Pepsin
Pepsin is the stomach's main protein-digesting enzyme, and it has a quirk that makes it both useful and misunderstood: it only works in a strongly acidic environment. A hundred years ago, doctors prescribed pepsin as a digestive aid, and that history was largely accurate about one thing — pepsin is genuinely useless unless the stomach is acidic enough. Today pepsin still turns up in over-the-counter digestive supplements, usually paired with an acid like betaine hydrochloride, and it has become a research focus for an unexpected reason: when stomach contents reflux up into the throat, the pepsin that rides along can damage delicate tissue. This page walks through what pepsin actually is, why its dependence on acid matters, where the old uses hold up and where they don't, the honest story on reflux, and the safety cautions that the cheerful supplement marketing tends to skip.
Table of Contents
- Historical Medical Use (1926 U.S. Dispensatory)
- What Pepsin Actually Is
- How Pepsin Digests Protein
- Why Acidity Matters: The pH Switch
- Pepsin & Reflux: The LPR Story (Honest)
- Pepsin as a Digestive Aid Today
- What the Evidence Does and Doesn't Show
- Safety, Cautions & Myths
- Key Research Papers
- Connections
- Featured Videos
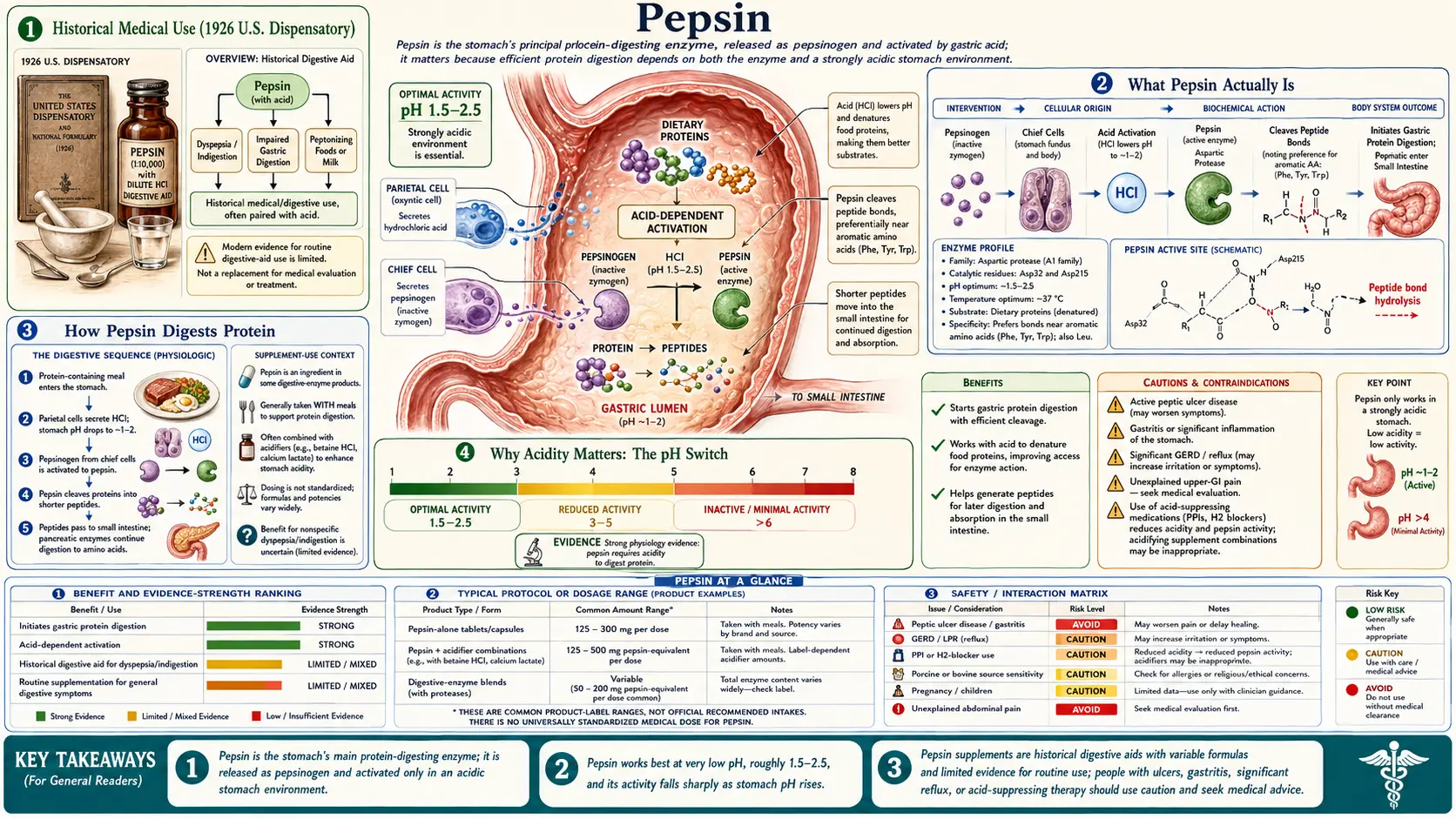
Historical Medical Use (1926 U.S. Dispensatory)
When the United States Dispensatory, 21st edition (1926) was the authoritative drug reference in America, pepsin had an established place in the doctor's bag as a remedy for "weak digestion." Physicians of that era prescribed it for the broad category of complaints we'd now call indigestion or dyspepsia — a heavy, bloated, slow-to-empty feeling after meals, especially after protein-rich food. The thinking was straightforward and, for its time, mechanistically reasonable: if a person seemed to be digesting protein poorly, give them more of the enzyme that digests protein.
