Bipolar Disorder: History and Discovery
The history of bipolar disorder is a two-thousand-year story of physicians noticing that the same person could swing between two opposite states — the soaring energy of mania and the heavy darkness of melancholia. Ancient Greek writers, above all Aretaeus of Cappadocia (1st–2nd century CE), suspected the two were linked. The modern illness, though, was born in nineteenth-century France, where Jean-Pierre Falret (1851) and Jules Baillarger (1854) each described a single disease in which mania and depression alternate. Emil Kraepelin unified these threads as “manic-depressive insanity” in 1899; Karl Leonhard drew the bipolar-versus-unipolar line in 1957; and the term bipolar disorder entered the DSM in 1980. Along the way, the Australian psychiatrist John Cade found lithium’s calming effect on mania (published 1949) — a founding moment of modern psychiatric medicine. This page traces that path honestly, separating what the ancients observed from what later science established.
Table of Contents
- A Two-Thousand-Year Observation
- Aretaeus and the Ancient Link Between Mania and Melancholia
- From the Middle Ages to the Eve of Psychiatry
- The French Birth of the Modern Concept (1851–1854)
- Kraepelin and Manic-Depressive Insanity (1899)
- Leonhard, the Bipolar–Unipolar Split, and the Spectrum
- John Cade, Lithium, and the Birth of Psychopharmacology
- Naming the Illness: From DSM-III to Today
- Language, Stigma, and What the History Teaches
- Research Papers and References
- Connections
- Featured Videos
A Two-Thousand-Year Observation
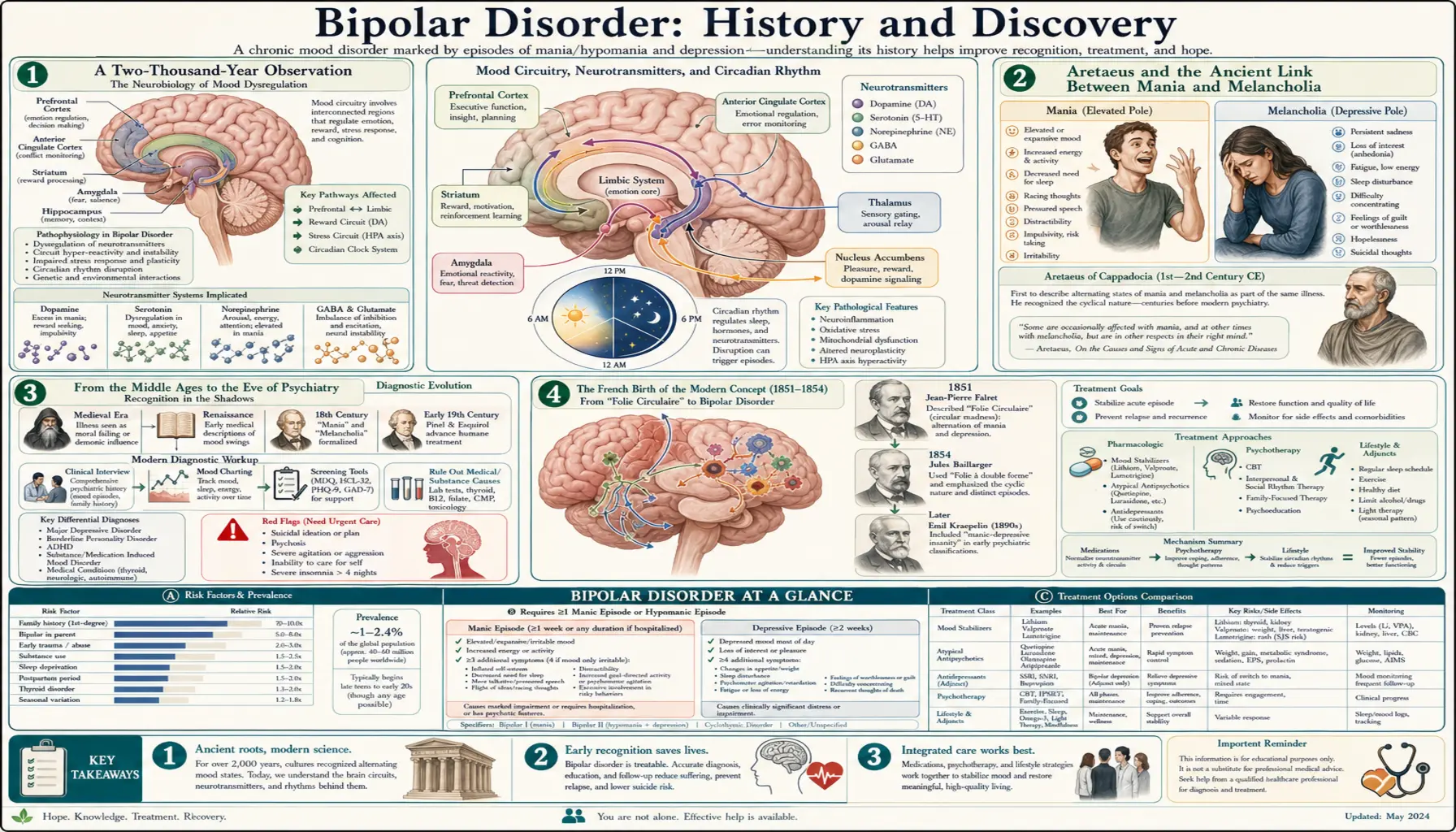
Bipolar disorder is defined by episodes at two opposite poles of mood and energy: mania or hypomania (elevated, expansive, or irritable mood with surplus energy, reduced need for sleep, and fast thought) and depression (low mood, loss of interest, fatigue, and slowed thinking). What makes the condition distinctive — and what observers across millennia kept rediscovering — is that these opposite states appear in the same person, often separated by stretches of relatively normal mood. The central historical question was never whether mania and melancholia existed, but whether they were two diseases or two faces of one.
That question has a surprisingly long pedigree. Ancient physicians described both states vividly and, in at least one influential case, proposed they were connected. The idea then lay largely dormant for centuries before being revived, refined, and finally formalised by nineteenth- and twentieth-century clinicians with the benefit of careful long-term observation of patients in asylums and clinics. The arc runs from a hypothesis grounded in the humoral theory of black bile, through systematic clinical description, to a modern diagnosis anchored in the observed course of illness and, eventually, in treatment response.
