Tendinitis: History and Discovery
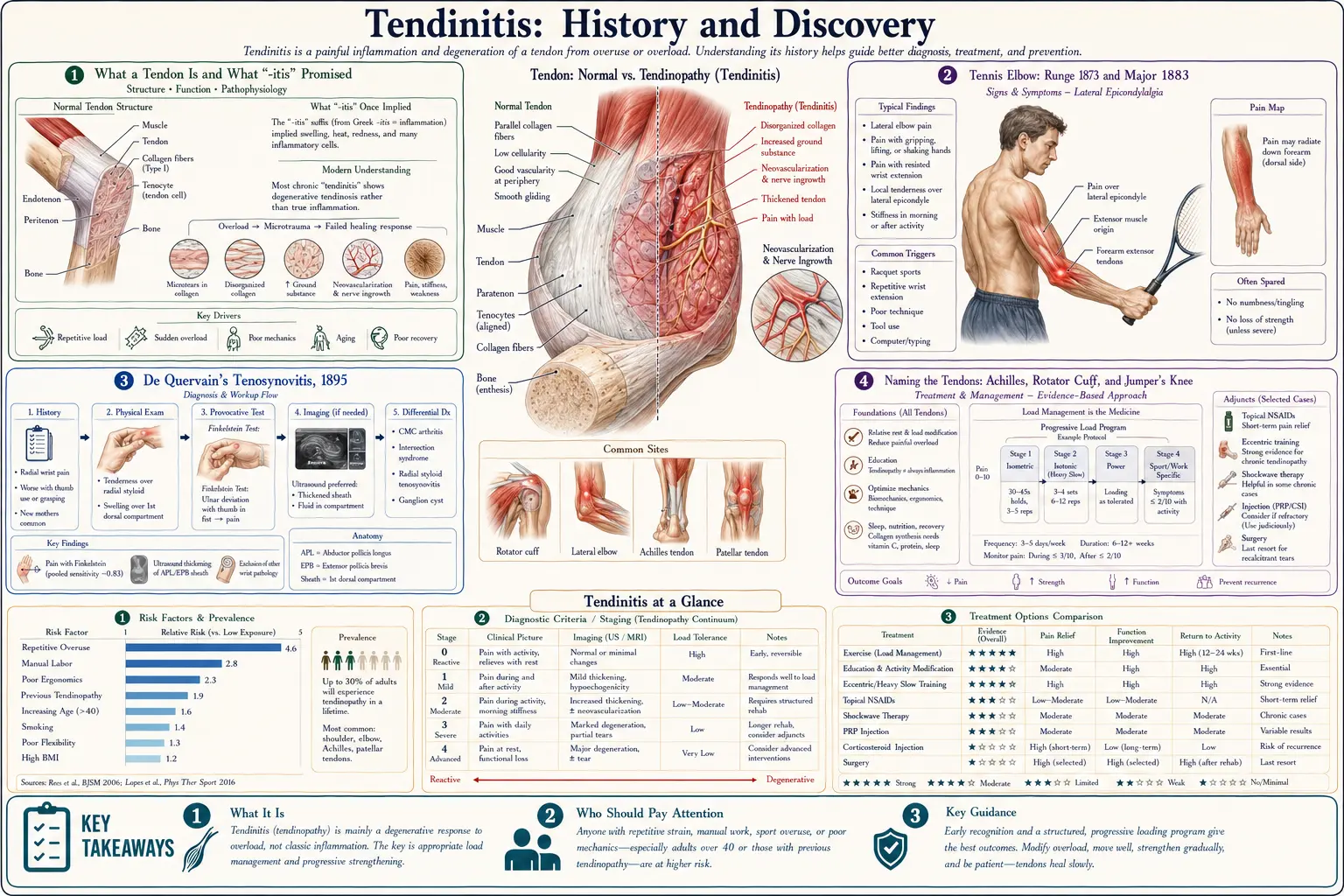
Tendinitis (also spelled tendonitis) means pain and injury of a tendon — the tough cord of collagen that anchors muscle to bone — most often from repeated overuse rather than a single injury. The name itself tells a story: the suffix “-itis” means inflammation, and for most of the twentieth century doctors assumed that an overused tendon was simply an inflamed one. But when researchers in the late twentieth century finally looked at chronically painful tendons under the microscope, they kept finding something unexpected — not the inflammatory cells they expected, but disorganized, degenerating collagen. That discovery rewrote the vocabulary of tendon medicine, replacing “tendinitis” with tendinosis (degeneration) and the broader umbrella term tendinopathy. This page traces that journey: from the first descriptions of “tennis elbow” in the 1870s and 1880s, through the named tendon disorders of the rotator cuff, the Achilles, and the knee, to the modern reckoning with what tendon pain actually is — and how that changed the way it is treated.
