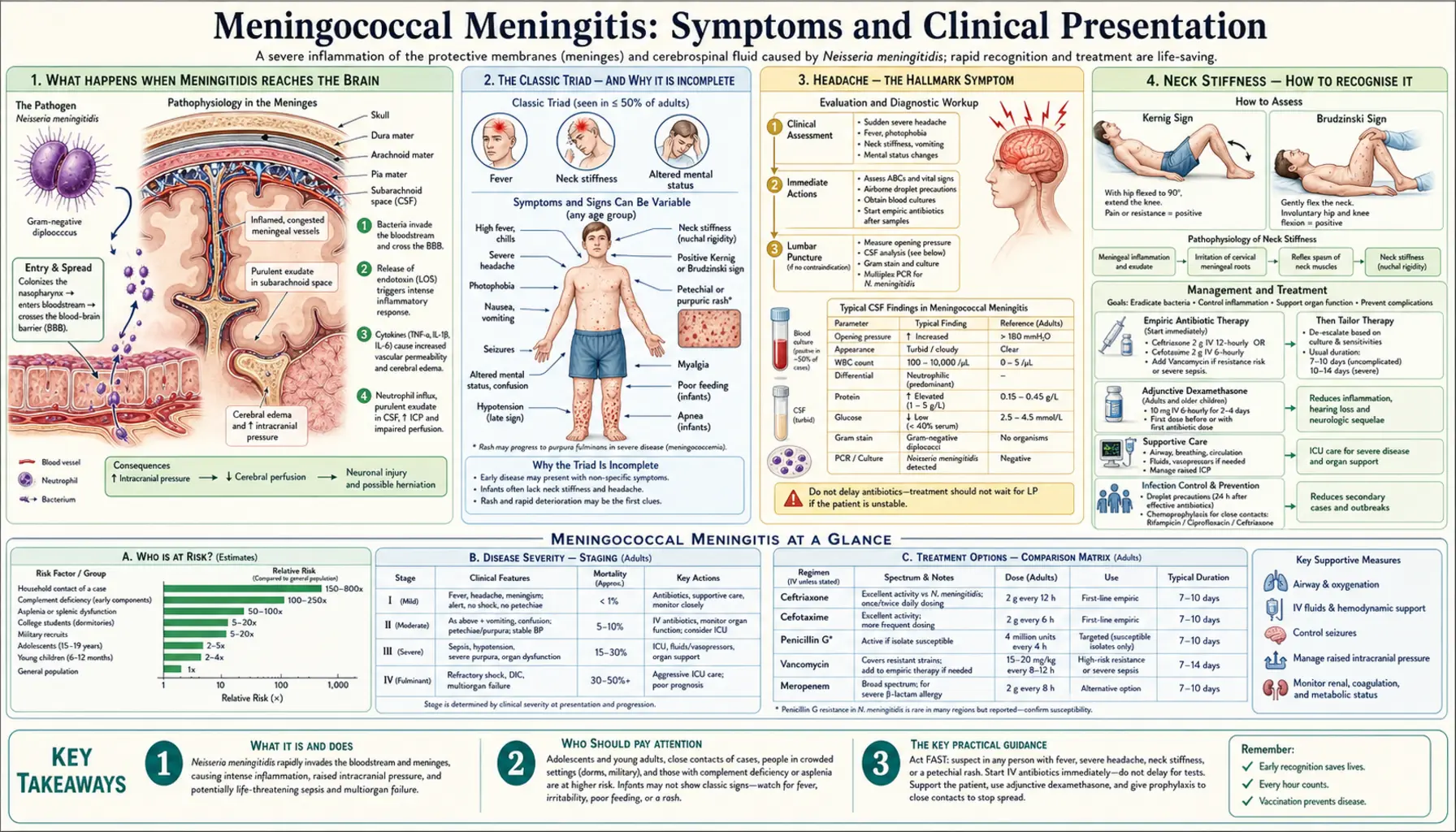
Table of Contents
- What Happens When Meningitidis Reaches the Brain
- The Classic Triad — and Why It Is Incomplete
- Headache — the Hallmark Symptom
- Neck Stiffness — How to Recognise It
- Altered Consciousness — a Sign of Severity
- Seizures in Meningococcal Meningitis
- How Meningitis Looks Different in Infants
- Early Non-Specific Phase — the Most Dangerous Stage
- Long-Term Neurological Sequelae
- Key Research Papers
- Connections
- Featured Videos
What Happens When Meningitidis Reaches the Brain
For Neisseria meningitidis to cause meningitis, it must make a journey that takes it from your throat to your bloodstream to your brain. Starting in the nasopharynx (the back of the throat), bacteria breach the mucosal lining — often helped by preceding viral infections that have damaged this barrier — and enter the bloodstream. From the blood, they must then cross the blood-brain barrier, the highly selective gateway that normally prevents most bacteria from entering the brain.
