Prostate Conditions: History and Discovery
The prostate is a small gland with a long history. It was first recognized in antiquity by anatomists working in Alexandria more than two thousand years ago, yet the three conditions that dominate its modern story — benign enlargement (BPH), inflammation (prostatitis), and prostate cancer — were only gradually disentangled across the centuries. This page traces that arc: from Herophilus and the Renaissance anatomists, through the first clear descriptions of prostatic obstruction and cancer in the 18th and 19th centuries, to Charles Huggins' Nobel-winning discovery that prostate cancer feeds on male hormones, and finally to the prostate-specific antigen (PSA) blood test and the genuine debate it sparked. Throughout, we have verified every name, date, and "first" against the medical-history literature and flagged anything uncertain — because accuracy matters more than a tidy story.
Table of Contents
- Herophilus and the Discovery in Antiquity
- What the Name "Prostate" Really Means
- Renaissance Anatomy: Massa and Vesalius
- Morgagni and the Recognition of Enlargement
- The First Descriptions of Prostate Cancer
- Huggins and the Hormone Connection
- PSA: The Discovery of a Blood Test
- The PSA-Screening Debate: Benefits and Harms
- Diagnosis Today: Exam, Ultrasound, and Biopsy
- Research Papers and References
- Connections
- Featured Videos
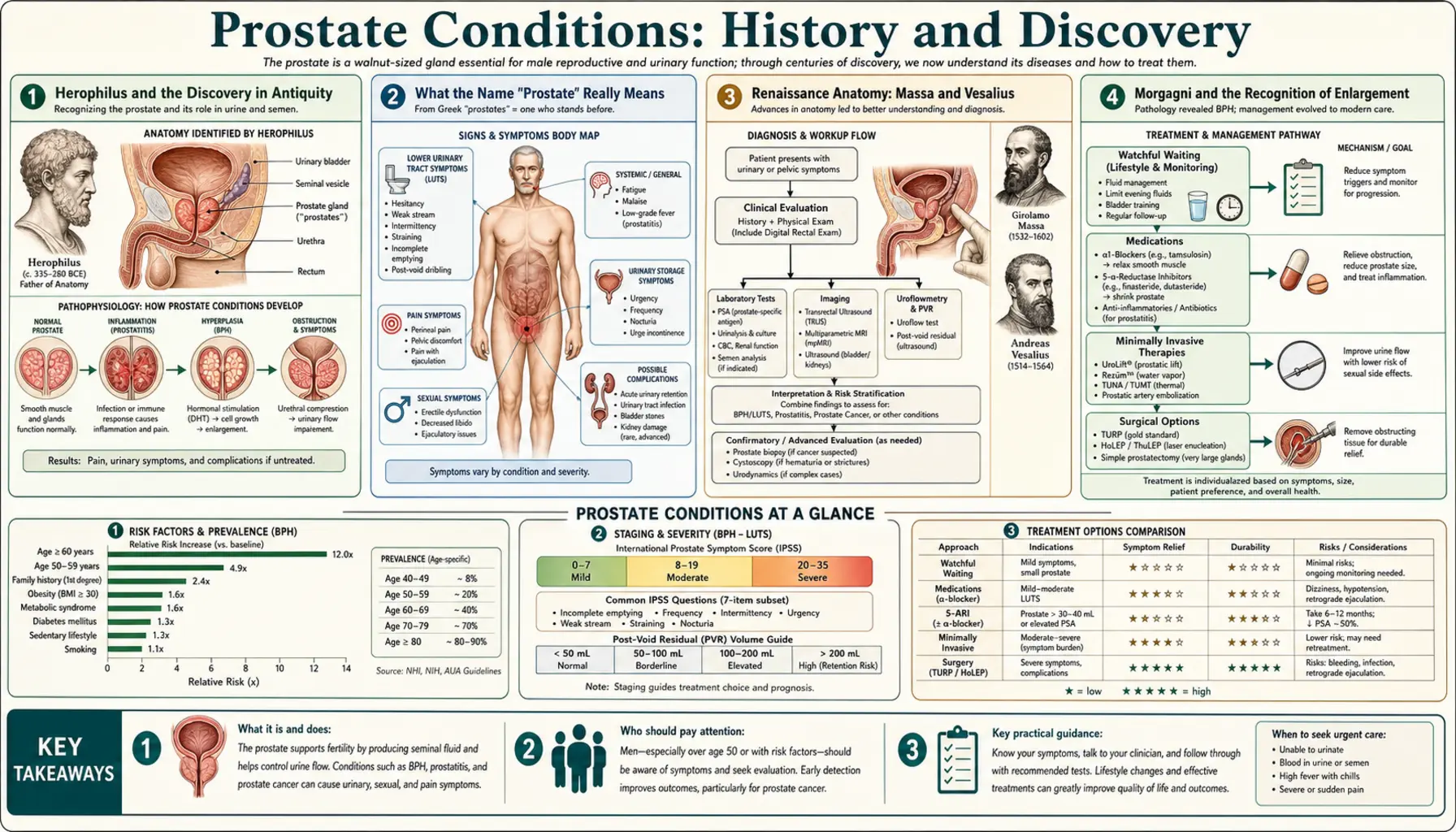
Herophilus and the Discovery in Antiquity
The prostate enters recorded history in the great medical school of Alexandria, in the third century BCE. Credit for the first description is traditionally given to Herophilus of Chalcedon (often called Herophilus of Alexandria, who lived roughly 325–255 BCE), one of the first physicians known to have performed systematic human dissection. We do not have this from Herophilus himself; his original writings are lost. Instead, the attribution reaches us through the great Roman physician Galen of Pergamon (129–c.216 CE), who centuries later credited Herophilus with describing the glandular structures sitting below the bladder and connected to the seminal vesicles. This is an honest example of how ancient medical history works — a foundational "first" preserved only as a later author's report.
It is worth being precise about what Herophilus actually saw, because the historical record is genuinely nuanced. He described paired glandular bodies near the neck of the bladder, but scholars note that his account may have blended what we now call the prostate with the seminal vesicles — the fine anatomical line between the two organs was not cleanly drawn for many centuries. So Herophilus deserves credit as the first to identify a glandular organ in this region, while we acknowledge that the modern, sharply-defined "prostate" is a later refinement built on his observation.
