Fenbendazole: History and Origins
Fenbendazole has two very different histories, and honesty requires telling them apart. The first is the real, documented story of a veterinary deworming drug: a benzimidazole compound developed by the German pharmaceutical company Hoechst in the early 1970s, sold under the brand name Panacur, and used safely in animals for half a century. The second is a much newer and far more contested story — how a single cancer patient's account, the "Joe Tippens protocol," turned an animal dewormer into a worldwide internet phenomenon promoted as a cancer cure. This article traces both threads carefully. It names the chemists and companies behind the drug's actual invention, follows the benzimidazole family back to its origin in 1961, recounts the Tippens story and the 2019 South Korean surge as the social events they were, and states plainly what the scientific and regulatory record says today: fenbendazole is not an approved cancer treatment in humans, no completed human clinical trials support that use, and major cancer organizations advise against it. Where the record is firm we say so; where a claim is anecdote, hope, or still unproven, we name it as such.
Table of Contents
- What Fenbendazole Is
- The Benzimidazole Family: Origins in 1961
- Hoechst and the Birth of Panacur (1970s)
- How the Drug Works: The Tubulin Story
- From Dewormer to Cancer Candidate
- The Joe Tippens Story (2016–2019)
- The South Korean Surge (2019)
- Evidence and Reception: An Honest Accounting
- Research Papers and References
- Connections
- Featured Videos
What Fenbendazole Is
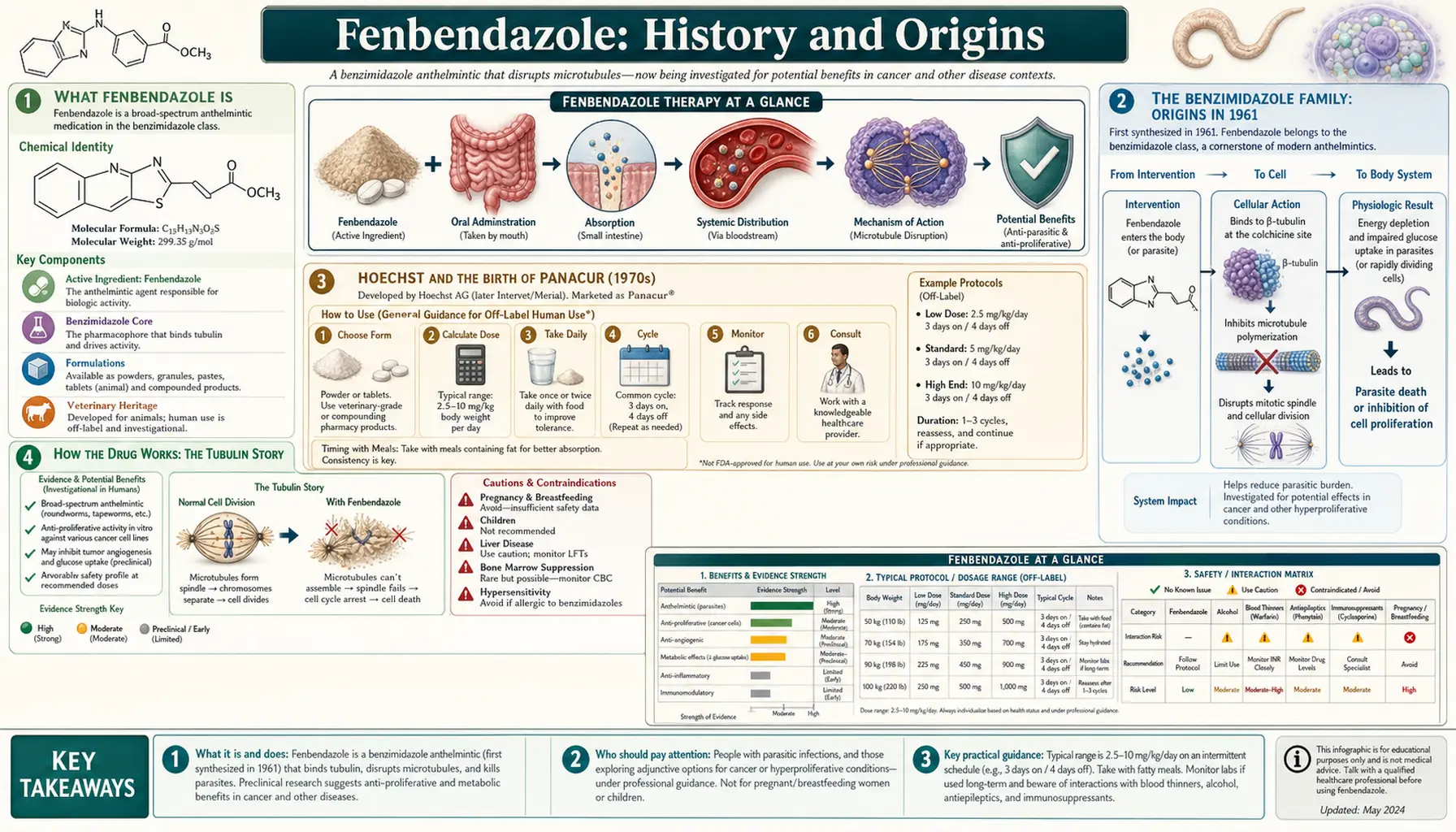
Before the history makes sense, it helps to be clear about what fenbendazole actually is. It is a broad-spectrum anthelmintic — a drug that kills parasitic worms — belonging to the chemical class called the benzimidazoles. Its full chemical name is methyl N-(6-phenylsulfanyl-1H-benzimidazol-2-yl)carbamate, and chemists classify it as a benzimidazole carbamate. In plain terms, it is a small molecule built around a benzimidazole ring, designed to be poorly absorbed into the bloodstream so that it stays in the gut where intestinal worms live.
