Kidney Stones: History and Discovery
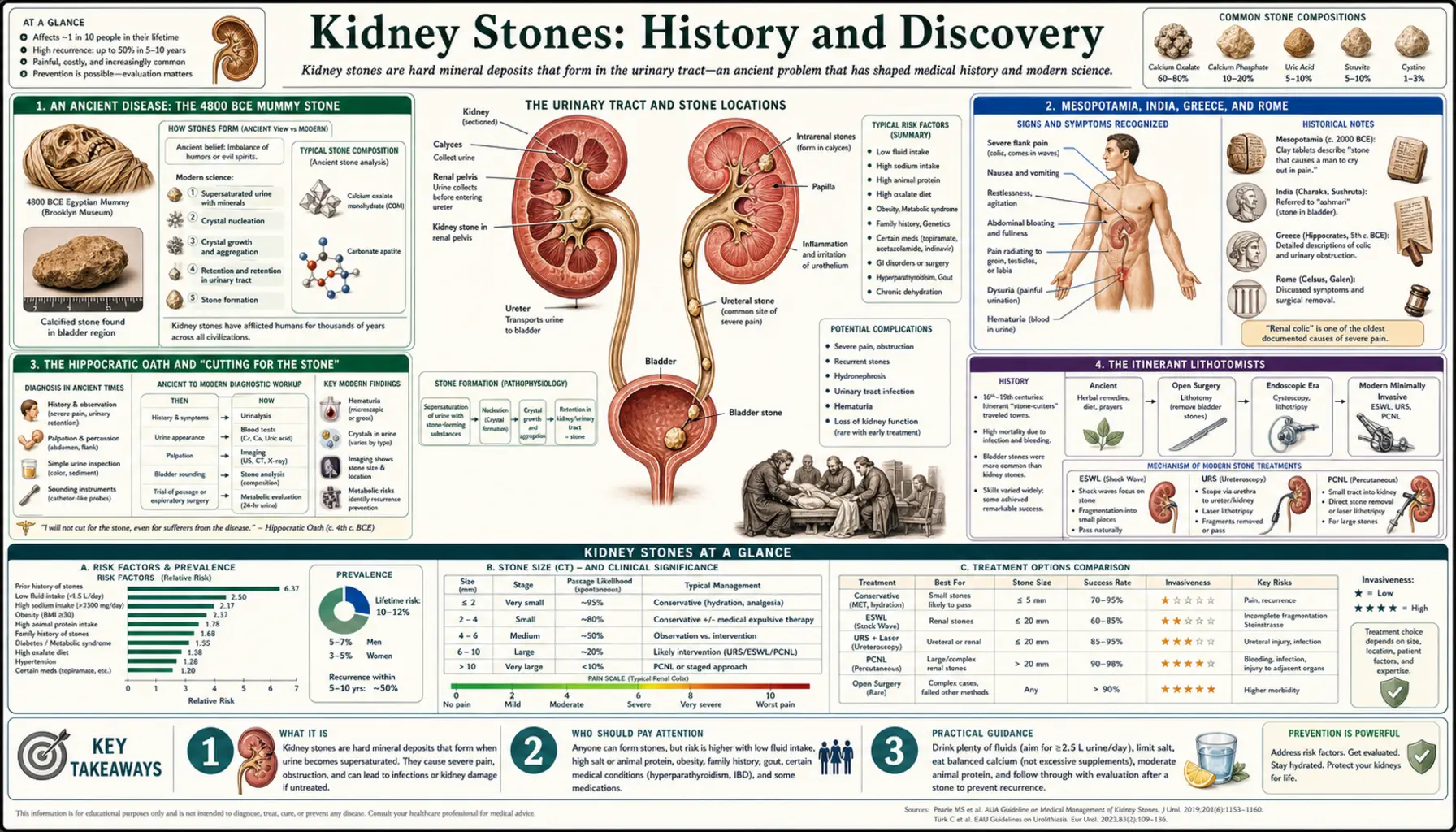
Urinary stone disease is one of the oldest documented illnesses of humankind — there is no single discoverer and no single "first." A bladder stone preserved in the pelvis of an Egyptian boy and dated to roughly 4800 BCE, recovered during excavation and presented to science by the anatomist G. Elliot Smith in 1901, is among the earliest physical evidence of any human disease. From that ancient stone runs an unbroken thread: the dread operation of "cutting for the stone," the wandering lithotomists who alone would perform it, the first instrument that crushed a stone without a knife, and finally the shock wave that, in 1980, began to dissolve the surgery itself. This page traces that history honestly, separating what is documented from what is merely supposed.