Table of Contents
- What a Tendon Is and What “-itis” Promised
- Tennis Elbow: Runge 1873 and Major 1883
- De Quervain’s Tenosynovitis, 1895
- Naming the Tendons: Achilles, Rotator Cuff, and Jumper’s Knee
- The Question That Broke the Word “Tendinitis”
- The Terminology Shift: Tendinitis → Tendinosis → Tendinopathy
- Overuse, Mechanical Load, and Why Rest Is Not Enough
- The Eccentric-Exercise Revolution in Treatment
- Legacy: An Old Word, a New Understanding
- Research Papers and References
- Connections
- Featured Videos
What a Tendon Is and What “-itis” Promised
A tendon is the dense, glistening band of connective tissue that transmits the pull of a muscle to a bone, allowing a contraction in the calf to lift the heel or a contraction in the forearm to grip a racket. Tendons are built almost entirely of type-I collagen, laid down in tight, parallel, rope-like bundles that give them enormous tensile strength but relatively little blood supply. That sparse blood flow, prized for efficiency, turns out to be a liability: it makes tendons slow to heal and, as later researchers would learn, prone to a quiet, gradual breakdown rather than the dramatic red-and-swollen reaction of more vascular tissues.
For most of medical history, the language used to describe a painful tendon followed a simple and intuitive rule. In medicine the suffix “-itis” denotes inflammation — appendicitis, arthritis, bronchitis — so a sore tendon was naturally called tendinitis (or tendonitis), and a sore tendon-sheath tenosynovitis or tendovaginitis. The word carried an embedded assumption: that the pain came from inflammation, that inflammatory cells were present, and that anti-inflammatory treatment — rest, ice, and later cortisone injections and anti-inflammatory drugs — was the logical cure.
That assumption was reasonable, widely held, and, for chronic overuse tendons, largely wrong. Unpicking it took roughly a century of clinical observation and, crucially, the willingness to put diseased tendon tissue under a microscope and report honestly what was — and was not — there. The story of tendinitis is therefore as much a story about a word as about a disease.
Tennis Elbow: Runge 1873 and Major 1883
The first tendon-overuse condition to be carefully described in the medical literature was the one we now call tennis elbow, or lateral epicondylitis — pain at the bony bump on the outer elbow where the forearm extensor tendons attach. The German physician F. Runge is generally credited with the first clinical description in 1873. Notably, Runge did not connect it to tennis at all; he described it in the context of writing and manual work and used terms rendered as “writer’s cramp” (Schreibekrampf), and the condition was also popularly known as “washerwoman’s elbow.” The link to sport came a decade later.
In 1882, the British surgeon Henry Morris published a note in The Lancet describing “the lawn tennis arm,” an aching forearm and elbow he attributed to the repeated back-stroke of the then-fashionable game of lawn tennis. The following year, 1883, H. P. Major coined the now-familiar phrase “lawn-tennis elbow,” which the medical world soon shortened to “tennis elbow.” The eponymous timeline — Runge’s 1873 description, Morris’s 1882 “lawn tennis arm,” and Major’s 1883 “lawn-tennis elbow” — is documented in historical reviews of the condition and is reasonably well established, though, as with many nineteenth-century eponyms, individual dates occasionally vary by a year between sources.
The irony embedded in the name endures. Then as now, only a small minority of tennis-elbow sufferers play tennis; the condition arises from any repetitive gripping and wrist-extending activity — plumbing, painting, carpentry, typing, butchery. The name “tennis elbow” is thus a historical accident of late-Victorian leisure, and the alternative formal name, “lateral epicondylitis,” carries the same misleading “-itis” that later research would call into question.