Fenbendazole was created for animals, not people. It is given to cattle, sheep, goats, horses, pigs, poultry, dogs, cats, rabbits, fish, and reptiles to clear roundworms, hookworms, whipworms, and certain tapeworms. Its best-known brand names are Panacur and Safe-Guard. It has never been approved for human use by the U.S. Food and Drug Administration or the European Medicines Agency — a fact that sits at the centre of the modern controversy and that the later sections return to. Everything that follows — the inventors, the dates, the brand — describes a veterinary medicine with a long and unremarkable safety record in the animals it was made for.
The Benzimidazole Family: Origins in 1961
Fenbendazole did not appear out of nowhere; it is one member of a large drug family whose origin can be dated precisely. The story of the benzimidazole anthelmintics begins in 1961 at the laboratories of Merck Sharp & Dohme, where a team led by the chemist H. D. Brown, together with A. R. Matzuk and colleagues, synthesised a compound called thiabendazole (2-(4'-thiazolyl)benzimidazole). Their paper, "Antiparasitic Drugs. IV. 2-(4'-Thiazolyl)-Benzimidazole, A New Anthelmintic," appeared in the Journal of the American Chemical Society that year. Thiabendazole was the first of its kind, and it was licensed for human use the following year, in 1962.
Thiabendazole's arrival is genuinely regarded as a turning point in parasitology — the breakthrough that opened the way to an entire generation of broad-spectrum dewormers. Over the following two decades chemists at several companies modified the benzimidazole core to make compounds that were more potent, broader in spectrum, and effective against worms living outside the gut. This effort produced a now-familiar roster of drugs: cambendazole, parbendazole, mebendazole, flubendazole, oxfendazole, albendazole, and — the subject of this page — fenbendazole. They are chemical cousins, and they share the same basic way of working, described in the mechanism section below.
