Erectile Dysfunction: History and Discovery
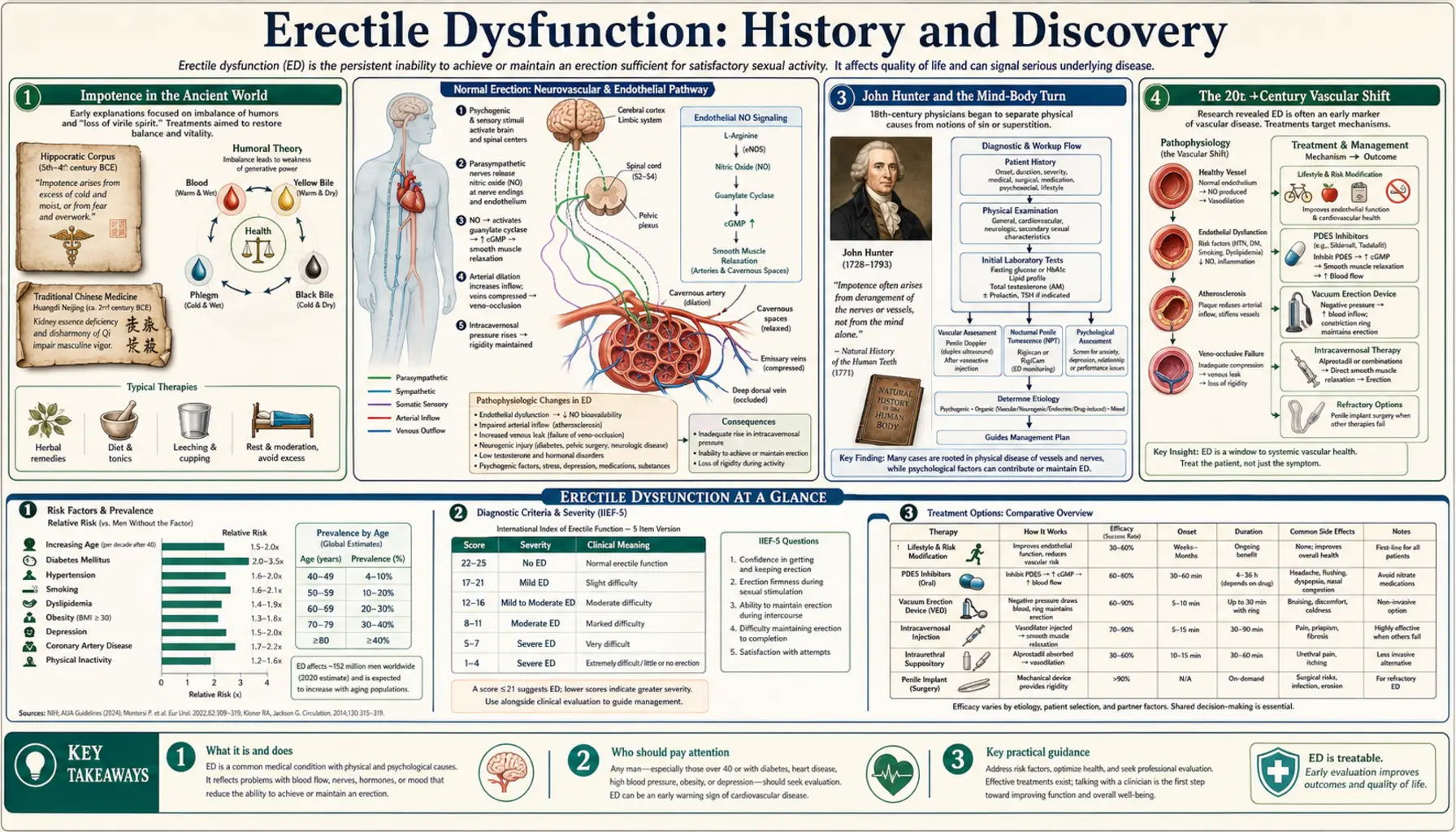
Few human complaints have a longer written record — or a stranger one — than the inability to achieve an erection. Discussed in ancient Egyptian, Greek, and Chinese medical texts and referenced in the Bible, “impotence” was for most of recorded history blamed on psychological weakness, divine punishment, or sorcery; medieval European witch-hunters treated bewitched impotence (maleficium) as a documented crime. The modern story is one of a steady shift from the supernatural and the purely psychological toward a physical, vascular understanding of the penis as a blood-flow organ — a shift that culminated in a single decade with self-injection therapy, the renaming of the condition itself, and the accidental discovery of an oral pill, sildenafil (Viagra), approved in March 1998, that transformed both medicine and public conversation.
