Rapamycin: History and Origins
Rapamycin is one of the rare drugs whose origin story can be told almost like an adventure: a soil sample scooped from the ground beneath the giant stone heads of Easter Island, a curious antibiotic that nobody quite knew what to do with, and a stubborn scientist who hid the bacteria in his home freezer to keep his company from destroying them. This article traces what the historical record actually supports — the 1964 Canadian expedition to Rapa Nui, the isolation of the molecule at Ayerst Laboratories in the early 1970s, the life and persistence of Suren Sehgal (1932–2003), the surprise discovery that the antifungal was a powerful immune suppressant, the unraveling of the mTOR pathway it acts on, its approval as a transplant drug in 1999, and its more recent and still investigational turn toward longevity. Where the record is firm we say so; where a claim is disputed, promotional, or unproven we name it as such. Rapamycin's use to slow human aging is experimental and not approved by any regulator — that honesty is part of the story too.
Table of Contents
- A Soil Sample from Easter Island (1964)
- Isolation and the Naming of Rapamycin (early 1970s–1975)
- Suren Sehgal: The Man and the Freezer
- From Antifungal to Immune Suppressant
- Discovering the Target: TOR and mTOR
- Rapamune: Approval and the Rapalogs (1999 onward)
- The Longevity Turn (2009 to Today)
- Evidence, Ethics, and Honest Reception
- Research Papers and References
- Connections
- Featured Videos
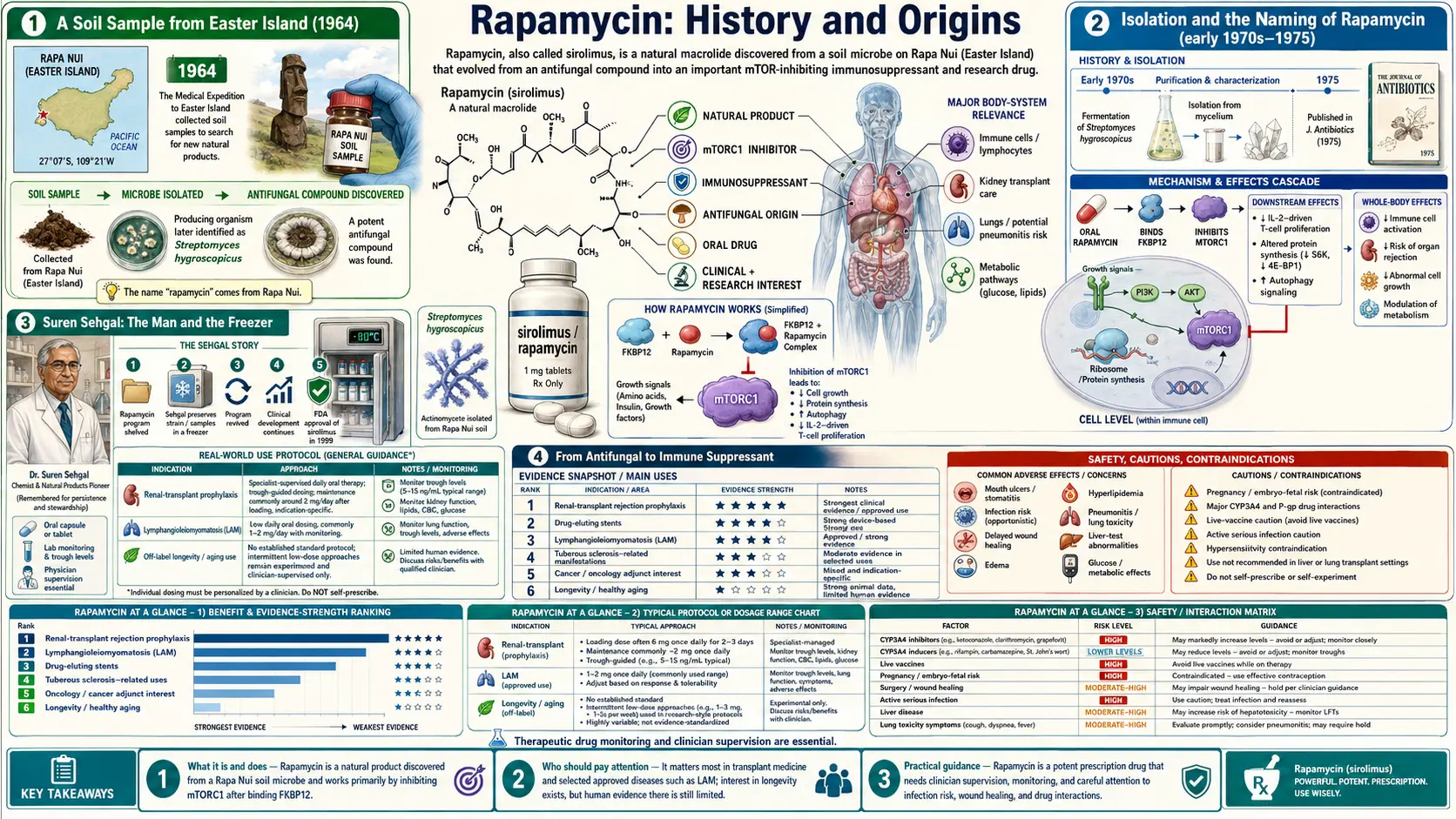
A Soil Sample from Easter Island (1964)
The story begins not in a laboratory but on one of the most remote inhabited places on Earth. In 1964, a Canadian-led scientific and medical expedition — later known by the acronym METEI, the Medical Expedition to Easter Island — traveled to Rapa Nui (Easter Island) aboard the naval vessel HMCS Cape Scott. The expedition's purpose was broadly to study the health of the island's isolated population before a planned airport ended that isolation, but one of its lasting legacies came from the dirt under everyone's feet.