Exactly how the meningococcus crosses the blood-brain barrier is still an area of active research, but it appears to involve interactions between bacterial surface proteins and receptors on the cells lining the brain's blood vessels. Once inside the cerebrospinal fluid (CSF) — the fluid that cushions the brain and spinal cord — the bacterium finds itself in an environment almost devoid of immune cells. The CSF normally has very few white blood cells, and antibody levels are low. The bacterium can multiply rapidly and largely unchallenged for a short but critical period.
When the immune system does mount a response — sending white blood cells flooding into the CSF and releasing inflammatory chemicals — the resulting inflammation causes swelling of the brain's covering membranes (the meninges). This inflammation, paradoxically, is part of what makes meningitis so dangerous: the inflammatory response that is trying to kill the bacteria also damages neurons, disrupts the blood-brain barrier further, and raises intracranial pressure to dangerous levels. It is this raised pressure inside the rigid skull — squeezing the brain — that drives many of the most serious complications.
The Classic Triad — and Why It Is Incomplete
Medical textbooks describe the "classic triad" of bacterial meningitis as fever, severe headache, and neck stiffness. This triad is important to know, but it is also critically important to know its limitations: in adults, all three features are present simultaneously in fewer than half of patients at the time they first seek care. In children under 2, the classic triad is often completely absent.
This does not mean meningitis is rare in someone without the full triad. It means that waiting for all three features to develop before taking action is dangerous. Clinicians are taught to have a low threshold for investigating any patient with fever and headache, particularly when the headache is severe and sudden in onset. The absence of neck stiffness should never be used to reassure either a doctor or a worried parent that meningitis has been ruled out.
Headache — the Hallmark Symptom
The headache of meningitis is characteristically severe, sudden in onset, and quite different from ordinary tension headaches. Patients often describe it as "the worst headache of my life" — a description that also features in subarachnoid haemorrhage (bleeding around the brain) and should always trigger urgent investigation. Some describe it as feeling like someone has hit the back of their head with a bat, often with an abrupt, explosive onset.
The headache is typically bifrontal (across the forehead) or global (felt everywhere in the head). It is not relieved by ordinary over-the-counter painkillers like paracetamol or ibuprofen. Two features that frequently accompany the headache are particularly characteristic:
- Photophobia — the eyes become intensely sensitive to normal levels of light, which causes significant pain. Even a normally lit room feels unbearably bright. Patients instinctively cover their eyes or seek darkness.
- Phonophobia — sensitivity to normal sounds, which also cause pain. A normally quiet environment feels unbearably loud. Patients ask for quiet and avoid noise.
These features reflect irritation of the meninges — even the vibrations caused by sound and the reflex pupil changes triggered by light cause pain when the meninges are inflamed.
Neck Stiffness — How to Recognise It
Neck stiffness in meningitis — known medically as nuchal rigidity — is a physical sign caused by irritation and spasm of the muscles in the back of the neck. When meningeal inflammation spreads down the spinal cord, stretching the inflamed meninges by moving the neck becomes extremely painful, so the neck muscles go into protective spasm to prevent that movement.
To check for nuchal rigidity in a conscious patient, ask them to try to bring their chin to rest on their chest. A healthy person can do this easily. Someone with significant nuchal rigidity cannot — either because it is too painful or because the muscle spasm physically prevents the movement. This is not a subtle finding in a fully developed case; it is often strikingly obvious.