De Quervain’s Tenosynovitis, 1895
A second landmark in the early history of tendon disorders came in 1895, when the Swiss surgeon Fritz de Quervain (1868–1940), working in La Chaux-de-Fonds, published a short series of cases — five patients in the original report — describing a tender, thickened swelling on the thumb side of the wrist that made thumb and wrist movement painful. He titled the paper, in German, on a form of chronic tendovaginitis (tendon-sheath disease), and the condition has carried his name ever since as De Quervain’s tenosynovitis.
What de Quervain described is, in modern terms, a stenosing (narrowing) condition of the first dorsal compartment of the wrist — the fibrous tunnel through which the tendons of two thumb muscles, the abductor pollicis longus and extensor pollicis brevis, glide. The sheath and its overlying retinaculum thicken, the tunnel narrows, and the tendons no longer slide freely, producing pain on gripping and lifting. It is classically associated with repetitive thumb and wrist use, and in the modern era is sometimes nicknamed “mother’s wrist” or “texting thumb” for its links to lifting infants and to handheld devices.
De Quervain’s contribution matters to this history for two reasons. First, it was an early, precise, anatomically grounded description of a tendon-sheath disorder, by a surgeon prominent enough that the eponym stuck across languages. Second, like tennis elbow, it was named within the inflammatory “-itis” (and “-vaginitis”) framework — yet modern study of de Quervain’s tissue typically shows thickening and degenerative change of the sheath rather than the acute inflammation the name implies, foreshadowing the larger reckoning to come.
Naming the Tendons: Achilles, Rotator Cuff, and Jumper’s Knee
Tendon problems cluster at a handful of high-load sites, and each of the most important has its own naming history. The Achilles tendon — the great heel cord and the largest, strongest tendon in the body — takes its name from the Greek hero whose heel was his one vulnerable point. The oldest surviving record of the anatomical name belongs to the Flemish anatomist Philip Verheyen, who in 1693, in his widely used text Corporis Humani Anatomia, described the structure and noted that it was commonly called “the cord of Achilles.” Achilles tendinopathy — pain in the mid-portion or insertion of that cord — would much later become one of the most-studied of all overuse tendon conditions.
At the shoulder, the four-tendon sleeve now called the rotator cuff has its own lineage. An early description of a torn shoulder tendon is credited to J. G. Smith, who reported tendon rupture after shoulder injury in the London Medical Gazette in 1834. The defining modern work, however, is Boston surgeon Ernest Amory Codman’s 1934 monograph, often referenced for its long subtitle about “rupture of the supraspinatus tendon and other lesions in or about the subacromial bursa,” which summarized decades of his observations and made the supraspinatus tendon a focus of shoulder medicine.
At the knee, the term “jumper’s knee” for pain at the patellar (kneecap) tendon was coined by Blazina and colleagues in 1973, who described it in skeletally mature athletes and proposed a staging system — based on whether pain came after activity, during and after activity, or constantly — that clinicians still cite. Together, these named conditions — tennis elbow, de Quervain’s, Achilles, rotator cuff, and jumper’s knee — formed the clinical map of tendon overuse. What they shared, and what would soon unite them under a new word, was a growing suspicion that the inflammatory model did not fit what surgeons were actually seeing inside the tissue.
The Question That Broke the Word “Tendinitis”
By the second half of the twentieth century, surgeons operating on chronically painful tendons — opening an Achilles, a patellar tendon, or a tennis-elbow extensor origin that had failed months of rest and anti-inflammatory treatment — began to notice a consistent mismatch. The tissue they found was not the angry, swollen, inflamed material the diagnosis of “tendinitis” predicted. Instead it was dull, gray-brown, soft, and disorganized: collagen that had lost its tight parallel order, with abnormal new blood-vessel and nerve ingrowth and an absence of the acute inflammatory cells (neutrophils and the like) that define true inflammation.
When pathologists examined these specimens under the microscope, they confirmed the surgeons’ impression. The dominant findings in chronic overuse tendons were degenerative — collagen disarray, increased ground substance, microscopic tearing, and neovascularization — not inflammatory. The German-speaking literature had in fact used the term tendinosis (the “-osis” suffix denoting a degenerative, non-inflammatory process) as early as the 1940s, and Italian and other European investigators through the 1970s, including work associated with Perugia and later Puddu, sharpened the focus on this histology and on the term tendinosis itself.