What's striking is how accurate one part of the 1926 understanding was. Physicians of the era already knew that pepsin only worked when the stomach was strongly acidic, and that giving pepsin to someone with too little stomach acid was pointless unless you also supplied the acid. That is genuinely correct enzymology — pepsin is inert in a neutral or alkaline stomach. This is why pepsin was so often dispensed together with dilute hydrochloric acid or with acid-supplying salts. The pairing of an enzyme with an acid "activator," which you still see in modern supplements that combine pepsin with betaine hydrochloride, is essentially a century-old idea.
It is worth being honest about the limits, though. In 1926, doctors could not reliably measure stomach acid in the office, had no way to identify why a given patient felt dyspeptic, and reached for pepsin partly because the alternatives were few. Much of what was treated as "poor protein digestion" was almost certainly something else — slow stomach emptying, an ulcer, reflux, gallbladder trouble, anxiety, or simply eating too much too fast. The remedy was applied far more broadly than the actual problem (true protein maldigestion from low stomach acid) ever warranted. We can report what physicians did and believed; we should not carry the over-broad prescribing into the present.
What Pepsin Actually Is
Pepsin is an enzyme — a protein that speeds up a specific chemical reaction. Its job is to break down other proteins. It belongs to a family called the aspartic proteases, named for the two aspartic-acid building blocks at the heart of the enzyme that do the cutting. Historically, the pepsin used in medicine was extracted from the stomach lining of pigs (porcine) or, less often, cattle, and food-grade and supplement pepsin still comes from these animal sources.
The most important thing to understand about pepsin is that your stomach does not actually make pepsin. It makes a harmless, inactive precursor called pepsinogen. Think of pepsinogen as a pair of scissors with a plastic safety guard clipped over the blades. The cells that line the stomach (called chief cells) manufacture and store pepsinogen safely, because an enzyme that chews up protein would damage the very cells that made it if it were active inside them.
The "safety guard" comes off only when pepsinogen meets acid. When stomach acid (hydrochloric acid, made by separate cells called parietal cells) drops the surrounding pH low enough, the pepsinogen molecule snaps off a piece of itself and becomes active pepsin. Once a little active pepsin exists, it accelerates the conversion of more pepsinogen — a self-amplifying cascade. So acid is not just the environment pepsin prefers; acid is the trigger that creates active pepsin in the first place. This zymogen-to-enzyme activation (pepsinogen → pepsin) is one of the cleanest examples in the body of a built-in safety mechanism: the destructive tool only switches on where and when it's supposed to.
How Pepsin Digests Protein
Proteins in food — the muscle in a steak, the casein in cheese, the proteins in eggs and beans — are long chains of amino acids folded into tight, complex shapes. Your body can't absorb a whole protein; it has to be taken apart. That dismantling happens in stages, and pepsin runs the first stage, in the stomach.
Pepsin works like a pair of molecular scissors that cuts protein chains at particular spots, preferring to snip next to certain amino acids (it favors cutting beside aromatic and other large amino acids such as phenylalanine, tyrosine, and tryptophan). It doesn't reduce protein all the way down to single amino acids. Instead it chops big proteins into shorter fragments called peptides — and it physically opens up the tangled protein structure so the next enzymes can get at it. In that sense pepsin is the demolition crew that breaks the building into rubble; the fine sorting comes later.
The job is finished further downstream. When the partly digested, acidic stomach contents pass into the small intestine, the pancreas releases its own protein-cutting enzymes (such as trypsin and chymotrypsin), and the intestinal lining adds still more. These work in a neutral-to-slightly-alkaline environment and complete the breakdown into the small peptides and free amino acids your body can finally absorb. Pepsin is the opening act, not the whole show — which is one reason the body has considerable backup. People can digest protein adequately even with reduced pepsin activity, because the pancreas and intestine carry a large share of the load.