A history written for a general audience has a duty to be precise about who observed what and when, because the temptation to project the modern diagnosis backward onto every ancient mention of madness is strong and misleading. The sections below distinguish three things that are often blurred together: the ancient intuition that mania and melancholia are related; the nineteenth-century concept of a single cyclical illness; and the modern bipolar/unipolar distinction underlying today’s diagnostic manuals.
Aretaeus and the Ancient Link Between Mania and Melancholia
The earliest detailed surviving link between mania and melancholia comes from Aretaeus of Cappadocia, a Greek physician usually dated to the first or second century CE who practised in the Greco-Roman medical tradition. In his clinical writings he described both melancholia and mania in memorable detail, and — crucially — he proposed that they were not two separate illnesses but two forms of one and the same disease. This is why Aretaeus is so often cited as a distant ancestor of the bipolar concept.
Honesty about the detail matters here. Aretaeus did not describe modern “bipolar disorder,” and he framed the relationship within the humoral medicine of his day, in which both states were traced to black bile (the Greek roots melan-, black, and -cholē, bile, survive in the word melancholia). In his account, mania was understood as a more intense or advanced expression of melancholia rather than as a distinct opposite pole — a framing that differs from how we think today, where mania and depression are seen as contrasting states of one illness. The enduring, verifiable contribution is the unifying intuition: that the manic patient and the melancholic patient might be suffering from a single underlying condition.
It is worth noting that earlier Greek medicine, in the Hippocratic tradition, had already named mania and melancholia and tied disturbances of mood to the balance of the four humours; Aretaeus inherited and sharpened that framework. He should therefore be read as the clearest ancient voice for a connection, not as a lone inventor of the idea. For a free public-health page, the responsible summary is simple: the suspicion that mania and depression belong together is ancient, but the disciplined description of an alternating, recurring single illness — the thing we now call bipolar disorder — is a product of the nineteenth century.