This was more than a semantic quibble. If chronic tendon pain was driven by degeneration rather than inflammation, then the entire anti-inflammatory therapeutic strategy — the cortisone injections, the long courses of anti-inflammatory drugs, the prolonged rest — was aimed at a target that, in most chronic cases, was not actually there. The word “tendinitis” was not merely inaccurate; it was actively steering treatment in an unhelpful direction.
The Terminology Shift: Tendinitis → Tendinosis → Tendinopathy
The decisive correction came in the late 1990s. In 1998, a group of clinician-researchers — notably Nicola Maffulli, Karim Khan, and Giancarlo Puddu — published an influential argument, with the pointed title “Overuse tendon conditions: time to change a confusing terminology.” Their case was straightforward: the clinical label should reflect the underlying tissue. Reserve tendinitis for the genuinely inflammatory minority of cases; use tendinosis for the far more common degenerative tissue diagnosis confirmed by histology; and, because clinicians usually cannot know the histology of a living patient’s painful tendon without a biopsy, adopt the neutral umbrella term tendinopathy for the clinical syndrome of a painful, often swollen, impaired tendon, whatever the precise tissue picture.
The reframing settled the field’s vocabulary. Tendinopathy became the preferred clinical umbrella term, with tendinosis denoting the degenerative tissue diagnosis and tendinitis retained only where true inflammation is present (most often in acute injury or around a frank rupture). It is now widely accepted that in chronic overuse conditions in and around tendons, frank inflammation is the exception rather than the rule. The older “-itis” names — tennis elbow as “lateral epicondylitis,” Achilles “tendinitis,” patellar “tendinitis” — persist in everyday speech and in many patient-facing materials, but the specialist literature increasingly speaks of epicondylalgia or epicondylosis, and of Achilles and patellar tendinopathy.
It is worth being honest about nuance here: the pendulum has not stopped swinging. More recent molecular research suggests that inflammatory signaling and immune-cell activity may play some role in tendinopathy after all, particularly in its early stages — so the strict “degeneration, never inflammation” position is itself now treated as an oversimplification, and is best described as an evolving hypothesis rather than a closed case. What remains firmly established is the core 1990s insight that classical acute inflammation does not dominate the chronic overuse tendon, and that “tendinitis” alone is a misleading name for it.
Overuse, Mechanical Load, and Why Rest Is Not Enough
If chronic tendon pain is not primarily an inflammatory fire to be doused, what drives it? The unifying answer that emerged is mechanical load — specifically, repetitive loading that outpaces the tendon’s capacity to adapt and repair. Tendons are living, responsive tissues: appropriate load makes them stronger, but load applied too often, too suddenly, or without enough recovery accumulates microscopic damage faster than the slow-healing collagen can rebuild it. The result is the disorganized, degenerative tissue described above — tendinosis — and the clinical syndrome of tendinopathy.
This load-centered model reframes who gets tendon trouble and why. It is not just elite athletes; it is anyone whose tendons are loaded repetitively beyond their adaptation — runners and jumpers (Achilles, patellar), throwers and overhead workers (rotator cuff), and people who grip and twist for a living (tennis elbow, de Quervain’s). Contributing factors layer on top of load: increasing age (collagen turns over more slowly and tendons stiffen), certain metabolic conditions, and some medications — the fluoroquinolone antibiotics, for instance, are recognized to raise the risk of tendon pain and even rupture, especially of the Achilles.
The load model also explains the limits of rest. Complete rest may calm an acutely irritable tendon, but because the underlying problem is failed collagen adaptation rather than inflammation, prolonged unloading allows the tendon to weaken further and does not rebuild its disorganized structure. Tendons appear to need some load to remodel and recover — which set the stage for the most important treatment discovery in the modern history of tendinopathy: that carefully applied exercise, not rest, is often the cure.
The Eccentric-Exercise Revolution in Treatment
Once tendinopathy was understood as a problem of load and degeneration rather than inflammation, the logical treatment was not to remove load but to apply it in a controlled, graded, therapeutic way. The roots of this idea reach back to Curwin and Stanish in 1984, who proposed an exercise program emphasizing eccentric contractions — muscle lengthening under tension, as when the calf slowly lowers the heel rather than pushing it up — for tendon rehabilitation, paired with stretching.