This lineage matters for understanding fenbendazole's modern reputation. Some of its benzimidazole relatives — particularly mebendazole, which is approved for humans — have been studied formally as possible repurposed cancer drugs. When people argue that fenbendazole "might" work against cancer, much of the underlying laboratory rationale actually comes from work on the broader benzimidazole class, not from fenbendazole alone. The family resemblance is real; the leap from "a relative was studied" to "this drug cures cancer" is not.
Hoechst and the Birth of Panacur (1970s)
Fenbendazole itself was developed in Germany by Hoechst AG (its animal-health arm trading as Farbwerke Hoechst), one of the great European chemical and pharmaceutical houses of the twentieth century. The compound was described by Hoechst in 1973 and introduced commercially around 1974, with the veterinary brand Panacur reaching the market in the 1970s; regulatory records list a first approval in 1977. Unlike a traditional herbal remedy, fenbendazole therefore has a clear corporate origin and a datable invention — it was the product of industrial medicinal chemistry, not folk tradition.
It is worth being candid about what is and is not documented here. The drug's institutional origin is well established — Hoechst, the early 1970s, the Panacur brand — but unlike, say, the discovery of penicillin or rapamycin, fenbendazole is not associated in the public record with a single famous "inventor" whose biography survives in popular accounts. It emerged from a corporate research programme refining the benzimidazole scaffold first opened up by thiabendazole. Over the decades the rights and manufacturing passed through corporate hands — Hoechst-Roussel Agri-Vet and later, after a series of mergers, into the portfolios of major animal-health companies — but the molecule and the Panacur name endured. By the time the cancer story began, fenbendazole had been an ordinary, inexpensive, off-patent veterinary dewormer for roughly forty years.
How the Drug Works: The Tubulin Story
To follow the rest of the history, it helps to understand what fenbendazole does inside a cell — because the same mechanism that kills worms is the one researchers later wondered about for cancer. Fenbendazole, like the other benzimidazoles, binds to a protein called β-tubulin. Tubulin is the building block of microtubules, the tiny scaffolding fibres that cells use to hold their shape, move materials around, and pull chromosomes apart when they divide. By binding tubulin, fenbendazole blocks microtubules from assembling. The mechanism by which benzimidazoles bind nematode β-tubulin and inhibit microtubule formation was characterised in classic veterinary-pharmacology work in the 1980s.
In a parasitic worm, jamming the microtubules wrecks the cells lining its gut and starves it — which is why the drug deworms so effectively. The reason it is relatively safe for the host animal is partly that fenbendazole binds worm tubulin much more tightly than mammalian tubulin, and partly that very little of the drug is absorbed from the gut into the body. That same logic — a molecule that disrupts cell division by hitting tubulin — is exactly what later drew the attention of cancer researchers, because some of the most important chemotherapy drugs, such as the taxanes and vinca alkaloids, also work by disrupting microtubules. That parallel is the hinge on which the next section turns. It is a real and interesting parallel; it is not, by itself, evidence that fenbendazole treats cancer in people.
From Dewormer to Cancer Candidate
The idea that an animal dewormer might fight cancer has a real scientific seed, even if it later grew into claims far beyond the evidence. Two strands feed into it. The first is the laboratory-animal observation often retold in the fenbendazole community: that mice in research colonies being treated for pinworm with fenbendazole proved unexpectedly resistant to growing implanted tumours, complicating some cancer experiments. This kind of incidental finding is the sort of thing that prompts a scientist to ask, "why?" — though it is an observation, not a treatment trial.
The second, firmer strand is genuine preclinical research. The most frequently cited fenbendazole-specific study was published in 2018 by Nilambra Dogra, Ashok Kumar, and Tapas Mukhopadhyay in the journal Scientific Reports. Working with human cancer cells and mouse models, they reported that fenbendazole acted as a moderate microtubule-destabilising agent and could kill cancer cells by hitting several pathways at once — disrupting microtubules, stabilising the tumour-suppressor protein p53, and interfering with cancer cells' glucose metabolism. Related laboratory work, much of it on the cousin drug mebendazole, has explored similar anticancer activity, and the broader effort to find new uses for old, cheap drugs is a legitimate field known as drug repurposing.