For the next millennium and a half, the prostate received little independent attention. Galen's anatomy — much of it derived from animal dissection — dominated European and Islamic medicine, and the organ remained a minor, somewhat blurred feature of the male pelvis. Its rediscovery as a distinct structure, and the modern name it carries, would have to wait for the anatomical revolution of the Renaissance.
What the Name "Prostate" Really Means
The English word prostate comes from the Ancient Greek prostates (προστατησ), usually translated "one who stands before," "protector," or "guardian" — an apt image for a gland that stands at the gateway of the bladder. The popular telling stops there, but the real etymological history, traced in detail by Marx and Karenberg, is more interesting and more honest.
In classical Greek, prostates was not a medical word at all: it meant something like "president," "leader," or "one who stands at the front," used in civic and political life. Herophilus himself reportedly called the glands by a different term — rendered roughly as adenoeides parastatai, the "glandular assistants" or "bystander glands," describing structures that stand beside rather than before. The modern anatomical name took hold much later: the medical literature credits the French physician André du Laurens (Laurentius) with introducing the Latin term prostatae for the organ around the year 1600. The familiar "one who stands before" gloss, in other words, is a Renaissance reinterpretation, not the literal meaning Herophilus had in mind.
This small correction shows why careful history is worth the effort. The poetic "guardian gland" story is not wrong as a description of where the prostate sits, but the scholarship shows the name evolved from "assistant" to "protector" over nearly two thousand years — even the words for our anatomy carry their own buried history.
Renaissance Anatomy: Massa and Vesalius
The prostate's rediscovery as a distinct organ belongs to the sixteenth-century revolution in human anatomy, when physicians returned to careful, hands-on dissection of the human body. The Venetian anatomist Niccolò Massa (c.1485–1569), in his Liber Introductorius Anatomiae of 1536, is frequently credited with one of the first clear post-classical descriptions of the prostate as a recognizable glandular body at the base of the bladder — predating, by a few years, the work for which the period is most famous.
That landmark work was De Humani Corporis Fabrica (1543) by Andreas Vesalius (1514–1564), the Flemish anatomist whose lavishly illustrated treatise overturned centuries of inherited Galenic error and founded modern anatomy. Vesalius depicted and described the glandular tissue surrounding the male urethra below the bladder, giving European medicine its first reliable, illustration-backed account of the organ's form and position. With Vesalius and his successors, the prostate finally became a stable, well-mapped structure rather than a vaguely-noted gland blurred together with the seminal vesicles.