Two classical clinical signs that emergency doctors look for are:
- Kernig's sign — with the patient lying on their back and the hip bent to 90 degrees, the examiner tries to straighten the knee. In a patient with meningeal irritation, this stretches the inflamed spinal meninges and causes pain, so the patient resists the movement. Kernig's sign is positive in approximately 50% of bacterial meningitis cases — so a negative result does not rule it out.
- Brudzinski's sign — when the examiner passively flexes the patient's neck (brings chin to chest), meningeal irritation causes the patient to involuntarily flex both hips and knees. Like Kernig's sign, it has sensitivity of around 50% and therefore should not be used to exclude meningitis if other features are present.
Altered Consciousness — a Sign of Severity
A change in the level of consciousness — confusion, disorientation, difficulty waking, or unresponsiveness — is a marker of severe meningococcal disease. It indicates that the raised intracranial pressure is directly affecting brain function, or that the brain itself is being damaged by the infection. This should be treated as an emergency sign requiring immediate escalation of care.
Medical teams use the Glasgow Coma Scale (GCS) to quantify the level of consciousness: it scores eye opening, verbal response, and motor response on a scale of 3 (completely unresponsive) to 15 (fully alert). A GCS below 9 indicates severe disease and signals the need for ICU-level care, often including intubation to protect the airway and manage intracranial pressure.
Altered consciousness in meningitis can result from several overlapping mechanisms: raised intracranial pressure squeezing the brain, direct brain invasion by bacteria in some cases, hypoglycaemia (low blood sugar, because the infection consumes glucose), electrolyte disturbances, or cerebral vasculitis (inflammation of brain blood vessels causing small strokes). Managing these simultaneously is one of the challenges of intensive care for meningococcal disease.
Seizures in Meningococcal Meningitis
Seizures occur in 15-30% of patients with bacterial meningitis and may be the first dramatic symptom that prompts emergency attendance. They can occur at any stage of the illness — sometimes before the headache and neck stiffness are obvious, making the diagnosis less immediately clear. A first-ever seizure in a febrile adult or child should always raise the possibility of meningitis.
The immediate management of a seizure in this context is identical to seizure management generally — lorazepam or diazepam intravenously or rectally to stop the seizure — but the critical additional step is treating the underlying meningitis with antibiotics urgently. Seizures in meningitis are more likely when:
- Intracranial pressure is markedly raised
- There are focal areas of brain inflammation or small strokes
- Electrolytes are severely disturbed (particularly low sodium — hyponatraemia, which can itself cause seizures)
Persistent or recurrent seizures that do not respond to initial anticonvulsant therapy are a sign of severe disease and warrant consideration of CT imaging to exclude complications such as cerebral abscess or venous sinus thrombosis.
How Meningitis Looks Different in Infants
In infants — particularly those under 18 months — the classic triad of fever, headache, and neck stiffness can be completely absent, making meningitis one of the most feared diagnoses to miss in paediatrics. Infants cannot report headache. Their soft skulls can accommodate some of the raised intracranial pressure by bulging the fontanelle (the soft spot on top of the head) outward, which means less neck stiffness early on. The immune response differs in young infants, and they may even be hypothermic (cold) rather than feverish, especially in the very young.
Warning signs in infants that should trigger immediate emergency evaluation include:
- Bulging anterior fontanelle — the soft spot at the top of the head is visibly and persistently bulging outward when the baby is upright and calm (a transiently bulging fontanelle during crying is normal)
- High-pitched or unusual cry — a piercing, unusual cry unlike the baby's normal cry; sometimes described as a "moaning" quality
- Paradoxical irritability — the baby cries more when picked up and comforted, rather than being soothed; this is because being held moves the inflamed meninges
- Poor feeding or vomiting — refusing feeds or forceful vomiting
- Seizures — particularly important in febrile infants
- Purple or red spots on the skin — petechiae or purpura in any febrile infant is an emergency
- Extreme pallor or mottled skin — signs of poor circulation
A parent's instinct that something is very wrong with their baby should never be dismissed. Parents know their baby's normal behaviour, and "something is different" is a valid and important clinical data point.
Early Non-Specific Phase — the Most Dangerous Stage
One of the most clinically important features of meningococcal disease is that the first 4-6 hours of illness are often indistinguishable from flu. The patient — or the parent of an affected child — typically reports high fever, shivering or rigors (violent shaking chills), severe generalised aching and pain, and feeling extremely unwell. The distinctive features of meningitis or septicaemia — the neck stiffness, the rash — typically develop later.