Table of Contents
- An Ancient Disease: The 4800 BCE Mummy Stone
- Mesopotamia, India, Greece, and Rome
- The Hippocratic Oath and "Cutting for the Stone"
- The Itinerant Lithotomists
- Crushing Without Cutting: Civiale and Lithotrity
- Seeing Inside: The Cystoscope
- The Shock Wave Revolution: ESWL, 1980
- Bladder Stones Versus Kidney Stones
- From Chemistry to Prevention
- Research Papers and References
- Connections
- Featured Videos
An Ancient Disease: The 4800 BCE Mummy Stone
Few diseases can be traced as far back as urinary stones. In the winter of 1900–1901, the Egyptologist Eric Peet's and Randall-MacIver's excavations at El-Amrah in Upper Egypt yielded the skeleton of an adolescent boy, and within his pelvis lay a urinary calculus. The specimen was studied by the anatomist Grafton Elliot Smith and presented in 1901; it was later described in detail by the pathologist Samuel Shattock. Radiologically and chemically the stone showed a uric-acid core wrapped in concentric layers of calcium oxalate and ammonium magnesium phosphate — a structure indistinguishable from stones formed today. Dated to roughly 4800 BCE, it is about seven thousand years old and stands among the very oldest physical specimens of any named human disease.
That single stone carries a second lesson. Elliot Smith, who over his career examined thousands of Egyptian mummies and skeletons, reported finding only a small number of bladder stones among them. Historians have read this as evidence that stone disease, while ancient, was not uniformly common in every era and place — its frequency rose and fell with diet, climate, hydration, and infection, exactly as it does in modern populations. The El-Amrah stone is therefore not merely a curiosity; it is the starting point of an epidemiological record that the rest of this page follows forward into the present.
It is worth being precise about what this find does and does not tell us. It proves that humans suffered urinary stones in the Neolithic; it does not tell us how that particular boy was treated, or whether he was treated at all. For that we must turn to the written record, which begins a little later and which describes both the agony of the disease and the earliest attempts to relieve it.
Mesopotamia, India, Greece, and Rome
Once writing appears, urinary stones appear with it. Mesopotamian and Egyptian medical texts of the second millennium BCE record symptoms consistent with painful urination and stone, and prescribe herbal and dietary remedies. The most remarkable early surgical record comes from India: the Sushruta Samhita, a Sanskrit treatise on surgery compiled in the centuries around the start of the common era, describes the perineal operation for removing a bladder stone in striking practical detail — the positioning of the patient, the incision, and the extraction — making Indian surgeons among the earliest documented practitioners of lithotomy anywhere in the world.
In the Greek world the disease was familiar enough to enter the foundational ethics of medicine, discussed in the next section. Greek and Roman physicians — among them the encyclopaedist Aulus Cornelius Celsus, whose first-century De Medicina gives a celebrated step-by-step account of perineal lithotomy — both described the stone and attempted to treat it with diet, baths, plant decoctions, and, when those failed, the knife. Celsus' description was so careful that the operation he outlined, later called the apparatus minor or "lesser apparatus," remained in use for more than a thousand years. These classical texts are named here as historical primary sources rather than as modern citations.
The Greco-Arabic physicians who inherited and extended this learning — including the great clinician Abu Bakr al-Razi (Rhazes) and the author of the Canon of Medicine, Ibn Sina (Avicenna) — wrote at length on the causes, prevention, and treatment of stones, refining diet-based management and surgical technique through the medieval centuries. Across all of these traditions one fact stands out: the disease was understood, dreaded, and operated upon long before anyone knew what a stone was made of or why it formed.
The Hippocratic Oath and "Cutting for the Stone"
One of the most famous lines in all of medicine concerns kidney and bladder stones. The classical Hippocratic Oath — the ethical pledge associated with the school of Hippocrates of Kos (c. 460–370 BCE) — contains a clause that, in Ludwig Edelstein's widely cited translation, reads: "I will not use the knife, not even on sufferers from stone, but will withdraw in favour of such men as are engaged in this work." In plain terms, the physician swore not to cut for the stone, but to leave that operation to others who specialised in it.