Among the team was a Montreal microbiologist named Georges Nogrady (1919–2013), of the University of Montreal. Nogrady systematically collected soil samples from across the island. Those samples eventually made their way to the pharmaceutical company Ayerst Laboratories in Montreal, where they were screened for microbes that might produce useful antibiotics — a standard practice in an era when soil bacteria were the richest known source of new drugs (penicillin, streptomycin, and many others had all come from microbes). One Easter Island sample harbored a bacterium that would prove unusually valuable.
It is worth pausing on a fact that later commentators have raised honestly: the molecule that grew out of that soil would one day become a globally important medicine and a multi-million-dollar product, yet the Indigenous Rapa Nui people on whose land it was found shared in none of that value. This is now discussed as an early and much-cited example of the ethics of benefit-sharing in bioprospecting, and it belongs in any complete telling of the history rather than being airbrushed out.
Isolation and the Naming of Rapamycin (early 1970s–1975)
At Ayerst, scientists isolated from the Easter Island soil a filamentous soil bacterium, a streptomycete identified as Streptomyces hygroscopicus. From it they extracted a previously unknown compound that strongly inhibited fungi — in laboratory tests it suppressed Candida albicans (a common cause of yeast infections), Microsporum gypseum, and Trichophyton granulosum (skin and ringworm fungi). At first, then, this was simply a promising new antifungal antibiotic.
The team gave it the laboratory code AY-22,989 and, in homage to where its parent bacterium had come from, named it rapamycin — after Rapa Nui, the Polynesian name for Easter Island, joined to the "-mycin" suffix conventional for antibiotics derived from soil actinomycetes. The work was formally published in 1975: Claude Vézina, A. Kudelski, and Suren N. Sehgal described the producing bacterium and the isolation of the active compound in the Journal of Antibiotics, in a paper titled "Rapamycin (AY-22,989), a new antifungal antibiotic. I. Taxonomy of the producing streptomycete and isolation of the active principle," followed by companion papers on its fermentation and characterization.