This early non-specific phase is when diagnosis is most difficult and, paradoxically, when early treatment would have the greatest impact. Studies of meningococcal deaths in previously healthy children and teenagers consistently find that the initial presentation looked like flu. The window for saving a life — before multi-organ failure, before massive DIC, before brain herniation — is often measured in hours.
For families: the key warning is rapid deterioration. If a person starts with what seems like flu but deteriorates very quickly — getting much worse within hours, developing confusion, developing any rash, or becoming very difficult to rouse — this pattern of rapid deterioration is itself a warning sign of meningococcal disease. Do not wait for the textbook triad. Call emergency services.
Long-Term Neurological Sequelae
Surviving meningococcal meningitis is a beginning, not an end. The neurological consequences can be significant, longlasting, and life-altering:
- Sensorineural hearing loss — affects 10-15% of survivors. Bacteria and inflammatory mediators enter the inner ear through the cochlear aqueduct during the acute infection, damaging the hair cells of the cochlea. The loss is typically bilateral and permanent. Every survivor of bacterial meningitis should have formal audiological assessment, as hearing aids or cochlear implants may be needed. Children who suffer hearing loss as a result of meningitis may require specialist educational support.
- Brain damage and cognitive changes — raised intracranial pressure causes areas of ischaemia (loss of blood supply) in the brain; bacteria may invade brain tissue directly; inflammation causes cytokine-mediated neuronal injury. Survivors may have ongoing memory problems, difficulty concentrating, slower processing speed, and changes in behaviour or personality. These may not be apparent immediately on hospital discharge and can emerge over the weeks and months of recovery. Children may be at risk of learning difficulties and may need educational assessment and support.
- Hydrocephalus — in some cases, inflammation causes blockage of the normal circulation of CSF, leading to its accumulation (hydrocephalus). This may require surgical placement of a ventricular drain or a permanent shunt.
- Focal neurological deficits — depending on which parts of the brain have been affected by infarction or direct inflammation, survivors may have persistent weakness of a limb, visual field defects, or other focal problems.
- Psychological sequelae — PTSD is common after the sudden, terrifying illness course and ICU treatment, in both survivors and their family members.
Key Research Papers
- van de Beek D, et al. Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med. 2004;351(18):1849-59. — Search PubMed
- Attia J, et al. Does this adult patient have acute meningitis? JAMA. 1999;282(2):175-81. PMID 10411200
- Brouwer MC, Tunkel AR, van de Beek D. Epidemiology, diagnosis, and antimicrobial treatment of acute bacterial meningitis. Clin Microbiol Rev. 2010;23(3):467-492. PMID 20610819
- Rosenstein NE, et al. Meningococcal disease. N Engl J Med. 2001;344(18):1378-1388. PMID 11333996
- Stephens DS, et al. Epidemic meningitis, meningococcaemia, and Neisseria meningitidis. Lancet. 2007;369(9580):2196-2210. PMID 17604802
- Thigpen MC, et al. Bacterial meningitis in the United States, 1998-2007. N Engl J Med. 2011;364(21):2016-25. PMID 21612470
- Edmond K, et al. Global and regional risk of disabling sequelae from bacterial meningitis. Lancet Infect Dis. 2010;10(5):317-28. PMID 20417414
- Pomeroy SL, Holmes SJ, Dodge PR, Feigin RD. Seizures and other neurologic sequelae of bacterial meningitis in children. N Engl J Med. 1990;323(24):1651-7. — Search PubMed
- Bedford H, de Louvois J, Halket S, et al. Meningitis in infancy in England and Wales. BMJ. 2001;323(7312):533-6. — Search PubMed
- Weisfelt M, et al. Pneumococcal meningitis in adults: new approaches to management and prevention. Lancet Neurol. 2006;5(4):332-42. PMID 16545749
Connections
- All Bacteria
- Symptoms and Disease Overview
- Meningococcemia and Purpura Fulminans
- Diagnosis and Lumbar Puncture
- Antibiotic Treatment
- Neisseria meningitidis Overview
- Meningitis
- Encephalitis