Why single out stone surgery? The consensus among historians is practical, not mystical. Perineal lithotomy — cutting into the perineum to reach the bladder — was, in an age with no anaesthesia and no understanding of infection, one of the most dangerous procedures a body could undergo: excruciatingly painful and frequently fatal from bleeding or sepsis. The Oath drew a line between the learned, mostly non-surgical physician and the hands-on operator, directing the patient to the latter. There is genuine scholarly debate about the clause — whether it referred to bladder stones specifically or to surgery more broadly, and how literally it was followed — and an honest history should flag that the exact original intent is not settled. What is not in doubt is the clause's lasting effect: for centuries, removing a stone was the province of a distinct, often itinerant, class of practitioners.
The Itinerant Lithotomists
Because the learned tradition shied away from the knife, "cutting for the stone" fell to specialist lithotomists — and many of the most famous were travelling operators who moved from town to town, set up for a few days, cut every waiting patient, and rode on. They worked fast of necessity: in the pre-anaesthetic era a perineal lithotomy lasted barely a minute or two, the patient held down by assistants. Skill, speed, and a strong stomach were everything; antisepsis lay centuries away.
The emblematic figure is Frère Jacques Beaulieu (1651–1719), a French itinerant lithotomist who, after an apparent religious conversion around 1690, adopted a monk's habit, called himself "Brother Jacques," and operated for small fees, often donating his earnings. Trained by apprenticeship to an Italian operator named Pauloni, he was among the first to champion the lateral perineal approach, which gave wider access to the bladder neck and to large stones. By the accounts that survive he performed on the order of several thousand lithotomies over roughly three decades and freely taught his technique to others — though his results carried heavy morbidity and mortality, and he was at times denied operating privileges. (The popular notion that the nursery rhyme "Frère Jacques" commemorates him is an enduring legend, not an established fact.)
The lateral lithotomy that Beaulieu helped popularise was carried to a high art in the following century by the English surgeon William Cheselden (1688–1752) at St Thomas' Hospital, who reportedly reduced the operation to well under a minute and achieved survival rates remarkable for the age. The era of the heroic lithotomist would end only when two innovations — an instrument that crushed the stone through the urethra, and later anaesthesia and antisepsis — made the bloody perineal cut unnecessary.
Crushing Without Cutting: Civiale and Lithotrity
The first true break with two thousand years of cutting came in Paris in the 1820s. The French surgeon Jean Civiale (1792–1867) reasoned that if a stone could be reached through the urethra and broken into fragments small enough to pass in the urine, the perineal incision — with all its danger — could be avoided altogether. He designed an instrument, the lithotrite (or litholabe), that was passed up the urethra to grasp and bore into the stone and then crush it. Civiale reported his early cases to the Paris Academy of Sciences on 22 March 1824, with his first such operation generally dated to January 1823. The technique was christened lithotrity (later litholapaxy when fragment-evacuation was added), and it is widely regarded as one of the first genuinely minimally invasive surgeries in history.
Civiale's contribution reaches beyond the operating room. To prove that lithotrity was safer than open lithotomy, he assembled large comparative tables of outcomes, and in 1835 the Academy of Sciences commissioned a statistical evaluation of stone surgery across Europe. The resulting debate over how to compare survival rates between two treatments is now cited as a milestone in the birth of evidence-based, statistical medicine — an early recognition that the right way to choose between operations is to count results, not to trust reputation. The instruments themselves were quickly refined by contemporaries such as Charles-Louis Heurteloup, whose percussion lithotrite of the early 1830s improved the crushing mechanism.
Seeing Inside: The Cystoscope
Crushing a stone blindly by feel was a great advance, but the operator still could not see what the instrument was doing. That changed with the development of the cystoscope — a lighted instrument for looking directly inside the living bladder. Early attempts at illuminated endoscopy date to Philipp Bozzini's Lichtleiter of around 1806, but the practical, usable cystoscope is generally credited to the German urologist Maximilian Nitze, who in 1879 (working with the Viennese instrument-maker Joseph Leiter) built a cystoscope incorporating an internal light source and lens optics. The arrival of Edison's incandescent bulb soon afterward made the instrument vastly safer and brighter.