From the Middle Ages to the Eve of Psychiatry
For many centuries after antiquity, the humoral model of mania and melancholia passed largely intact through Byzantine, Islamic, and medieval European medicine. Physicians kept describing excited and depressed states, and some noted cases in which the two seemed to follow one another in the same patient, but the ancient suggestion of a single cyclical disease was not systematically developed. Madness in this long era was understood through a shifting mix of humoral theory, religious interpretation, and moral judgement, and the careful longitudinal tracking of one person’s mood over years — the observation the diagnosis ultimately depends on — was rare.
The intellectual ground began to shift in the eighteenth and early nineteenth centuries with the rise of clinical psychiatry (then often called “alienism”) and the asylum. As reform-minded physicians began to observe and record patients over long periods, the recurring, episodic nature of certain mood illnesses became harder to miss. This was the setting in which French clinicians, working in large Parisian asylums with the chance to follow patients for years, were finally positioned to convert the ancient intuition into a defined disease. The decisive step came in the early 1850s.
The French Birth of the Modern Concept (1851–1854)
The modern illness was, in a meaningful sense, born in France. In 1851, the French psychiatrist Jean-Pierre Falret (1794–1870) described what he called la folie circulaire — “circular insanity.” Falret’s key insight was that mania, depression, and intervals of normal mood could form a single, repeating cycle within one patient, with the lucid intervals between episodes varying in length. By treating the alternation itself as the disease, rather than treating each manic or depressive episode in isolation, Falret produced what is widely regarded as the first description of bipolar disorder as a unified, recurring condition.
Three years later, in 1854, his colleague Jules Baillarger (1809–1890) presented a closely related concept he named la folie à double forme — “dual-form insanity.” Baillarger emphasised an illness in which mania and melancholia transform into one another as two phases of a single attack. The two Frenchmen’s formulations were not identical, and there was a priority dispute between them. The most-cited distinction is the role of the symptom-free interval: Falret’s folie circulaire built the recurring lucid interval into the cycle, whereas Baillarger’s folie à double forme stressed the direct succession of the two phases without requiring a normal interval between them.
Whatever the differences, the combined effect of the 1851 and 1854 publications was decisive: by the latter part of the nineteenth century, European psychiatry had broadly accepted the existence of a single illness defined by alternating mania and depression. The ancient hypothesis of a link had become a clinical entity with a course, a name, and a recognised pattern. What it still lacked was a place within a comprehensive classification of mental illness — the contribution of Emil Kraepelin.
Kraepelin and Manic-Depressive Insanity (1899)
The German psychiatrist Emil Kraepelin (1856–1926) gave the illness its enduring twentieth-century shape. Working from the systematic long-term follow-up of large numbers of patients, Kraepelin organised the major non-organic psychoses into two great categories in the influential sixth edition of his textbook Psychiatrie (1899). On one side he placed dementia praecox (later renamed schizophrenia by Eugen Bleuler), which he characterised by progressive deterioration and poor outcome. On the other he placed manic-depressive insanity (manisch-depressives Irresein), into which he folded the various circular, recurrent, and periodic mood illnesses — including the French folie circulaire — as well as much of what we would today call recurrent depression.
Kraepelin’s organising principle was not a snapshot of symptoms but the course and outcome of the illness over time. The crucial contrast he drew was that manic-depressive insanity, however severe its episodes, tended toward periods of remission and even full recovery between attacks, whereas dementia praecox tended toward steady decline. This division — later nicknamed the Kraepelinian dichotomy — became the backbone of psychiatric classification for more than a century and still shapes how the diagnostic manuals separate mood disorders from the schizophrenia spectrum.
One honest caveat carries forward to the present: Kraepelin’s “manic-depressive insanity” was broader than today’s bipolar disorder, because it grouped recurrent unipolar depression together with the bipolar (manic-and-depressed) cases. Disentangling those two groups was the work of the next major figure in the story, and it is the reason the modern diagnosis is defined as much by the presence of mania as by the presence of depression.
Leonhard, the Bipolar–Unipolar Split, and the Spectrum
The distinction that gives the modern diagnosis its name came from the German psychiatrist Karl Leonhard (1904–1988). In 1957, building on and re-evaluating Kraepelin’s broad category, Leonhard introduced the contrast between bipolar mood disorders — those with both manic and depressive episodes — and monopolar or unipolar disorders, marked by depressive episodes alone without mania. Splitting Kraepelin’s single “manic-depressive” group along this axis was a conceptual turning point: it made the presence of mania, not merely the recurrence of mood episodes, the defining feature of one branch of illness.
