Procalcitonin Test (PCT): Bacterial Infection and Sepsis Marker
Procalcitonin (PCT) is a 116-amino acid prohormone of calcitonin that is normally undetectable in healthy individuals (<0.05 ng/mL). During serious bacterial infections, virtually every cell type in the body begins producing PCT in response to bacterial endotoxin and pro-inflammatory cytokines, causing levels to rise dramatically — sometimes over 100-fold. In contrast, interferon-gamma released during viral infections actively suppresses ectopic PCT production, explaining why PCT remains low in most viral illnesses. This bacterial-versus-viral discrimination makes PCT one of the most clinically useful biomarkers for antibiotic stewardship and sepsis management.
- Overview — What Is Procalcitonin?
- Biochemistry and Production
- Reference Ranges and Interpretation
- Distinguishing Bacterial from Viral Infection
- PCT in Sepsis Diagnosis and Severity
- Antibiotic Stewardship: PCT-Guided Protocols
- False Positives and Limitations
- Key Research and Citations
- Connections
- Featured Videos
Overview — What Is Procalcitonin?
Procalcitonin is a prohormone of calcitonin produced under normal physiological conditions exclusively by thyroid parafollicular C cells, where it is immediately processed into the mature hormone calcitonin. In healthy individuals, circulating PCT levels are virtually undetectable — typically below 0.05 ng/mL (equivalent to 0.05 µg/L). This tight baseline makes even small elevations clinically meaningful.
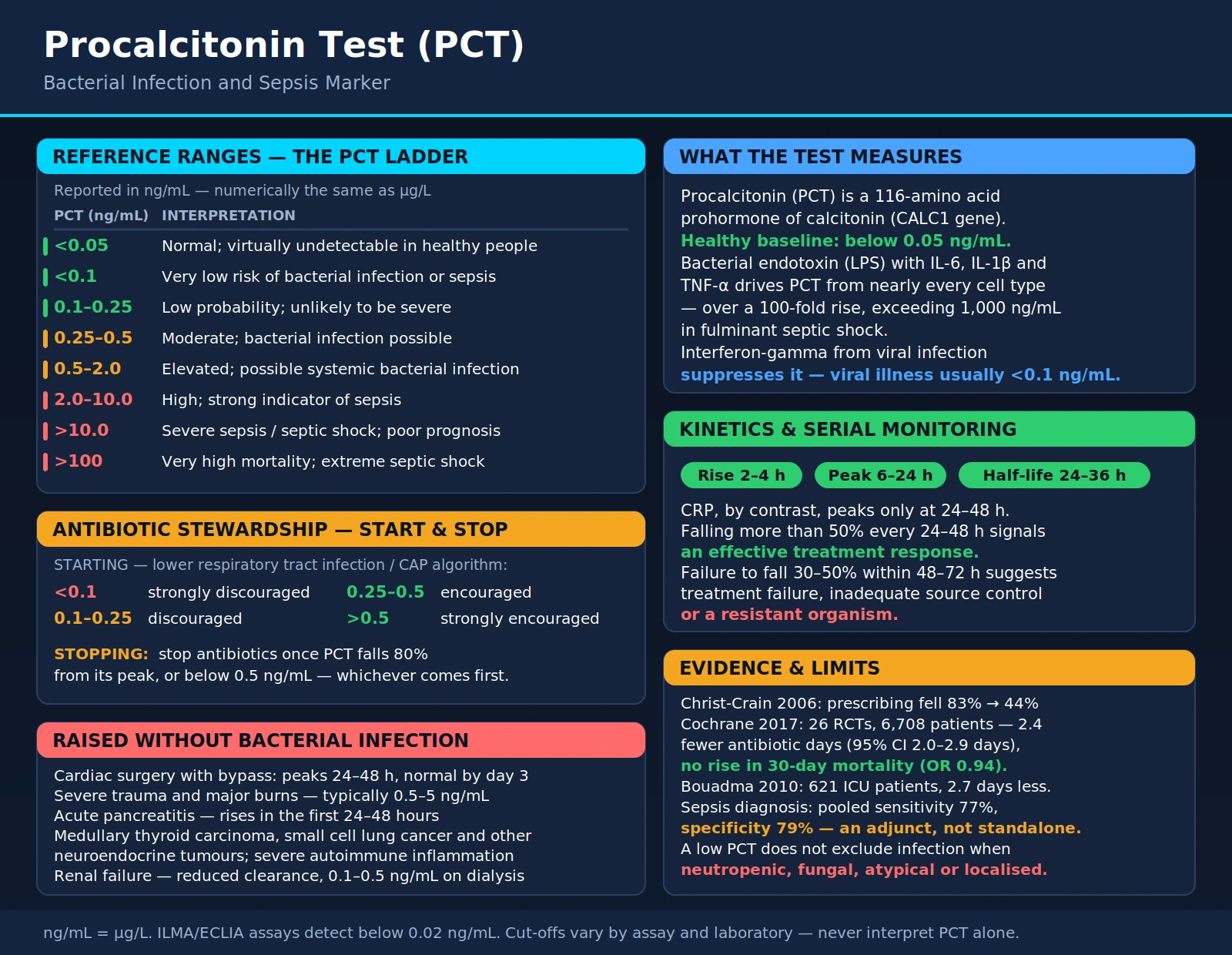
During severe bacterial infections, this picture changes dramatically. Bacterial endotoxin (lipopolysaccharide, LPS), as well as pro-inflammatory cytokines including IL-6, IL-1β, and TNF-α, trigger ectopic PCT production across virtually every cell type in the body: hepatocytes, monocytes, adipocytes, and parenchymal cells of the lungs, kidneys, and intestines. The result is a massive surge in circulating PCT that can exceed 1,000 ng/mL in fulminant septic shock.