Here the crucial distinction must be drawn clearly. All of this is preclinical — it took place in cell cultures and in animals, not in controlled human trials. A compound killing cancer cells in a dish, or shrinking tumours in mice, is a reason to investigate further; it is emphatically not proof that the drug is safe or effective for treating cancer in a human being. Many compounds that look powerful in the laboratory fail in people. The science described here explains why fenbendazole became a plausible candidate worth studying — it does not establish that it works, and the social story that follows ran far ahead of what the laboratory had shown.
The Joe Tippens Story (2016–2019)
The modern fenbendazole phenomenon has a clear human origin point: a man named Joe Tippens. Tippens was an Oklahoma businessman who, in 2016, was diagnosed with small cell lung cancer that had spread widely through his body. The prognosis was grim — he has said he was given only a few months to live — and he enrolled in an immunotherapy clinical trial. According to his own account, a veterinarian suggested he try fenbendazole after hearing of the laboratory observation that it interfered with tumour growth in mice. Tippens began taking it alongside his trial immunotherapy, together with supplements including vitamin E, curcumin, and CBD oil — the combination that became known as the "Joe Tippens protocol."
Tippens subsequently reported that his scans showed no detectable cancer, and he shared his experience publicly on a blog, "My Cancer Story Rocks," which went viral in 2019. His account spread across social media and reached an enormous audience, and a large community of cancer patients began experimenting with the protocol. To his credit, Tippens has been consistent on one important point: he has not claimed that fenbendazole alone cured him, noting that he was also receiving immunotherapy in a clinical trial at the same time.
That caveat is essential, and it is where careful thinking is required. Tippens's story is a single, self-reported anecdote, and it is genuinely impossible to know what role — if any — the fenbendazole played, because he was simultaneously receiving an experimental immunotherapy that can, on its own, produce dramatic responses in some patients. A compelling personal account is not the same as evidence; it cannot separate cause from coincidence, account for the other treatment, or stand in for a controlled trial. The honest reading is that Tippens's case is the origin of a movement, not proof of a cure. The history is real and worth telling plainly; the medical conclusion many drew from it outran what one person's experience can support.
The South Korean Surge (2019)
The reach of the Tippens story is itself part of the history. In 2019, after his account circulated widely on Korean-language social media, fenbendazole became a national talking point in South Korea. Cancer patients and their families began buying veterinary fenbendazole, and reports described animal-pharmacy stocks selling out as demand surged. The episode became one of the most-discussed health stories in the country that year, amplified by video platforms documenting patients' experiences.
The reaction from the medical establishment was cautionary. Korean health authorities and cancer specialists publicly warned that fenbendazole had not been proven safe or effective for treating cancer in people, that the evidence was limited to laboratory studies, and that patients risked harm — including the danger of abandoning or undermining proven treatments. The surge is a striking illustration of how quickly a single anecdote, moving through social media, can become a mass behaviour that races ahead of the science. It belongs in the history not as evidence that the drug works, but as a documented social event — a case study in how medical hope spreads online.
Evidence and Reception: An Honest Accounting
Because the rest of this article describes a popular movement, this section states the scientific and regulatory reality as plainly as possible. Fenbendazole is not an approved cancer treatment for humans. Neither the U.S. Food and Drug Administration nor the European Medicines Agency permits it for human use; it remains a veterinary medicine. As of this writing there are no completed randomised controlled human clinical trials showing that fenbendazole is safe or effective against any human cancer. The interesting laboratory and animal findings remain exactly that — preclinical.