Table of Contents
- Impotence in the Ancient World
- Sin, Sorcery, and Medieval Maleficium
- John Hunter and the Mind-Body Turn
- The 20th-Century Vascular Shift
- Injection Therapy: Virag, Brindley, and 1983
- Vacuum Devices and Penile Implants
- Renaming the Condition: The 1992 NIH Consensus
- The Accidental Pill: Sildenafil and Viagra
- Legacy and the Modern Understanding
- Research Papers and References
- Connections
- Featured Videos
Impotence in the Ancient World
The inability to achieve or sustain an erection is one of the oldest documented medical complaints. Descriptions appear in ancient Egyptian medical writing dating to roughly the second millennium BCE, where the condition was distinguished into a “natural” form — a failure of the body — and a “supernatural” form attributed to hostile magic or demonic influence. Egyptian physicians recorded aphrodisiac preparations, ointments, and protective spells intended to restore lost potency, weaving together what we would now separate into medicine and ritual.
The theme recurs across the ancient world. Classical Greek and Roman writers discussed impotence and prescribed for it; the Hippocratic and later Galenic traditions framed sexual function within humoral balance, and aphrodisiacs and dietary remedies feature throughout the classical materia medica. Traditional Chinese medical texts addressed loss of male sexual function within their own framework of jing (essence) and kidney vitality, prescribing tonics and herbs to replenish what was thought to be depleted. The Bible, too, references barrenness and the loss of generative power. For accessibility these ancient and scriptural sources are named here as historical primary records rather than as modern citations.
What unites these widely separated cultures is a frame of mind very different from our own. With no concept of blood pressure, vascular tone, or nerve signaling, ancient observers reached for explanations rooted in spirit, balance, diet, and the will. Impotence was understood as something done to a man — by the gods, by an enemy’s curse, by a depletion of vital essence — or as a failure of his own desire and resolve. That interpretive lens, far more than any specific remedy, is the ancient inheritance the next two millennia would slowly have to overturn.
Sin, Sorcery, and Medieval Maleficium
In medieval and early-modern Europe the psychological and supernatural framing hardened into something with real legal and religious weight. Within Christian moral theology, the marriage act was central to the validity of a marriage, so the inability to consummate — impotentia — became a matter for canon law and the church courts, which could examine, adjudicate, and even annul on the grounds of incurable impotence. Potency was thus not merely a private misfortune but a public, juridical fact.
More striking to modern eyes is the era’s firm belief that impotence could be inflicted by witchcraft. The Latin term maleficium — harmful sorcery — explicitly covered the magical “binding” of a man so that he could not perform with his wife. The notorious late-fifteenth-century witch-hunting manual Malleus Maleficarum (“Hammer of Witches,” 1486) devotes attention to witches who were believed to cause impotence and even, in its lurid framing, to make the male member appear to vanish. Bewitched impotence was treated as a genuine, prosecutable harm; remedies ran to prayer, exorcism, pilgrimage, and counter-charms rather than to anything we would call medicine.
It is worth being clear that this is the history of a belief, not of a mechanism: no one was ever made impotent by a curse. But the maleficium episode matters because it shows how completely, for centuries, a physical and treatable condition was absorbed into frameworks of sin, supernatural attack, and moral failing. Untangling erectile failure from shame and superstition — rather than discovering a drug — would turn out to be one of the longest tasks in this story, and one not finished until the late twentieth century.
John Hunter and the Mind-Body Turn
The Scottish surgeon and anatomist John Hunter (1728–1793), one of the founders of scientific surgery, is an important transitional figure. In his A Treatise on the Venereal Disease (1786) Hunter discussed impotence directly and, crucially, separated cases arising from physical disease from those arising “entirely from the state of the mind.” In a frequently cited passage he described counseling a patient by telling him he could be cured if he would, for a set period, deliberately refrain from attempting intercourse — removing the anxiety of performance so that natural function could reassert itself. The man, freed from the pressure to succeed, recovered.
Hunter’s account is remarkable for two reasons. First, it is an early, lucid articulation of what we would now call psychogenic erectile dysfunction and of performance anxiety as a self-reinforcing trap — an insight that anticipates twentieth-century sex therapy by nearly two hundred years. Second, by insisting that some impotence is bodily and some is mental, and that the two demand different approaches, Hunter helped pull the condition out of the moral-supernatural frame and into the domain of clinical observation. His was not yet a vascular theory; the engine driving the erection was still a mystery. But the questions had become medical ones, asked at the bedside, which is precisely where the nineteenth and twentieth centuries would pick them up.