Through the 1960s and 1970s, researchers in Europe and the United States accumulated evidence that bipolar and unipolar depression differed in important ways — in family history, in typical age of onset, and in response to treatment — which gave the bipolar/unipolar split clinical teeth and prepared the ground for its adoption into formal classification. Over later decades the picture broadened further into the idea of a bipolar spectrum, distinguishing, for example, bipolar I (with full manic episodes) from bipolar II (with hypomania and depression), and recognising milder and mixed presentations. These finer subdivisions belong to the later twentieth and twenty-first centuries and continue to be refined.
John Cade, Lithium, and the Birth of Psychopharmacology
Running alongside the story of naming the illness is the story of treating it — and here the landmark is lithium. The Australian psychiatrist John Cade (1912–1980), working in modest conditions at a repatriation hospital in Victoria after returning from years as a prisoner of war, suspected that mania might be caused by some circulating chemical in the body. While investigating this idea in animal experiments, he used lithium salts to dissolve a compound and noticed that the lithium itself made the animals calm and placid. He then cautiously tried lithium in patients with mania and observed striking improvement. Cade published these findings in the Medical Journal of Australia in 1949, in a paper titled “Lithium salts in the treatment of psychotic excitement” (the underlying observations date to the late 1940s; the formal report appeared in 1949).
Cade’s discovery is rightly remembered as one of the founding events of modern psychopharmacology — arguably the first time a simple chemical was shown to target a specific severe mental illness — yet it nearly vanished. It was published in a then-obscure journal, lithium carried real toxicity risks that frightened clinicians (lithium chloride had caused poisonings when used as a salt substitute), and the finding was slow to spread beyond Australia. Its rescue and rigorous validation are largely owed to the Danish psychiatrist Mogens Schou (1918–2005), who, with colleagues, ran controlled studies confirming lithium’s antimanic effect and — most importantly — demonstrated that ongoing lithium could serve as prophylaxis, reducing the recurrence of future mood episodes. That shift, from quieting an acute attack to preventing the next one, transformed lithium from a curiosity into a cornerstone of long-term care.
For readers today, two honest points deserve emphasis. First, lithium is a genuine medical treatment requiring blood-level monitoring and clinical supervision; this page is history, not medical advice, and treatment decisions belong with a qualified clinician. Second, the lithium story is a reminder that effective psychiatric treatments can emerge from careful observation and be confirmed only through controlled research — the same disciplined progression from hypothesis to evidence that runs through the entire history of this illness.
Naming the Illness: From DSM-III to Today
The word patients and clinicians use today is relatively new. The American Psychiatric Association’s third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III, 1980) replaced the older label “manic-depressive illness” with bipolar disorder, formally importing Leonhard’s bipolar framing into mainstream diagnosis. Part of the motivation was to move away from a term widely felt to be stigmatising and easily confused, in everyday speech, with words like “maniac.” DSM-III is also remembered for shifting psychiatric diagnosis toward explicit, listed criteria, which made conditions like bipolar disorder easier to identify consistently across clinicians.
Since 1980 the diagnosis has continued to be refined. Later editions formalised the separation of bipolar I (defined by at least one full manic episode) from bipolar II (defined by hypomania together with major depression), and recognised related and milder presentations such as cyclothymia. The broad outline, however, traces directly back through Leonhard to Kraepelin to the French clinicians of the 1850s — and, in spirit, to the ancient intuition of Aretaeus that mania and melancholia belong to one story.
Language, Stigma, and What the History Teaches
The evolution of the name — from circular insanity, to manic-depressive insanity, to manic-depressive illness, to bipolar disorder — is itself a history of changing attitudes. Each renaming reflected an effort to describe the condition more accurately and, increasingly, more humanely. The 1980 move to “bipolar disorder” was driven partly by a wish to reduce the stigma attached to older language, and the same impulse continues today in person-first phrasing such as “a person living with bipolar disorder.” Words shape how people who live with this condition are seen and treated, which is why precision and compassion in language are not cosmetic.