Crucially, this ectopic production is suppressed by interferon-gamma (IFN-γ), a cytokine characteristically elevated in viral infections. This mechanism explains why PCT remains low in most viral syndromes — even severe ones — while rising sharply in bacterial disease. PCT was first identified as a sepsis biomarker by Assicot et al. in 1993 (PMID: 8098784), a landmark observation that has since been validated in thousands of clinical trials and is embedded in international sepsis guidelines.
Biochemistry and Production
PCT is a 116-amino acid protein encoded by the CALC1 gene. Its structure consists of three functional domains:
- N-terminal region (amino acids 1–57): Katacalcin precursor sequence, cleaved off during normal thyroid processing.
- Central region (amino acids 60–91): The 32-amino acid calcitonin sequence, which becomes the biologically active hormone under normal conditions.
- C-terminal region (amino acids 96–116): Calcitonin carboxypeptidase-1 region, also cleaved in the thyroid.
In thyroid C cells, all three domains are cleaved by specific processing enzymes to yield mature calcitonin, katacalcin, and the N-terminal fragment. These processing enzymes are absent in non-thyroid cells. When ectopic PCT production is triggered by bacterial infection, the intact 116-amino acid PCT molecule accumulates in the circulation because extra-thyroidal cells cannot process it — this intact form is what immunoassays detect.
Kinetics: PCT rises within 2–4 hours of bacterial infection onset, peaks between 6 and 24 hours, and has a circulating half-life of approximately 24–36 hours. This kinetic profile offers important clinical advantages over other inflammatory markers:
- Faster than CRP: C-reactive protein typically peaks at 24–48 hours post-infection onset; PCT peaks earlier and reflects bacterial load more acutely.
- More specific than IL-6: Interleukin-6 rises very rapidly but is also highly transient and non-specific, making it unsuitable for serial monitoring.
- Ideal for serial monitoring: The 24–36 hour half-life means that twice-daily or daily PCT measurements clearly reflect treatment response — a falling PCT signals effective antibiotic therapy, while a plateau or rise suggests treatment failure.
PCT is measured in plasma or serum using immunoluminometric assay (ILMA) or electrochemiluminescence immunoassay (ECLIA). Both platforms have excellent analytical sensitivity with lower detection limits below 0.02 ng/mL.