From this Renaissance foundation, attention shifted from what the prostate is to what goes wrong with it. With the gland's normal anatomy firmly established, the physicians who followed could begin to describe its diseases — the swelling that blocked old men's urine, and, eventually, the cancer that grew within it.
Morgagni and the Recognition of Enlargement
That benign enlargement of the prostate causes the urinary misery of older men — a weak stream, frequent night-time trips, and sometimes a complete inability to pass urine — was clarified by the founder of modern anatomical pathology, Giovanni Battista Morgagni (1682–1771). In his monumental 1761 work De Sedibus et Causis Morborum per Anatomen Indagatis ("On the Seats and Causes of Diseases Investigated by Anatomy"), Morgagni correlated the findings of some 700 autopsies with the symptoms his patients had suffered in life. He was among the first to recognize clearly that diseases of the prostate are a problem of older men, and to tie the enlarged gland found at autopsy to the obstruction of urine that had tormented the living patient.
Morgagni's great methodological innovation — that careful dissection after death can explain the symptoms experienced in life — transformed prostate disease from a vague complaint of old age into an anatomically grounded condition with a visible cause. The growing gland pressing on the urethra was, at last, a mechanism one could see and reason about.
The surgical and medical management of this enlargement — later named benign prostatic hyperplasia (BPH) — would develop over the following two centuries, from crude instruments passed to relieve a blocked bladder, through the transurethral resection (TURP) operation, to the modern drug therapies that shrink or relax the gland. Because that story is rich enough to stand on its own, this overview points readers to the dedicated Benign Prostatic Hyperplasia page for the full account of how enlargement came to be treated.
The First Descriptions of Prostate Cancer
Prostate cancer is so common today that it is startling to learn how recently it was first clearly described. For most of medical history it went unrecognized, hidden among the general category of "tumours" and the urinary troubles of old age. The first detailed description from gross anatomy is generally credited to the London surgeon and pathologist George Langstaff (1780–1846). In a paper read in 1817, Langstaff reported the case of a 68-year-old man with a large tumour arising from the prostate that obstructed the urinary tract, together with what he took to be deposits in the liver — very likely the first recorded account of metastatic prostate cancer seen with the naked eye.
The first histologically confirmed case — that is, the first diagnosis proven by examining the diseased tissue under a microscope — came in 1853, when John Adams (1806–1877), a surgeon at The London Hospital, described a malignant growth of the prostate verified by microscopic examination. Adams famously remarked that the disease was "a very rare disease" — a striking comment given that prostate cancer is now among the most commonly diagnosed cancers in men. The contrast is not because the disease has become vastly more common, but because most cases once went undetected: men died with prostate cancer, not obviously of it, and without the microscope and modern testing it remained invisible.
Through the rest of the nineteenth and early twentieth centuries, prostate cancer was understood as a grim and largely untreatable condition. Surgery was hazardous, radiation was in its infancy, and there was no systemic therapy. What changed the entire field — and turned an incurable disease into a treatable one — was a discovery about hormones made in a Chicago laboratory in 1941.
Huggins and the Hormone Connection
In 1941, the surgeon-scientist Charles Brenton Huggins (1901–1997), working at the University of Chicago with his colleague Clarence V. Hodges, made one of the most consequential discoveries in the history of cancer medicine: that prostate cancer is hormone-dependent. Huggins showed that the growth of advanced prostate cancer could be dramatically slowed by lowering the level of male hormones (androgens, chiefly testosterone) in the body — either by surgically removing the testicles (castration) or by administering the female hormone estrogen, which suppresses testosterone. Conversely, giving androgens made the cancer worse.
The landmark 1941 paper by Huggins and Hodges, "Studies on Prostatic Cancer," demonstrated these effects by tracking blood enzyme levels (serum acid phosphatase) as a marker of disease activity. This was a revolutionary idea: that a cancer could be controlled not by cutting it out or burning it, but by manipulating the body's own hormonal environment. It was the first clear demonstration that any human cancer was dependent on a hormone — and it opened the entire field of endocrine cancer therapy.