The 20th-Century Vascular Shift
For erectile dysfunction to become a treatable medical problem, the erection itself had to be understood as a physical event — specifically, as a matter of blood flow. The penis is a hydraulic organ: erection occurs when the smooth muscle lining its spongy erectile chambers (the paired corpora cavernosa) relaxes, allowing arterial blood to rush in and engorge the tissue while the swelling compresses the outflow veins and traps the blood under pressure. This is a vascular and neuromuscular cascade, not an act of will. Recognizing it as such was the single most important conceptual change in the entire history of the condition.
This understanding assembled gradually across the twentieth century. Anatomists and physiologists mapped the penile arteries, the cavernosal smooth muscle, and the nerves that govern them; clinicians came to appreciate that conditions which damage blood vessels or nerves — atherosclerosis, diabetes, high blood pressure, pelvic surgery, spinal injury — commonly produce erectile failure, and that the great majority of long-standing cases are organic (physical) rather than purely psychological. By the second half of the century the field had largely inverted the ancient assumption: instead of treating impotence as a disorder of the mind by default, physicians increasingly saw failing erections as a window onto the health of a man’s blood vessels and nerves — sometimes the first warning sign of cardiovascular disease.
It is fair to mark some of the finer mechanistic detail as comparatively recent. The central role of nitric oxide as the signaling molecule that relaxes penile smooth muscle, and of the second messenger cyclic GMP that carries that signal, was worked out only in the late 1980s and early 1990s — the same nitric-oxide biology recognized by the 1998 Nobel Prize in Physiology or Medicine. That discovery is not a loose hypothesis but established pharmacology, and, as the next sections show, it is exactly the chemistry the modern therapies act upon. Where any specific causal claim here remains a working hypothesis rather than settled fact, it should be read as such; the broad vascular model of erection, however, is firmly established.
Injection Therapy: Virag, Brindley, and 1983
The vascular model produced the first genuinely effective modern treatments, and they arrived not as pills but as injections directly into the erectile tissue. In 1982 the French vascular surgeon Ronald Virag reported in The Lancet that injecting the smooth-muscle relaxant papaverine into the corpus cavernosum produced an erection — an observation he traced to an accidental intracavernosal injection during vascular surgery that had unexpectedly caused a sustained erection. Virag’s brief report demonstrated, for the first time, that an erection could be reliably switched on by a drug acting locally on penile blood flow, and it founded the field of intracavernosal injection therapy.
The discovery’s most famous moment, however, belongs to the British physiologist Giles Brindley. At the 1983 meeting of the Urodynamics Society in Las Vegas, Brindley reported his own work on intracavernosal injection of vasoactive drugs to induce erection — and, in a now-legendary demonstration, having injected himself with papaverine beforehand, he stepped from behind the podium to exhibit the result to a stunned audience. The event was recounted years later in a widely read first-person memoir by the urologist Laurence Klotz, an attendee, and it has become the field’s defining anecdote precisely because it dramatized, unforgettably, that erection was now a controllable pharmacological event.
Beyond the spectacle, injection therapy was a real clinical advance. Papaverine, later refined to combinations and ultimately to alprostadil (prostaglandin E1, the basis of FDA-approved injectable and intraurethral products in the mid-1990s), gave urologists the first dependable, on-demand treatment for organic erectile dysfunction. It remains in use today for men who do not respond to oral drugs. Injection therapy also proved the principle that an oral agent would later exploit: if you can relax penile smooth muscle and open its blood flow, you can restore an erection regardless of desire or willpower.
Vacuum Devices and Penile Implants
Alongside the pharmacological line ran a mechanical one. The idea of drawing blood into the penis with suction is surprisingly old: in 1874 the American physician John King described a “glass exhauster” that produced an artificial erection by vacuum. The modern vacuum erection device — a cylinder that pulls blood into the penis, after which a constriction ring at the base traps it — was commercialized in the United States in the 1970s by the Georgia businessman Geddings D. Osbon Sr., who marketed it widely; such devices received U.S. Food and Drug Administration clearance for erectile dysfunction in the 1980s. Non-invasive and drug-free, the vacuum device remains a standard option, particularly after prostate surgery.