Reference Ranges and Interpretation
PCT results are reported in ng/mL (nanograms per milliliter), which is numerically equivalent to µg/L (micrograms per liter). The following stratified reference ranges reflect published consensus thresholds:
| PCT Level (ng/mL) | Interpretation |
|---|---|
| <0.05 | Normal; virtually undetectable in healthy individuals |
| <0.1 | Very low risk of bacterial infection or systemic sepsis |
| 0.1–0.25 | Low probability; bacterial infection possible but unlikely to be severe |
| 0.25–0.5 | Moderate elevation; bacterial infection possible — clinical correlation required |
| 0.5–2.0 | Elevated; suggests possible systemic bacterial infection (soft sepsis) |
| 2.0–10.0 | High; strong indicator of systemic bacterial infection or sepsis |
| >10.0 | Severe sepsis / septic shock; correlates with poor prognosis |
| >100 | Associated with very high mortality; extreme septic shock |
These thresholds are widely used in clinical practice but must always be interpreted in clinical context. A PCT of 0.4 ng/mL in a patient with classic pneumonia symptoms and a consolidation on chest X-ray has different weight than the same result in an asymptomatic individual with known chronic kidney disease. No biomarker replaces clinical judgment.
Distinguishing Bacterial from Viral Infection
The most impactful clinical application of PCT testing — particularly in the outpatient and emergency department setting — is differentiating bacterial from viral respiratory tract infections, where unnecessary antibiotic prescribing is endemic.
The landmark ProCAP trial (Christ-Crain et al., 2006, PMID: 17018932) randomized patients with community-acquired lower respiratory tract infections (LRTI) to PCT-guided versus standard antibiotic management. PCT guidance reduced antibiotic prescription rates from 83% to 44% without any increase in adverse outcomes, treatment failure, or mortality. This single trial established the proof of concept that PCT could safely halve antibiotic use in a high-prescribing setting.
The larger ProHOSP trial (Schuetz et al., 2009, PMID: 19738090), enrolling 1,359 patients across six Swiss hospitals, confirmed that PCT-guided therapy was non-inferior to guideline-adherent standard therapy across all primary outcomes — 30-day adverse outcomes, length of hospital stay, and antibiotic duration — while significantly reducing antibiotic exposure.
Algorithmic thresholds for lower respiratory tract infections and community-acquired pneumonia (CAP):
- PCT <0.1 ng/mL: Antibiotics strongly discouraged
- PCT 0.1–0.25 ng/mL: Antibiotics discouraged
- PCT 0.25–0.5 ng/mL: Antibiotics encouraged
- PCT >0.5 ng/mL: Antibiotics strongly encouraged
For viral syndromes — influenza, RSV, rhinovirus, adenovirus, and even mild-to-moderate COVID-19 disease — PCT typically remains below 0.1 ng/mL. Elevated PCT in a COVID-19 patient should raise suspicion for bacterial superinfection. A meta-analysis by Huang et al. (2018, PMID: 30020557) in the New England Journal of Medicine further confirmed PCT-guided therapy reduced antibiotic use by 2.7 days compared to standard care across diverse acute respiratory infection settings.
PCT in Sepsis Diagnosis and Severity
Sepsis — life-threatening organ dysfunction caused by a dysregulated host response to infection — is one of the leading causes of in-hospital mortality worldwide. Early, accurate diagnosis is critical because each hour of delay in effective antibiotic therapy increases mortality by approximately 7%. PCT plays an important supporting role in this diagnostic and prognostic context.
The Surviving Sepsis Campaign 2021 International Guidelines (Rhodes et al., 2017, PMID: 28101605) include PCT as a useful adjunct biomarker alongside lactate and clinical scoring systems. PCT >10 ng/mL correlates with bacteremia and septic shock severity. In a systematic review and meta-analysis by Wacker et al. (2013, PMID: 23375419), PCT had a pooled sensitivity of 77% and specificity of 79% for sepsis diagnosis — clinically useful but not standalone diagnostic.