So the documented birth of rapamycin as a named molecule is firm and datable: a real bacterium, real scientists, a real journal, and the year 1975. What nobody yet realized was that its antifungal activity — the property it was named and described for — would turn out to be almost a footnote next to what it did to the immune system and to the machinery of cellular growth.
Suren Sehgal: The Man and the Freezer
If rapamycin has a single human champion, it is Surendra Nath "Suren" Sehgal (1932–2003). He was born in 1932 in Khushab, in the Punjab of British India (a town now in Pakistan). He earned a Bachelor of Pharmacy (1952) and a Master of Pharmacy (1953) from Banaras Hindu University, then traveled to England and completed a Ph.D. in microbiology at the University of Bristol in 1957. After a postdoctoral fellowship at Canada's National Research Council, he joined Ayerst Research Laboratories in Montreal in 1959, where he worked in the microbiology department — the lab that would receive the Easter Island soil. Sehgal helped isolate and characterize rapamycin and was a co-author on the foundational 1975 papers.
Sehgal became convinced that rapamycin was special — that it had important properties beyond killing fungi. He pushed it forward despite obstacles, including sending samples to the U.S. National Cancer Institute for screening when he suspected it could inhibit the growth of tumor cells. Then came the moment that has made his name famous in pharmacology. In 1983, Ayerst closed its Montreal laboratory, the rapamycin program was cancelled, and the bacterial cultures were slated for destruction.
Rather than let the organism be thrown away, Sehgal took vials of the rapamycin-producing bacteria home and stored them in his household freezer. The accounts agree on the essentials: he preserved the strain himself, and when the opportunity came he transported the precious samples — reportedly packed in a homemade dry-ice cooler — so the work could be revived. After Ayerst merged with Wyeth (the corporate lineage runs through American Home Products), new management restored support for rapamycin development in 1988. That revived program led, eleven years later, to the drug's approval. Sehgal lived to see rapamycin become a marketed medicine; he died of cancer on January 21, 2003, in Seattle. It is no exaggeration to say that without one scientist's refusal to discard a freezer vial, the entire field of mTOR biology and rapamycin medicine might have been delayed by years or lost altogether.
From Antifungal to Immune Suppressant
The pivot that changed rapamycin's destiny was the recognition that it powerfully suppresses the immune system. Researchers found that rapamycin blocked the activation and proliferation of T-lymphocytes — the immune cells responsible for attacking foreign tissue, including a transplanted organ. This was the same general problem that the blockbuster drug cyclosporine addressed, but rapamycin worked by a different mechanism, which made it attractive both on its own and in combination.
A landmark step in establishing rapamycin as a transplant drug was the work of the British transplant surgeon Sir Roy Calne and colleagues, who reported in 1989 in The Lancet that rapamycin could be used for immunosuppression in organ allografting, describing it as a highly active agent. Around the same period, transplant researchers including Randall E. Morris characterized how rapamycin prevented graft rejection in animal models. This body of work reframed rapamycin entirely: the molecule named for an antifungal property was now a candidate to keep transplanted kidneys, hearts, and livers alive.
This is also why rapamycin carries two names. As a marketed pharmaceutical its official generic (nonproprietary) name is sirolimus; "rapamycin" remains the original chemical name and the one most people use in the longevity context. They are the same compound.
Discovering the Target: TOR and mTOR
A drug can work for years before anyone understands how, and rapamycin is a classic example. The molecular detective story unfolded mostly in the 1990s. Working in yeast, Joseph Heitman, Rao Movva, and Michael N. Hall — then at the Biozentrum in Basel, Switzerland — published a pivotal paper in Science in 1991 identifying genes whose mutation made yeast resistant to rapamycin. They named these genes TOR1 and TOR2, for Target Of Rapamycin. The work also confirmed that rapamycin first binds a small protein called FKBP12, and that the resulting rapamycin–FKBP12 complex is what acts on the TOR proteins.