Direct vision transformed stone surgery. A surgeon could now locate a stone precisely, guide instruments to it, and confirm that the bladder had been cleared — the foundation of modern transurethral and, eventually, ureteroscopic stone removal. Over the twentieth century the rigid cystoscope was joined by miniature ureteroscopes and flexible fibre-optic scopes able to travel up the ureter to the kidney itself, so that even stones high in the upper urinary tract could be reached and fragmented through the body's own passages, without any external incision.
The Shock Wave Revolution: ESWL, 1980
The single most dramatic milestone in the modern history of stone disease did not involve a knife or even an instrument inside the body. Extracorporeal Shock Wave Lithotripsy (ESWL) uses focused acoustic shock waves, generated outside the body and aimed through the skin, to fragment a kidney stone into sand-like pieces that the patient then passes naturally. The effect had been observed almost by accident: engineers at the German aerospace firm Dornier noticed that shock waves — of the kind studied in connection with high-speed flight and impact — could damage solid material inside a fluid without harming the surrounding soft tissue.
From 1974 a collaboration between Dornier (in Friedrichshafen, West Germany) and the Department of Urology and Institute for Surgical Research at the University of Munich, funded by the German government, turned that observation into a medical device, the Dornier HM1 lithotripter. On 7 February 1980 the team — Christian Chaussy with Bernd Forssmann and Dieter Jocham — treated the first kidney-stone patient with extracorporeal shock waves, a landmark reported by Chaussy and colleagues. The improved Dornier HM3, introduced in 1983–1984, made the technique a worldwide standard and, for a time, the default treatment for most kidney stones.
The consequence was a revolution in the patient's experience of stone disease. An illness whose treatment had meant, within living memory, a frightening operation and a long recovery could now often be handled without a single incision — in many cases on an outpatient basis. ESWL did not make stones painless, and it has its own limits (large, hard, or awkwardly placed stones are still better treated with ureteroscopy or percutaneous surgery), but it broke the ancient link between "stone" and "the knife" more completely than anything before it. Today ESWL, flexible ureteroscopy with laser fragmentation, and percutaneous nephrolithotomy together form a graded toolkit, chosen according to a stone's size, location, and composition.
Bladder Stones Versus Kidney Stones
An honest history must stress a distinction the modern public often misses: for most of recorded history, the stone that filled the operating tables was the bladder stone, not the kidney stone. The classic lithotomy patient of antiquity and the early-modern period was frequently a child — bladder stones were a disease of poor, malnourished boys in particular. This "endemic bladder stone" pattern was driven largely by infant diet: early weaning onto cereal pap low in protein and certain minerals, together with dehydration and recurrent infection, promoted stones that formed and grew in the bladder.
Over the nineteenth and twentieth centuries the endemic childhood bladder stone vanished from the developed world. Better infant nutrition, breastfeeding, dairy in the diet, clean water, and the control of infection removed the conditions that bred it — so thoroughly that a disease once ubiquitous in Europe is now rare there, persisting mainly in pockets of the developing world. As bladder stones receded, the upper-tract stone — the kidney and ureteric stone of the modern adult, driven by affluence, dehydration, obesity, and metabolic factors — rose to become the dominant form. The shift is real and well documented; a study from Pakistan, for instance, recorded the predominant stone location migrating from bladder to upper tract over little more than a decade.
This is why "kidney stones" today and "the stone" of history are related but not identical diseases. The agony of passing a stone is ancient and unchanged, but its typical victim has moved — from the malnourished child with a bladder stone to the well-fed, dehydrated adult with a stone lodged in the ureter. Keeping the two apart is essential to reading the historical record correctly.
From Chemistry to Prevention
The final chapter of the story is the one that turned stone disease from a surgical emergency into a largely preventable, manageable condition: understanding what stones are made of and why they form. As analytical chemistry matured, stones were sorted into types — calcium oxalate and calcium phosphate (by far the most common), uric acid, struvite (infection) stones, and the rare hereditary cystine stone — each with its own causes and its own prevention. The recognition that uric-acid stones share a metabolic neighbourhood with gout, and that both reflect how the body handles urate, tied stone medicine to nutrition and metabolism rather than to the operating theatre alone.