The most definitive mechanical solution is the surgically implanted penile prosthesis. Rigid and semi-rigid rod implants were tried earlier, but the breakthrough came in 1973 when the urologists F. Brantley Scott, William Bradley, and Gerald Timm introduced the inflatable penile prosthesis — hydraulic cylinders implanted in the corpora cavernosa, filled on demand from a concealed fluid reservoir via a pump in the scrotum, producing a controllable erection and then deflating. Made practical by medical-grade silicone, the inflatable prosthesis was a landmark in reconstructive urology and, in steadily improved forms, remains the most reliable treatment for severe, drug-resistant erectile dysfunction.
These device-based approaches matter to the larger history because they reinforced, from the engineering side, the same lesson the injections taught from the pharmacological side: erection is a mechanical, blood-flow phenomenon that can be produced by physical means. By the early 1980s a man with organic erectile dysfunction had, for the first time, several genuinely effective options — injections, a vacuum pump, or an implant. What no one yet had was a simple pill. Two converging developments — a change in language and a serendipitous laboratory finding — would supply the rest.
Renaming the Condition: The 1992 NIH Consensus
In December 1992 the U.S. National Institutes of Health convened a Consensus Development Conference on the condition then still officially called “impotence.” The panel’s report made a recommendation that proved quietly historic: the term “erectile dysfunction” should replace “impotence.” The older word, the panel reasoned, was imprecise — it had been used loosely for everything from low desire to infertility — and, worse, it carried a heavy freight of stigma, implying a global failure of manhood rather than a specific, often treatable, problem of erection.
The change was more than cosmetic. “Erectile dysfunction” is descriptive and neutral: it names a particular physiological function that is not working, the way one might speak of a thyroid or a kidney problem, and it can be graded and measured. The conference also confronted the era’s persistent silence around the topic, noting that embarrassment on the part of patients and the reluctance of both men and clinicians to discuss sexual matters openly led to widespread under-diagnosis of a common and manageable condition. In effect, the panel diagnosed the shame as part of the disease’s burden.
Renaming the condition helped complete the long arc this page has traced — the journey from maleficium and moral failing to a medical diagnosis a man could discuss with his doctor without disgrace. The timing was fortunate. Within a few years an oral treatment would arrive and be marketed openly, on television, to the general public; the destigmatized clinical vocabulary established in 1992 was precisely what made that public conversation possible. The new word and the new pill reinforced each other.
The Accidental Pill: Sildenafil and Viagra
The drug that changed everything was not designed for erectile dysfunction at all. In the late 1980s, scientists at Pfizer’s research site in Sandwich, England, were developing a compound coded UK-92480 — later named sildenafil — as a treatment for angina, the chest pain of coronary heart disease. The rationale was sound vascular pharmacology: sildenafil inhibits an enzyme called phosphodiesterase type 5 (PDE5), which breaks down cyclic GMP, the very messenger that relaxes vascular smooth muscle. By blocking its breakdown, the drug should prolong cGMP’s vessel-relaxing action and, the hope was, ease the heart’s blood supply.
As a heart drug it underwhelmed. In early-1990s clinical trials — the program is associated with Pfizer researcher Ian Osterloh, a co-author of the authoritative scientific account of the drug’s history — sildenafil’s effect on angina proved modest. But male volunteers, including participants in trials in South Wales, reported an unexpected and consistent side effect: penile erections. The reason, in hindsight, was elegant: PDE5 is highly concentrated in penile erectile tissue, so a drug that preserves cGMP there powerfully amplifies the natural nitric-oxide signal that relaxes cavernosal smooth muscle and admits blood — exactly the nitric-oxide / cGMP pathway worked out in those same years. Pfizer, recognizing what it had, redirected the entire program from the heart to erectile dysfunction.
The redirected development succeeded spectacularly. On March 27, 1998, the U.S. Food and Drug Administration approved sildenafil, marketed as Viagra — the first effective oral pill for erectile dysfunction. Its impact is hard to overstate: an on-demand tablet that worked with sexual stimulation rather than requiring an injection, a pump, or surgery, it was an immediate commercial phenomenon and, just as importantly, a cultural one. Advertised openly and discussed in the press, “the little blue pill” dragged a long-hidden condition into ordinary conversation, accelerated the destigmatization the 1992 renaming had begun, and opened the modern era of PDE5-inhibitor therapy (later joined by tadalafil and vardenafil). Sildenafil’s own story did not end there: the same vascular action led to its approval, under the name Revatio, for pulmonary arterial hypertension — a fitting coda for a heart drug that became a sexual-medicine landmark.