Why Acidity Matters: The pH Switch
Here is the single fact that explains almost everything practical about pepsin: pepsin is active only at low pH, roughly 1.5 to 3.5, and it is most active around pH 2 — the normal acidity of a working stomach. Move the pH up toward neutral and pepsin's activity falls off sharply. Take it into clearly alkaline territory and pepsin is not just slowed; it is denatured — its delicate three-dimensional shape unfolds and it is permanently inactivated, the way an egg white turns solid and can never go back to liquid.
This pH dependence is why every claim about pepsin has to be checked against the acidity question first:
- If the stomach is normally acidic, you already have plenty of active pepsin. Adding more is unlikely to do much, because acid (and the available pepsinogen), not enzyme quantity, is usually the limiting factor.
- If someone genuinely has low stomach acid (a real but over-diagnosed condition called hypochlorhydria, more common with age, certain autoimmune stomach conditions, and chronic acid-suppressing drugs), then swallowing pepsin alone won't help — there isn't enough acid to keep it active. This is exactly why pepsin supplements are paired with an acid such as betaine hydrochloride, and exactly what the 1926 physicians understood.
- If someone takes a proton-pump inhibitor (a powerful acid-blocking drug like omeprazole), they deliberately have a high stomach pH. In that environment, both their own pepsin and any pepsin they swallow are largely shut off. A controlled study in healthy volunteers showed that betaine HCl can transiently re-acidify the stomach even after a strong acid blocker — direct evidence that the acid, not the enzyme, is the lever (Yago and colleagues, 2013).
So the old belief that pepsin "works only when the stomach is strongly acidic" wasn't folklore — it's textbook biochemistry, and it should anchor how anyone thinks about taking pepsin.
Pepsin & Reflux: The LPR Story (Honest)
This is the part of the pepsin story that has flipped from "helpful remedy" to "part of the problem," and it deserves a careful, honest telling.
Normally pepsin stays in the stomach, where it belongs and where the acid keeps it working on your food. But in reflux, stomach contents wash back up the esophagus. When that backflow reaches all the way up to the throat and voice box, it's called laryngopharyngeal reflux (LPR), sometimes nicknamed "silent reflux" because it can cause throat symptoms — hoarseness, chronic throat-clearing, a lump-in-the-throat sensation, cough, post-nasal-drip feeling — without the classic heartburn. Refluxed material carries pepsin with it, and that is where the trouble starts.
The lining of the throat and larynx is far more fragile than the lining of the stomach, and it has none of the stomach's defenses. Research suggests pepsin can damage this tissue in two ways. First, although pepsin needs acid to digest protein actively, it is not necessarily destroyed the moment it reaches the less-acidic throat — it can remain present and become re-activated if the local environment turns acidic again (for example, during another reflux event or even from acidic food and drink). Second, and more strikingly, laboratory work has shown that throat lining cells can actually take pepsin up inside themselves through a process called receptor-mediated endocytosis, where it appears to cause cellular stress and inflammation even at a pH where it isn't busy digesting protein (Johnston and colleagues, 2007). In other words, the pepsin that floats up during reflux may injure the throat by getting into cells, not only by digesting tissue in the open.
This insight reshaped how specialists think about reflux. It helps explain a long-standing puzzle: why some people with throat symptoms don't get better on acid-blocking drugs alone. If acid-suppressing medication raises the pH but pepsin is still being refluxed and taken up by cells, the drug treats only half the problem. It is also why detecting pepsin in saliva or throat secretions has been explored as a way to diagnose reflux-related throat disease — pepsin doesn't belong up there, so finding it is a clue (Knight and colleagues, 2005; Wang and colleagues, 2019). Researchers are even investigating drugs and compounds that block pepsin's harmful activity in the throat as a future treatment avenue (Bardhan and colleagues, 2012).
The honest bottom line: pepsin in the throat is a problem to be limited, not a remedy. Anyone with persistent throat symptoms, a chronic cough, or hoarseness should be evaluated by a clinician (often an ENT specialist or gastroenterologist) rather than reaching for a pepsin supplement — and certainly should not take supplemental pepsin in the hope it will somehow help a refluxing throat.