Serial PCT for treatment monitoring: Failure of PCT to fall by 30–50% within 48–72 hours of antibiotic initiation is a strong signal of treatment failure, inadequate source control, or a resistant organism. Conversely, a rapidly declining PCT (falling >50% every 24–48 hours) indicates an effective treatment response. This serial monitoring capability is one of PCT's most valuable clinical attributes — it quantifies bacterial load dynamics in a way that clinical symptoms alone cannot.
PCT also correlates with the Sequential Organ Failure Assessment (SOFA) score and can be used to track multi-organ involvement. The PRORATA trial (Bouadma et al., 2010, PMID: 20097417), enrolling 621 ICU patients, demonstrated that PCT-guided antibiotic discontinuation reduced total antibiotic exposure by 2.7 days compared to standard care without increasing 28-day mortality or ICU length of stay.
Antibiotic Stewardship: PCT-Guided Protocols
The global antibiotic resistance crisis — driven in large part by unnecessary antibiotic prescribing — makes PCT one of the most important tools in modern antimicrobial stewardship programs. By providing an objective, quantitative, time-varying measure of bacterial infection burden, PCT enables clinicians to safely shorten antibiotic courses without compromising patient outcomes.
The de Jager et al. 2010 study (PMID: 20602568) validated an evidence-based PCT stop rule: antibiotics can be safely discontinued when PCT falls 80% from its peak value, OR when it reaches an absolute level below 0.5 ng/mL in non-severely ill patients. For ICU patients with sepsis, the stop threshold is typically <0.5 ng/mL or an 80% reduction from peak, whichever is reached first.
The Schuetz et al. 2017 Cochrane meta-analysis (PMID: 28526066) synthesized 26 randomized controlled trials comprising 6,708 patients and found that PCT-guided antibiotic protocols:
- Reduced total antibiotic duration by a mean of 2.4 days (95% CI: 2.0–2.9 days)
- Did not increase 30-day mortality (OR 0.94; 95% CI: 0.71–1.23)
- Did not increase treatment failure rates
- Reduced antibiotic-associated adverse effects (diarrhea, renal injury, fungal overgrowth)
The de Jong et al. 2016 LRTI trial (PMID: 27185348) in critically ill patients confirmed similar findings — PCT guidance reduced antibiotic duration by 4.2 days in the ICU population specifically, with no increase in 28-day mortality, 1-year mortality, or readmission rates. These consistent findings across diverse populations and care settings provide strong evidence that PCT-guided stewardship is both effective and safe.
Practical implementation in hospital antibiotic stewardship programs typically involves:
- Baseline PCT at admission for suspected infection
- Repeat PCT every 24–48 hours during antibiotic therapy
- Discontinuation trigger: PCT <0.5 ng/mL or ≥80% reduction from peak
- Documentation of PCT trajectory in clinical notes
False Positives and Limitations
PCT is a powerful but imperfect tool. Understanding its limitations is as important as understanding its strengths. The following conditions can elevate PCT in the absence of bacterial infection:
- Major cardiac surgery with cardiopulmonary bypass: PCT typically peaks at 24–48 hours post-operatively and normalizes by day 3. This post-surgical elevation reflects a systemic inflammatory response, not infection. Interpreting PCT in the immediate post-cardiac-surgery period requires caution and serial trending.
- Severe trauma and major burns: The non-infectious cytokine surge following major tissue injury can elevate PCT to moderate levels (typically 0.5–5 ng/mL), though values above 10 ng/mL in a trauma patient should still raise concern for concurrent infection.
- Acute pancreatitis: PCT rises in the first 24–48 hours, with higher levels correlating with severe necrotizing pancreatitis. PCT can help distinguish infected from sterile pancreatic necrosis later in the disease course (>72 hours).
- Medullary thyroid carcinoma (MTC): MTC cells produce calcitonin precursors including PCT. Very high PCT in the absence of infection should prompt consideration of MTC. Serial PCT is a standard marker for post-thyroidectomy MTC recurrence monitoring.