The history also offers a quiet corrective to two opposite errors. It cautions against over-claiming — reading the full modern diagnosis into every ancient or famous historical figure, when the honest record supports only an intuition in antiquity and a defined illness from the nineteenth century onward. And it cautions against dismissing the condition as a modern invention — because the core observation, that one person can swing between mania and depression, has been independently noticed by careful clinicians across two thousand years and three continents. That convergence is exactly what one expects of a real biological illness, and it is the most reassuring thing the long history of bipolar disorder has to teach.
Finally, the arc from Aretaeus’s humoral speculation to Cade and Schou’s evidence-based lithium prophylaxis is a model of how medicine should work: an old observation is taken seriously, tested against careful clinical follow-up, sharpened into a precise diagnosis, and matched at last with a treatment proven in controlled research. For anyone affected by bipolar disorder, knowing that this scaffolding exists — built patiently over centuries — can make a frightening diagnosis feel less like a mystery and more like a well-mapped, treatable part of human health.
Research Papers and References
The references below combine peer-reviewed historical scholarship on bipolar disorder with curated PubMed topic-search links into the primary literature. Classic primary works are named in the article as historical sources rather than as modern citations: Aretaeus of Cappadocia’s clinical writings (1st–2nd century CE); Falret’s folie circulaire (1851) and Baillarger’s folie à double forme (1854); Kraepelin’s Psychiatrie, 6th edition (1899); Leonhard’s monograph on the classification of the endogenous psychoses (1957); and Cade’s original lithium report in the Medical Journal of Australia (1949). Each link opens at its source in a new tab.
- Angst J, Marneros A. Bipolarity from ancient to modern times: conception, birth and rebirth. Journal of Affective Disorders. 2001;67(1–3):3–19. — doi:10.1016/S0165-0327(01)00429-3
- Marneros A. The birth of the bipolar disorder. European Psychiatry. 2009;24(3):200–202. — PubMed: PMID 19698309
- Sedler MJ. Falret’s discovery: the origin of the concept of bipolar affective illness. American Journal of Psychiatry. 1983;140(9):1127–1133. — doi:10.1176/ajp.140.9.1127
- Pichot P. Tracing the origins of bipolar disorder: from Falret to DSM-IV and ICD-10. Journal of Affective Disorders. 2006;96(3):145–148. — doi:10.1016/j.jad.2006.08.013
- Haustgen T, Akiskal H. French antecedents of “contemporary” concepts in the American Psychiatric Association’s classification of bipolar (mood) disorders. Journal of Affective Disorders. 2006;96(3):149–163. — doi:10.1016/j.jad.2006.08.029
- Ban TA. Pharmacotherapy of mental illness — a historical analysis. Progress in Neuro-Psychopharmacology & Biological Psychiatry. 2001;25(4):709–727. — doi:10.1016/S0278-5846(01)00160-9
- Cade JFJ. Lithium salts in the treatment of psychotic excitement. Medical Journal of Australia. 1949;2(10):349–352. (Reprinted: Bulletin of the World Health Organization. 2000;78(4):518–520.) — PMC reprint: PMC2560740
- Mitchell PB, Hadzi-Pavlovic D. John Cade and the discovery of lithium treatment for manic depressive illness. Medical Journal of Australia. 1999;171(5):262–264. — PubMed: PMID 10495760
- Shorter E. The history of lithium therapy. Bipolar Disorders. 2009;11(Suppl 2):4–9. — doi:10.1111/j.1399-5618.2009.00706.x
- Schou M. Lithium treatment at 52. Journal of Affective Disorders. 2001;67(1–3):21–32. — doi:10.1016/S0165-0327(01)00380-9
- Kraepelin’s dichotomy and the classification of mood and psychotic disorders (historical reviews) — PubMed: Kraepelin manic-depressive insanity history
- Karl Leonhard and the bipolar–unipolar (monopolar) distinction — PubMed: Leonhard bipolar unipolar classification
- Aretaeus of Cappadocia on mania and melancholia (history of psychiatry) — PubMed: Aretaeus mania and melancholia
- History and evolution of bipolar disorder diagnostic criteria (DSM) — PubMed: bipolar disorder history and diagnostic criteria
External Authoritative Resources
- NIMH — Bipolar Disorder (National Institute of Mental Health)
- History of Bipolar Disorder — overview with primary-source citations
- PubMed — All research on the history of bipolar disorder