For this work, Huggins was awarded the Nobel Prize in Physiology or Medicine in 1966 (sharing it with Peyton Rous, who was honoured for separate work on tumour-causing viruses). The principle Huggins established — now called androgen-deprivation therapy (ADT) — remains, more than eighty years later, the cornerstone of treatment for advanced and metastatic prostate cancer, although the crude tools of 1941 (surgical castration, high-dose estrogen) have been refined into far gentler modern hormonal drugs.
PSA: The Discovery of a Blood Test
If Huggins gave medicine a way to treat advanced prostate cancer, the discovery of prostate-specific antigen (PSA) gave it a way to detect the disease early — and, more controversially, to screen for it in men with no symptoms at all. PSA is a protein made almost exclusively by prostate tissue; small amounts leak into the bloodstream, and the level tends to rise when the prostate is enlarged, inflamed, or cancerous.
The protein was purified and characterized in a landmark 1979 study by Ming C. Wang and coworkers at Roswell Park Memorial Institute in Buffalo, New York, who isolated it from prostate tissue and recognized its potential as a marker of prostatic disease. (The history is genuinely tangled — several investigators detected prostate-associated antigens in the 1960s and 1970s, and scholars still debate priority — but Wang's 1979 purification is the work most directly tied to the clinical test that followed.) The crucial step from laboratory curiosity to a usable blood test came in 1987, when Thomas A. Stamey and colleagues, publishing in the New England Journal of Medicine, established PSA as a practical serum marker for prostate cancer — useful for detecting the disease and for following its response to treatment.
The United States Food and Drug Administration (FDA) first approved the PSA test in 1986 for monitoring men already diagnosed with prostate cancer — tracking whether treatment was working or the disease was returning. In 1994 the FDA approved PSA, used together with the digital rectal examination, as an aid in the early detection of prostate cancer in men without symptoms. That second approval launched the modern era of mass PSA screening — and with it, one of the most important and genuinely unresolved debates in preventive medicine.
The PSA-Screening Debate: Benefits and Harms
It would be dishonest to present PSA screening as a straightforward triumph, because it is not. The PSA test undeniably finds prostate cancers earlier, and after its introduction the number of prostate cancers diagnosed in the United States rose sharply. But finding more cancer is not the same as saving more lives, and this is the heart of a debate that thoughtful doctors still have today. This page lays out both sides fairly, because men deserve to make this decision with the real picture in front of them.
The case for screening: prostate cancer is common and can be deadly, and catching an aggressive tumour while it is still confined to the gland offers the best chance of cure. Large randomized trials — most notably the European ERSPC study — found that PSA screening reduced deaths from prostate cancer, and the fall in prostate-cancer mortality across many countries since the 1990s is at least partly attributed to earlier detection. For a man with a fast-growing cancer, early detection can genuinely be life-saving.
The case against indiscriminate screening: PSA is not specific to cancer — benign enlargement, infection, recent ejaculation, and even a bicycle ride can raise it — so it produces many false alarms, leading to biopsies that carry their own risks. More fundamentally, many prostate cancers grow so slowly that they would never have caused harm in a man's lifetime; detecting and treating them (a problem called overdiagnosis and overtreatment) can leave men with lasting incontinence or erectile dysfunction from surgery or radiation they never needed. Weighing this, the U.S. Preventive Services Task Force in 2012 recommended against routine PSA screening, then in 2018 softened that to a position of shared, individualized decision-making for men aged 55–69 — the current mainstream view. The honest bottom line, and the one major medical bodies now endorse, is that PSA screening is a personal decision a man should make in conversation with his clinician, weighing his own age, family history, and values — not an automatic test for everyone.
Diagnosis Today: Exam, Ultrasound, and Biopsy
The PSA blood test is only one of several tools that, together, make up the modern evaluation of the prostate — and each has its own history. The oldest is the digital rectal examination (DRE), in which a clinician feels the back wall of the prostate through the rectum to detect hardness, nodules, or asymmetry. Because the gland sits just in front of the rectum, this simple, centuries-old physical examination remains a genuinely useful first step, capable of detecting some cancers that PSA misses (and vice versa).