Major cancer bodies have spoken directly to the question. The American Cancer Society states flatly that the FDA "has never approved fenbendazole for humans for any purpose," that "scientific data does not exist about whether fenbendazole is safe and effective for people," and that there is "no proven benefit but several potential risks" — adding that oncologists do not prescribe it. The American Society of Clinical Oncology (ASCO) has issued a clinical notice recommending against the use of fenbendazole (and ivermectin) for cancer outside of clinical trials, noting the absence of robust, peer-reviewed clinical evidence that it is safe or effective for any human malignancy.
The risks are not merely theoretical. The medical literature now includes documented cases of liver injury in people who self-administered fenbendazole for cancer. In one well-known report, an 80-year-old woman with non-small cell lung cancer, taking the immunotherapy pembrolizumab, developed severe drug-induced liver injury after a month of self-administering fenbendazole that she had learned about on social media; her liver function recovered once she stopped the drug, and her tumour had not responded. Additional case reports describe similar hepatic injury. Beyond direct toxicity, clinicians warn of two further dangers: the possibility that an unregulated drug taken in secret may interact with proper cancer therapy, and the risk that someone might delay or forgo proven treatment in favour of an unproven one.
None of this is to dismiss the underlying scientific question. There is legitimate preclinical interest in benzimidazoles as repurposed anticancer agents, and serious researchers have argued that properly funded human trials would be worthwhile — precisely because a cheap, widely available drug with anticancer activity in the laboratory would be valuable if it proved out. The barrier is partly economic: as an off-patent generic, fenbendazole attracts little of the funding needed for large human trials. The fair conclusion is the one this whole article has built toward: fenbendazole has a real, well-documented history as a veterinary dewormer and a genuine, unresolved place as a laboratory cancer candidate — but the leap to a proven human cancer cure has not been made, and anyone presenting it as one is reporting hope, not fact. Anyone considering it should do so only in conversation with their own oncologist. The detailed mechanisms, protocols, dosing, and safety discussion are covered in the companion Fenbendazole Benefits articles and on the main Fenbendazole page; this history is concerned with how the drug came to be, and how it came to be talked about.
Research Papers and References
The list below combines key peer-reviewed sources on fenbendazole's chemistry, its proposed anticancer activity, its documented risks, and the mainstream medical reception, with curated PubMed topic-search links. Author names, titles, and journals are given as plain text; only the stable DOI, PMID, or archive link is hyperlinked, and each opens in a new tab. Statements attributed above to the American Cancer Society and ASCO are drawn from the authoritative resources listed at the end.
- Brown HD, Matzuk AR, Ilves IR, et al. Antiparasitic drugs. IV. 2-(4'-thiazolyl)-benzimidazole, a new anthelmintic. Journal of the American Chemical Society. 1961;83(7):1764-1765. — doi:10.1021/ja01468a052
- Dogra N, Kumar A, Mukhopadhyay T. Fenbendazole acts as a moderate microtubule destabilizing agent and causes cancer cell death by modulating multiple cellular pathways. Scientific Reports. 2018;8:11926. — doi:10.1038/s41598-018-30158-6
- Nguyen J, Nguyen TQ, Han B, Hoang BX. Oral fenbendazole for cancer therapy in humans and animals. Anticancer Research. 2024;44(9):3725-3735. — doi:10.21873/anticanres.17197
- Yamaguchi T, Shimizu J, Oya Y, Horio Y, Hida T. Drug-induced liver injury in a patient with nonsmall cell lung cancer after the self-administration of fenbendazole based on social media information. Case Reports in Oncology. 2021;14(2):886-891. — PMID: 34248555
- Anthelmintic agents. In: LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. National Institute of Diabetes and Digestive and Kidney Diseases. — NCBI Bookshelf: NBK548602
- Fenbendazole cancer research — PubMed: fenbendazole and cancer
- Benzimidazole anthelmintics: history and mechanism — PubMed: benzimidazole anthelmintic history and tubulin
External Authoritative Resources
- American Cancer Society — What to Know About Fenbendazole
- ASCO — Clinical Notice: Recommending Against Ivermectin and Fenbendazole for Cancer Treatment
- PubMed — All research on fenbendazole