- Small cell lung cancer and other neuroendocrine tumors: Ectopic production of calcitonin/PCT precursors can cause elevated baseline PCT values.
- Renal failure: Reduced PCT clearance modestly elevates baseline PCT (typically 0.1–0.5 ng/mL range in dialysis patients). Serial trending and higher absolute thresholds are needed in this population.
- Autoimmune multi-organ dysfunction: Rare autoimmune conditions involving severe systemic inflammation can occasionally elevate PCT modestly.
False negatives — conditions where PCT may be inappropriately low despite bacterial infection:
- Immunocompromised patients: Neutropenic patients (from chemotherapy) may have blunted PCT responses because the cytokine cascade driving ectopic production is itself impaired. A normal PCT in a febrile neutropenic patient does not exclude serious infection.
- Localized infections without systemic spread: An early, well-contained abscess or cellulitis may not elevate PCT significantly before systemic spread occurs.
- Fungal infections: Fungal pathogens cause variable, generally lower PCT elevations compared to gram-negative bacteria. A normal PCT does not exclude invasive candidiasis or aspergillosis.
- Atypical bacterial organisms: Some intracellular bacteria (e.g., Mycoplasma pneumoniae, Chlamydophila pneumoniae) may generate lower PCT responses than typical extracellular pathogens.
PCT should never be used as a standalone diagnostic. It provides the highest clinical value when interpreted alongside the clinical history, physical examination, vital signs, white blood cell count, cultures, and imaging findings.
Key Research and Citations
- Assicot M, Gendrel D, Carsin H, Raymond J, Guilbaud J, Bohuon C. (1993). High serum procalcitonin concentrations in patients with sepsis and infection. Lancet. 341(8844):515–518. — Search PubMed
- Christ-Crain M, Jaccard-Stolz D, Bingisser R, et al. (2006). Procalcitonin guidance of antibiotic therapy in community-acquired pneumonia: a randomized trial. Am J Respir Crit Care Med. 174(1):84–93. — Search PubMed
- Schuetz P, Christ-Crain M, Thomann R, et al. (2009). Effect of procalcitonin-based guidelines vs standard guidelines on antibiotic use in lower respiratory tract infections: the ProHOSP randomized controlled trial. JAMA. 302(10):1059–1066. PMID: 19738090
- Schuetz P, Wirz Y, Sager R, et al. (2017). Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev. 10:CD007498. — Search PubMed
- de Jong E, van Oers JA, Beishuizen A, et al. (2016). Efficacy and safety of procalcitonin guidance in reducing the duration of antibiotic treatment in critically ill patients: a randomised, controlled, open-label trial. Lancet Infect Dis. 16(7):819–827. — Search PubMed
- Bouadma L, Luyt CE, Tubach F, et al. (2010). Use of procalcitonin to reduce patients' exposure to antibiotics in intensive care units (PRORATA trial): a multicentre randomised controlled trial. Lancet. 375(9713):463–474. PMID: 20097417
- Müller B, Harbarth S, Stolz D, et al. (2010). Diagnostic and prognostic accuracy of clinical and laboratory parameters in community-acquired pneumonia. BMC Infect Dis. 10:310. — Search PubMed
- De Jager CP, van Wijk PT, Mathoera RB, et al. (2010). Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Crit Care. 14(5):R192. — Search PubMed
- Wacker C, Prkno A, Brunkhorst FM, Schlattmann P. (2013). Procalcitonin as a diagnostic marker for sepsis: a systematic review and meta-analysis. Lancet Infect Dis. 13(5):426–435. PMID: 23375419
- Meisner M. (2014). Update on procalcitonin measurements. Ann Lab Med. 34(4):263–273. — Search PubMed
- Huang DT, Yealy DM, Filbin MR, et al. (2018). Procalcitonin-guided use of antibiotics for lower respiratory tract infection. N Engl J Med. 379(3):236–249. — Search PubMed
- Rhodes A, Evans LE, Alhazzani W, et al. (2017). Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 43(3):304–377. PMID: 28101605