Imaging arrived in the later twentieth century. Transrectal ultrasound (TRUS), developed and refined from the 1970s and 1980s onward, uses a probe placed in the rectum to produce real-time images of the prostate, allowing doctors to estimate its size and, crucially, to guide a needle accurately into suspicious areas. The definitive diagnostic step is the prostate biopsy — taking small tissue cores so a pathologist can examine them under the microscope, exactly as John Adams did by hand in 1853, now done systematically under ultrasound (and increasingly MRI) guidance. The microscopic appearance is graded by the Gleason system, introduced by the pathologist Donald Gleason in the 1960s, which scores how aggressive the cancer looks and remains central to treatment decisions.
The modern pathway — PSA and DRE to raise suspicion, multiparametric MRI and ultrasound to localize it, and targeted biopsy with Gleason grading to confirm and stage it — is the product of every era described on this page, from Herophilus' first glimpse of the gland to twenty-first-century imaging. The detailed, practical guidance on what each test means for a patient lives on the dedicated Prostate Conditions overview and the PSA Test screening guide.
Research Papers and References
The references below are peer-reviewed sources on the history and discovery of the prostate and its diseases, supplemented with curated PubMed topic-search links into the medical-history literature. Historical primary texts (Galen on Herophilus, Vesalius' De Humani Corporis Fabrica, Morgagni's De Sedibus) are named in the article as historical sources rather than as modern citations. Each link opens in a new tab.
- Marx FJ, Karenberg A. History of the Term Prostate. The Prostate. 2009;69(2):208-213. — doi:10.1002/pros.20871
- Marx FJ, Karenberg A. Uro-words making history: ureter and urethra. The Prostate. 2010;70(9):952-958. — doi:10.1002/pros.21129
- Denmeade SR, Isaacs JT. A history of prostate cancer treatment. Nature Reviews Cancer. 2002;2(5):389-396. — doi:10.1038/nrc801
- Huggins C, Hodges CV. Studies on prostatic cancer. I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer Research. 1941;1:293-297. — PubMed: Huggins & Hodges 1941
- Benadada I, et al. Charles Brenton Huggins: a historical review of the Nobel laureate's pioneering discoveries. Cancer. 2024;130(6):857-866. — doi:10.1002/cncr.35173
- Catalona WJ. History of the discovery and clinical translation of prostate-specific antigen. Asian Journal of Urology. 2014;1(1):12-14. — doi:10.1016/j.ajur.2014.09.008
- Wang MC, Valenzuela LA, Murphy GP, Chu TM. Purification of a human prostate specific antigen. Investigative Urology. 1979;17(2):159-163. — PubMed: Wang et al. 1979
- Stamey TA, Yang N, Hay AR, McNeal JE, Freiha FS, Redwine E. Prostate-specific antigen as a serum marker for adenocarcinoma of the prostate. New England Journal of Medicine. 1987;317(15):909-916. — doi:10.1056/NEJM198710083171501
- Hajdu SI. A note from history: landmarks in history of cancer, part 3. Cancer. 2012;118(4):1155-1168. — doi:10.1002/cncr.26320
- Schröder FH, et al. Screening and prostate cancer mortality: results of the European Randomised Study of Screening for Prostate Cancer (ERSPC). The Lancet. 2014;384(9959):2027-2035. — doi:10.1016/S0140-6736(14)60525-0
- US Preventive Services Task Force. Screening for prostate cancer: US Preventive Services Task Force recommendation statement. JAMA. 2018;319(18):1901-1913. — doi:10.1001/jama.2018.3710
- Herophilus, the discovery of the prostate, and the anatomy of Alexandria — PubMed: Herophilus and the prostate
- George Langstaff (1817) and John Adams (1853): early descriptions of prostate cancer — PubMed: early history of prostate cancer
- Morgagni, De Sedibus (1761), and the history of benign prostatic enlargement — PubMed: Morgagni and prostatic enlargement
External Authoritative Resources
- National Cancer Institute — Prostate Cancer
- The Nobel Prize — Charles B. Huggins, Physiology or Medicine 1966
- PubMed — History of the prostate and PSA
Connections
- Urology
- Prostate Conditions (Overview)
- Benign Prostatic Hyperplasia (BPH)
- Erectile Dysfunction
- Low Testosterone & TRT
- PSA Test: Screening Guide
- Bladder Cancer
- All Conditions
- Prostate Cancer — modern diagnosis, staging, and treatment of the disease whose history is traced here.