Legacy and the Modern Understanding
The history of erectile dysfunction is, at bottom, the history of an idea slowly correcting itself. For thousands of years a physical, vascular problem was misread as a failure of spirit, virtue, or will, or as the work of curses; the cures were spells, penances, and shame. Only in the twentieth century did the erection come to be understood for what it is — a controllable event of blood flow governed by nerves, smooth muscle, and chemical messengers — and only then could real treatments follow. The injection demonstrations of 1982–83, the inflatable prosthesis, the vacuum device, the renaming of the condition in 1992, and the accidental pill of 1998 are all chapters of that single correction.
The modern legacy is twofold. Clinically, erectile dysfunction is now recognized as a sentinel of vascular health: because the penile arteries are small, they often clog before the larger coronary arteries do, so new-onset erectile dysfunction in a middle-aged man is frequently an early warning of atherosclerosis, diabetes, or other cardiovascular disease and a prompt to assess the whole body, not just the symptom. Culturally, the condition has moved from the unspeakable to the routinely advertised — a transformation that lets millions of men seek help they once suffered in silence.
For readers, the practical takeaways of this history are worth stating plainly. Erectile dysfunction is common, it is medical, and it is treatable — and, importantly, it can be a meaningful clue to a man’s heart and blood-vessel health, which is why it deserves a real evaluation rather than only a prescription. The detailed causes, modern diagnosis, and full range of treatments are covered in the main Erectile Dysfunction article, with closely related material on low testosterone and on atherosclerosis. This page is historical background; it is not medical advice, and anyone troubled by erectile difficulty should see a clinician, both for effective treatment and because of what the symptom may reveal.
Research Papers and References
The references below combine peer-reviewed historical and scientific sources with curated PubMed topic-search links into the history of erectile dysfunction and its treatments. Historical primary texts (ancient Egyptian, Greek, biblical, and Chinese medical writings; the Malleus Maleficarum; and John Hunter’s A Treatise on the Venereal Disease) are named in the article as historical sources rather than as modern citations. Direct citations with a DOI link open the publisher record; PubMed topic links open at the National Library of Medicine. All external links open in a new tab.
- Ghofrani HA, Osterloh IH, Grimminger F. Sildenafil: from angina to erectile dysfunction to pulmonary hypertension and beyond. Nature Reviews Drug Discovery. 2006;5(8):689-702. — doi:10.1038/nrd2030
- Virag R. Intracavernous injection of papaverine for erectile failure. The Lancet. 1982;2(8304):938. — doi:10.1016/S0140-6736(82)90910-2
- Klotz L. How (not) to communicate new scientific information: a memoir of the famous Brindley lecture. BJU International. 2005;96(7):956-957. — doi:10.1111/j.1464-410X.2005.05797.x
- NIH Consensus Development Panel on Impotence. Impotence. JAMA. 1993;270(1):83-90 (NIH Consensus Conference, December 7–9, 1992; recommended “erectile dysfunction” replace “impotence”). — PubMed: NIH Consensus on Impotence (PMID 8510302)
- Consensus development conference statement. National Institutes of Health. Impotence. December 7–9, 1992. — PubMed: NIH Impotence consensus statement (PMID 8173631)
- History of the inflatable penile prosthesis (Scott, Bradley, and Timm, 1973) and historical ED treatments. — PubMed: inflatable penile prosthesis history
- A comprehensive history of injection therapy for erectile dysfunction. — PubMed: history of intracavernosal injection therapy
- Erectile dysfunction: historical perspectives and the evolution of treatment. — PubMed: erectile dysfunction / impotence history
- Impotence in antiquity and the history of sexual medicine. — PubMed: impotence in antiquity and the history of sexual medicine
- Nitric oxide and cyclic GMP signaling in penile erection. — PubMed: nitric oxide and cGMP in penile erection
- Phosphodiesterase type 5 (PDE5) inhibitors: pharmacology and clinical development. — PubMed: PDE5 inhibitors and erectile dysfunction
- Sildenafil (Viagra): discovery, development, and clinical use. — PubMed: sildenafil discovery and development
- Erectile dysfunction as a marker of cardiovascular disease. — PubMed: erectile dysfunction as a cardiovascular marker
- Vacuum erection devices for erectile dysfunction: history and clinical use. — PubMed: vacuum erection device history
External Authoritative Resources
- NIDDK (National Institutes of Health) — Erectile Dysfunction
- MedlinePlus — Erectile Dysfunction
- PubMed — All research on the history of erectile dysfunction
Connections
- Urology
- Erectile Dysfunction (main article)
- Low Testosterone and TRT
- Benign Prostatic Hyperplasia
- Atherosclerosis
- All Conditions