Pepsin as a Digestive Aid Today
Pepsin is still sold today, almost always as one ingredient in a combination digestive-aid supplement rather than on its own. The most common pairing is pepsin with betaine hydrochloride, and the logic is exactly the 1926 logic, just better understood: betaine HCl is meant to supply acid, the acid keeps pepsin active, and the active pepsin helps break down protein. Some products also add other digestive enzymes (like pancreatic enzymes or plant-derived proteases) aimed at different parts of digestion.
The intended audience is people with suspected low stomach acid — for whom, in theory, restoring an acidic, enzyme-active stomach could ease protein-heavy meals. That's a legitimate target on paper. The practical problems are who actually has that condition, how to know, and how much to take, none of which are simple:
- Forms. Pepsin appears in capsules and tablets, typically combined with betaine HCl. It is also still used in laboratories and food processing for its protein-cutting ability; here we're concerned only with the supplement use.
- Dosing is not standardized. Pepsin activity is measured in functional units rather than simple milligrams, and product labels vary widely. There is no well-established, evidence-based dose for "improving digestion" in the general public, and self-escalating betaine HCl by feel — a popular internet practice — is not a validated or safe way to titrate.
- It is not a substitute for diagnosis. Genuine low stomach acid, pancreatic enzyme insufficiency, and many other causes of poor digestion each have proper tests and treatments. A supplement bought on a hunch can paper over a condition that deserves real evaluation.
For the much rarer, well-defined problem of the pancreas not making enough digestive enzymes (pancreatic exocrine insufficiency), the established treatment is prescription pancreatic enzyme replacement, not OTC pepsin — a different enzyme for a different part of the gut. Pepsin's modern niche is narrow and honestly somewhat thinly supported (Ianiro and colleagues, 2016).
What the Evidence Does and Doesn't Show
It's important to separate what is solidly established about pepsin from what is merely marketed.
Solid: Pepsin's biochemistry is textbook-certain. It is an aspartic protease; it is made as pepsinogen and activated by acid; it works only at low pH and is denatured by alkalinity; it begins protein digestion in the stomach (Samloff, 1982). Its role in damaging tissue during reflux — particularly the throat in LPR — is supported by a growing body of laboratory and clinical research (Johnston 2007; Bardhan 2012; Li and colleagues, 2025), and in animal models pepsin is genuinely necessary for the worst acid-reflux esophageal injury, not just a bystander (Nagahama and colleagues, 2006).
Weak or missing: The evidence that swallowing supplemental pepsin (with or without betaine HCl) measurably improves digestion, symptoms, or health in ordinary people is limited. There is a sound rationale and some supportive physiology for the acid side of the pairing, but high-quality randomized controlled trials testing pepsin digestive-aid supplements for indigestion in the general population are scarce. That doesn't mean it's useless for everyone — it means the honest position is "plausible for a specific, properly diagnosed minority, but not a proven general remedy." Shorter and true: pepsin is real and important biology, but as an over-the-counter pill it is under-studied, and confident health claims about it outrun the data.
Safety, Cautions & Myths
Pepsin supplements are generally combined with an acid, so the safety profile mirrors that of acid supplements like betaine hydrochloride. The cautions below are the ones the upbeat marketing tends to leave out.
- Do not use if you have an active ulcer, gastritis, or known acid-related damage. Adding acid and a protein-digesting enzyme to an already-irritated or eroded stomach lining can worsen pain and injury. If you have, or suspect, a peptic ulcer, pepsin/betaine HCl products are the wrong tool.
- Do not combine with acid-suppressing medication, and don't use it to "counteract" reflux drugs. If you're taking a proton-pump inhibitor or H2 blocker (often for a good medical reason), deliberately re-acidifying the stomach with a supplement is working against your own treatment and may aggravate symptoms.
- Be cautious with NSAIDs and other stomach-irritating drugs. Pain relievers like ibuprofen, naproxen, and aspirin already stress the stomach lining; combining them with acidifying supplements raises the risk of irritation and bleeding.
- Heartburn and reflux are usually NOT from too little acid — get evaluated, don't self-prescribe. This is the most important myth to correct. A popular online claim holds that most reflux is caused by low stomach acid and should be treated with more acid (betaine HCl + pepsin). For the large majority of people, that is mistaken: typical reflux involves stomach contents — including acid and pepsin — escaping upward, and adding acid can make it worse and can injure the esophagus or throat. Given what we now know about pepsin damaging throat tissue in LPR, self-treating reflux with supplemental pepsin is exactly backward. Persistent heartburn, throat symptoms, difficulty swallowing, unintended weight loss, or vomiting need proper medical evaluation, not a guessed-at supplement.
- Don't self-titrate by feeling. The internet practice of swallowing escalating betaine HCl capsules until you feel a "warmth" and then backing off is not a validated test for low stomach acid and risks irritating the gut. Real assessment of stomach acid is done clinically.