From that chemistry flowed the modern emphasis on prevention: drinking enough water to keep the urine dilute, moderating dietary salt and animal protein, ensuring adequate (not excessive) calcium, limiting very high-oxalate intake for those who form oxalate stones, and using targeted measures — citrate to raise urinary citrate, allopurinol to lower uric acid, urine alkalinisation to dissolve uric-acid stones — matched to the individual's stone type and 24-hour urine chemistry. Twenty-four-hour urine testing and stone analysis let physicians tailor prevention to the person, so that someone who has passed one stone need not simply wait, helpless, for the next.
Seen whole, the history of kidney stones is a record of steadily shrinking violence. The disease itself is essentially unchanged from the boy at El-Amrah seven thousand years ago; what has changed is everything around it. The dread perineal cut of the lithotomist gave way to Civiale's crushing instrument, then to the lighted cystoscope, then to the shock wave that needs no incision at all — and alongside the falling violence of treatment came the rising power of prevention, the ability to stop the next stone before it forms. The practical, present-day side of all this — symptoms, diagnosis, treatment options, and prevention — is covered on the main Kidney Stones page.
Research Papers and References
The references below combine peer-reviewed historical reviews of urinary-stone disease with curated PubMed topic-search links into the relevant literature. Classical primary texts (the Hippocratic Oath, Celsus' De Medicina, the Sushruta Samhita, and the writings of al-Razi and Ibn Sina) are named in the article as historical sources rather than as modern citations. Each search link opens at PubMed (U.S. National Library of Medicine) in a new tab.
- Tefekli A, Cezayirli F. The history of urinary stones: in parallel with civilization. The Scientific World Journal. 2013;2013:423964. — doi:10.1155/2013/423964
- López M, Hoppe B. History, epidemiology and regional diversities of urolithiasis. Pediatric Nephrology. 2010;25(1):49-59. — doi:10.1007/s00467-008-0960-5
- Herr HW. 'Cutting for the stone': the ancient art of lithotomy. BJU International. 2008;101(10):1214-1216. — doi:10.1111/j.1464-410X.2008.07510.x
- Herr HW. 'I will not cut…': the oath that defined urology. BJU International. 2008;102(7):769-771. — doi:10.1111/j.1464-410X.2008.07796.x
- Herr HW. 'Crushing the stone': a brief history of lithotripsy, the first minimally invasive surgery. BJU International. 2008;102(4):432-435. — doi:10.1111/j.1464-410X.2008.07639.x
- Chaussy C, Brendel W, Schmiedt E. Extracorporeally induced destruction of kidney stones by shock waves. The Lancet. 1980;2(8207):1265-1268. — doi:10.1016/S0140-6736(80)92335-1
- Romero V, Akpinar H, Assimos DG. Kidney stones: a global picture of prevalence, incidence, and associated risk factors. Reviews in Urology. 2010;12(2-3):e86-e96. — PMC2931286
- Hippocratic Oath — the lithotomy clause and its interpretation — PubMed: Hippocratic Oath and cutting for stone
- Frère Jacques Beaulieu and the itinerant lithotomists — PubMed: Beaulieu and historical lithotomy
- Jean Civiale, lithotrity, and the dawn of statistical medicine — PubMed: Civiale, lithotrity and statistics
- History and development of the cystoscope (Nitze, Leiter, Bozzini) — PubMed: history of the cystoscope
- Extracorporeal shock wave lithotripsy — history and development — PubMed: history of ESWL
- Endemic bladder stone disease of childhood and its decline — PubMed: endemic childhood bladder stone
- Stone composition, metabolism, and the prevention of recurrent urolithiasis — PubMed: stone composition and prevention
External Authoritative Resources
- EAU European Museum of Urology — Cutting for the Stone
- NIDDK (NIH) — Kidney Stones
- PubMed — All research on the history of urolithiasis
Connections
- Urology
- Kidney Stones (main page)
- All Conditions
- Urinary Tract Infections
- Kidney Disease
- Gout (uric-acid stones)
- Chanca Piedra (the "stone breaker" herb)
- Chanca Piedra Kidney-Stone Protocol