A few years later, several independent groups identified the mammalian equivalent of TOR. In 1994, David M. Sabatini (then a graduate student in Solomon Snyder's lab at Johns Hopkins) reported a mammalian protein he called RAFT1 in the journal Cell; other groups working at the same time named the same protein FRAP (from the Schreiber laboratory) and mTOR. The community eventually settled on the name mTOR — the mechanistic (originally "mammalian") target of rapamycin.
This mattered far beyond rapamycin itself. mTOR turned out to be a master regulator: a kinase that senses nutrients and growth signals and decides whether a cell should grow and build or conserve and recycle. Rapamycin became the essential tool that let biologists probe this central pathway — which is how a transplant antibiotic ended up at the heart of research on cancer, metabolism, and aging. The detailed biology is covered on the companion mTOR Inhibition Mechanism page.
Rapamune: Approval and the Rapalogs (1999 onward)
The revived development program reached its goal at the end of the decade. In September 1999, the U.S. Food and Drug Administration approved sirolimus, under the brand name Rapamune (Wyeth-Ayerst), as an oral solution for the prevention of organ rejection in kidney-transplant patients; an oral tablet form followed in 2000. After roughly three and a half decades, the molecule from the Easter Island soil was finally a licensed drug.
Rapamycin's success also spawned a family of chemical relatives, collectively called rapalogs — analogues engineered for better solubility or pharmacology while keeping the mTOR-inhibiting action. Everolimus and temsirolimus became important drugs in oncology, used against certain advanced kidney cancers and other tumors, and everolimus is also used in transplantation. The same biology underlies drug-eluting coronary stents: a sirolimus coating released slowly at the site of an artery repair helps prevent the vessel from re-narrowing (restenosis). All of these applications trace back to the single property that the rapamycin–FKBP12 complex inhibits mTOR.
The Longevity Turn (2009 to Today)
The newest and most talked-about chapter began when researchers asked whether inhibiting mTOR — a nutrient-sensing growth pathway — might slow aging itself, as caloric restriction does in many animals. The breakthrough finding came in 2009, when the U.S. National Institute on Aging's Interventions Testing Program (ITP) — a rigorous study run across three independent laboratories — reported in Nature that rapamycin extended both median and maximum lifespan in genetically diverse mice. Remarkably, the benefit appeared even though treatment was started late in the animals' lives (at roughly 600 days, the mouse equivalent of late middle age). This was the first time a drug had been shown to extend mammalian lifespan in such a careful test, and it electrified the aging-research field.
On the human side, the clearest controlled evidence so far concerns the immune system. In 2014, a team led by Joan Mannick reported in Science Translational Medicine that the rapalog everolimus (RAD001) improved the response to influenza vaccination in elderly volunteers by roughly 20 percent — a striking hint that low, intermittent mTOR inhibition might counter some effects of immune aging. More recently, the PEARL trial (Participatory Evaluation of Aging with Rapamycin for Longevity), a placebo-controlled study of low-dose weekly rapamycin in healthy adults run by AgelessRx, published one-year results in the journal Aging in 2024 reporting that intermittent low-dose rapamycin was generally well tolerated, with some improvements in body composition and other healthspan measures, particularly in women. Ongoing and proposed studies — and the Dog Aging Project, which is testing rapamycin in companion dogs — aim to learn whether these signals translate into meaningful, lasting benefit.
Evidence, Ethics, and Honest Reception
Because rapamycin is now promoted in some circles as an anti-aging breakthrough, an honest history has to draw a clear line between what is established and what is hopeful. The established facts are these: rapamycin is an FDA-approved drug, but only for preventing transplant rejection and a few specific conditions — not for healthy aging, longevity, or general "prevention." Its lifespan-extending effect is robustly demonstrated in mice and other laboratory animals. Whether it meaningfully extends healthy human lifespan is not yet proven; the human evidence consists of a small number of trials measuring biomarkers and short-term outcomes, not lifespan itself.