- Source and special situations. Pepsin is animal-derived (usually porcine), which matters for people with religious dietary restrictions or pork allergy. As with most supplements, there is little safety data in pregnancy and breastfeeding, so avoid unless a clinician advises otherwise. Supplement quality and labeling vary; products are not vetted like prescription drugs.
- Myth — "pepsin detoxes or repairs the gut." Pepsin is a protein-digesting enzyme, full stop. It does not detoxify the body, heal the gut lining, or cure disease, and there's no evidence it does anything beyond its narrow digestive role (and its unwanted tissue-damaging role when refluxed).
Key Research Papers
- Samloff IM, Townes PL. (1982). Pepsinogens I and II: Purification from gastric mucosa and radioimmunoassay in serum. Gastroenterology, 82(1):26–33. — Foundational human work characterizing the pepsinogens (the inactive precursors that acid converts to pepsin) and how they appear in serum, underpinning the pepsinogen → pepsin activation story. (PMID: 7053333)
- Yago MR, Frymoyer AR, Smelick GS, et al. (2013). Gastric Reacidification with Betaine HCl in Healthy Volunteers with Rabeprazole-Induced Hypochlorhydria. Molecular Pharmaceutics, 10(11):4032–4037. — A controlled study showing betaine HCl can briefly restore a low (acidic) stomach pH even after a strong acid-blocking drug — direct evidence that acid, the activator of pepsin, is the key variable. (PMID: 24074021)
- Ianiro G, Pecere S, Giorgio V, Gasbarrini A, Cammarota G. (2016). Digestive Enzyme Supplementation in Gastrointestinal Diseases. Current Drug Metabolism, 17(2):187–193. — A review of where digestive-enzyme supplementation does and doesn't have evidence, useful context for the limited, niche role of OTC enzymes like pepsin. (PMID: 26806042)
- Johnston N, Wells CW, Blumin JH, Toohill RJ, Merati AL. (2007). Receptor-Mediated Uptake of Pepsin by Laryngeal Epithelial Cells. Annals of Otology, Rhinology & Laryngology, 116(12):934–938. — Laboratory evidence that throat (laryngeal) cells actively take pepsin inside themselves, a mechanism for how refluxed pepsin can damage throat tissue even at non-digesting pH. (PMID: 18217514)
- Bardhan KD, Strugala V, Dettmar PW. (2012). Reflux Revisited: Advancing the Role of Pepsin. International Journal of Otolaryngology, 2012:646901. — A review reframing pepsin (not just acid) as a central agent of reflux injury, and a target for diagnosis and future therapy. (PMID: 22242022)
- Nagahama K, Yamato M, Nishio H, Takeuchi K. (2006). Essential Role of Pepsin in Pathogenesis of Acid Reflux Esophagitis in Rats. Digestive Diseases and Sciences, 51(2):303–309. — In an animal model, pepsin was necessary for the severe esophageal damage of acid reflux — acid alone was far less injurious — showing pepsin is an active culprit, not a bystander. (PMID: 16534672)
- Knight J, Lively MO, Johnston N, Dettmar PW, Koufman JA. (2005). Sensitive Pepsin Immunoassay for Detection of Laryngopharyngeal Reflux. The Laryngoscope, 115(8):1473–1478. — Demonstrated that detecting pepsin (which doesn't belong in the throat) can serve as a marker for laryngopharyngeal reflux. (PMID: 16094128)
- Wang CP, Wang CC, Lien HC, et al. (2019). Saliva Pepsin Detection and Proton Pump Inhibitor Response in Suspected Laryngopharyngeal Reflux. The Laryngoscope, 129(3):709–714. — Clinical study using salivary pepsin in suspected throat reflux, part of the effort to use pepsin as a practical diagnostic clue. (PMID: 30151836)
- Li C, Cao X, Wang H. (2025). Pathogenesis of pepsin-induced gastroesophageal reflux disease with advanced diagnostic tools and therapeutic implications. Frontiers in Medicine, 12:1516335. — A recent review of how pepsin drives reflux-related tissue damage and what that means for diagnosis and treatment.
Live PubMed Searches
- Pepsin, protein digestion & pH activation
- Pepsin & laryngopharyngeal reflux (LPR)
- Betaine HCl, gastric acid & hypochlorhydria
- Digestive enzyme supplementation & dyspepsia
Connections
- Betaine HCL
- Gut Healing
- Gut-Brain Axis
- Anti-Inflammatory Diet
- Natural Constipation Relief
- Gastroenterology
- Beef (Dietary Protein)
- Amino Acids
- All Remedies