This means that taking rapamycin to slow aging is, by definition, an off-label, investigational use. It is a genuine prescription drug with genuine risks — mouth ulcers, raised blood lipids, impaired blood-sugar control, and dose-dependent suppression of immunity and wound healing among them — which is precisely why it should be prescribed and monitored by a qualified clinician rather than self-sourced. Anyone reading enthusiastic claims online should treat the longevity application as a serious experiment in progress, not a settled therapy. The honest summary is that rapamycin occupies the best-evidenced corner of pharmacological longevity research and remains unproven for that purpose — both halves of that sentence are true at once.
There is also the human and ethical dimension worth remembering. The drug exists because of one curious expedition, one resilient bacterium, and one scientist who refused to let his work be destroyed — and because of an island whose people were studied but never compensated. Knowing that fuller story is the point of reading the history at all. The current evidence, dosing approaches, mechanisms, and cautions are covered in depth in the companion Rapamycin Benefits articles and on the main Rapamycin page.
Research Papers and References
The list below combines key peer-reviewed sources on the discovery, mechanism, and longevity research of rapamycin (sirolimus) with curated PubMed topic-search links. Author names, titles, and journals are given as plain text; only the stable DOI, PMID, or archive link is hyperlinked, and each opens in a new tab.
- Vézina C, Kudelski A, Sehgal SN. Rapamycin (AY-22,989), a new antifungal antibiotic. I. Taxonomy of the producing streptomycete and isolation of the active principle. The Journal of Antibiotics. 1975;28(10):721-726. — PMID: 1102508
- Sehgal SN, Baker H, Vézina C. Rapamycin (AY-22,989), a new antifungal antibiotic. II. Fermentation, isolation and characterization. The Journal of Antibiotics. 1975;28(10):727-732. — PMID: 1102509
- Calne RY, Collier DStJ, Lim S, et al. Rapamycin for immunosuppression in organ allografting. The Lancet. 1989;2(8656):227. — PMID: 2568561
- Heitman J, Movva NR, Hall MN. Targets for cell cycle arrest by the immunosuppressant rapamycin in yeast. Science. 1991;253(5022):905-909. — doi:10.1126/science.1715094
- Sabatini DM, Erdjument-Bromage H, Lui M, Tempst P, Snyder SH. RAFT1: a mammalian protein that binds to FKBP12 in a rapamycin-dependent fashion and is homologous to yeast TORs. Cell. 1994;78(1):35-43. — doi:10.1016/0092-8674(94)90570-3
- Harrison DE, Strong R, Sharp ZD, et al. Rapamycin fed late in life extends lifespan in genetically heterogeneous mice. Nature. 2009;460(7253):392-395. — doi:10.1038/nature08221
- Mannick JB, Del Giudice G, Lattanzi M, et al. mTOR inhibition improves immune function in the elderly. Science Translational Medicine. 2014;6(268):268ra179. — doi:10.1126/scitranslmed.3009892
- Halford B. Rapamycin's secrets unearthed. Chemical & Engineering News. 2016;94(29):26-30 (feature on the discovery of rapamycin and the role of Suren Sehgal). — cen.acs.org — Rapamycin's Secrets Unearthed
- Rapamycin (sirolimus) discovery and history — PubMed: rapamycin discovery and history
- Rapamycin, mTOR, and lifespan extension — PubMed: rapamycin, mTOR, and lifespan
External Authoritative Resources
- LiverTox — Sirolimus (NCBI Bookshelf)
- The Dog Aging Project — rapamycin in companion dogs
- PubMed — All research on sirolimus (rapamycin)
Connections
- All Remedies
- Rapamycin
- Rapamycin Benefits
- Longevity Protocols
- Fasting
- Berberine
- GLP-1 Receptor Agonists
- NAD+ & NMN
- Fisetin