The landmark demonstration came in 1998, when the Swedish physician Håkan Alfredson and colleagues at the University of Umeå published a now-famous study of heavy-load eccentric calf training for chronic Achilles tendinosis. Patients performed a structured program of painful eccentric heel-drops — on the order of 180 repetitions a day, divided into sets, performed daily over twelve weeks — and a striking proportion improved enough to return to activity and avoid the surgery they had been waiting for. The “Alfredson protocol” became one of the most widely adopted and studied interventions in all of sports medicine, and confirmed in practice what the histology had implied: a degenerating tendon responds to loading, not unloading.
Later research has refined rather than overturned this picture. Heavy-slow-resistance training (using both the lowering and lifting phases under heavy load) has shown comparable benefit to pure eccentric work for several tendinopathies and is often easier for patients to sustain, and progressive, individualized loading programs are now the backbone of conservative care. The broader lesson of the eccentric-exercise era is the practical payoff of the terminology shift: changing the name from “tendinitis” to “tendinopathy” changed the question from “how do we reduce inflammation?” to “how do we rebuild a degenerated, load-sensitive tendon?” — and the answer, for many patients, turned out to be patient, graded exercise rather than rest and injections.
Legacy: An Old Word, a New Understanding
The history of tendinitis is unusual in medicine because its central event is the partial retirement of its own name. The conditions are ancient and the early descriptions vivid — Runge’s writer’s cramp, Morris’s and Major’s lawn-tennis arm and elbow, de Quervain’s thickened wrist, Codman’s torn shoulder, Blazina’s jumper’s knee — but the deepest insight came not from discovering a new disease, but from looking honestly at a familiar one and admitting that its long-assumed mechanism was, in most chronic cases, mistaken.
That insight reshaped both language and practice. The umbrella term tendinopathy, the tissue diagnosis tendinosis, and the narrowed, accurate use of tendinitis now structure how clinicians think; and the move away from rest-and-anti-inflammation toward progressive, load-based rehabilitation reflects the same change in understanding. For the millions of people who develop tendon pain at the elbow, heel, shoulder, knee, or thumb, this history is not academic: it is the reason a modern clinician is more likely to prescribe a graded exercise program than a cortisone shot and indefinite rest.
The word “tendinitis” survives in everyday speech, and this site — like most patient-facing resources — keeps it as the familiar entry point. But the better, truer picture behind it is that an overused tendon is usually not on fire; it is worn, disordered, and waiting to be carefully rebuilt. Knowing that difference is the single most useful thing the long history of tendon medicine has to teach.
Research Papers and References
The list below combines key peer-reviewed papers on tendon terminology, histopathology, eponymous history, and treatment with curated PubMed topic-search links. Historical primary sources (Runge’s 1873 description, Morris’s 1882 and Major’s 1883 Lancet notes, de Quervain’s 1895 paper, Verheyen’s 1693 anatomy, and Codman’s 1934 monograph) are named in the article as historical sources. Each link opens in a new tab.
- Maffulli N, Khan KM, Puddu G. Overuse tendon conditions: time to change a confusing terminology. Arthroscopy. 1998;14(8):840-843. — PubMed 9848596
- Khan KM, Cook JL, Kannus P, Maffulli N, Bonar SF. Time to abandon the “tendinitis” myth. BMJ. 2002;324(7338):626-627. — doi:10.1136/bmj.324.7338.626
- Scott A, Squier K, Alfredson H, et al. ICON 2019: International Scientific Tendinopathy Symposium Consensus — terminology for tendon pathology. Br J Sports Med. 2020;54(5):260-262. — doi:10.1136/bjsports-2019-100885
- Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J Sports Med. 2009;43(6):409-416. — doi:10.1136/bjsm.2008.051193
- Alfredson H, Pietilä T, Jonsson P, Lorentzon R. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med. 1998;26(3):360-366. — doi:10.1177/03635465980260030301
- de Quervain F. On a form of chronic tendovaginitis (1895; reprinted/translated). — PubMed 9316729
- Ahuja V, Thapa D, Patial S, et al. (and related historical reviews) Tennis elbow: a clinical review article. J Clin Orthop Trauma. 2020. — PMC6926298
- Rees JD, Stride M, Scott A. Tendons — time to revisit inflammation. Br J Sports Med. 2014;48(21):1553-1557. — doi:10.1136/bjsports-2012-091957
- Beyer R, Kongsgaard M, Hougs Kjaer B, et al. Heavy slow resistance versus eccentric training for patellar tendinopathy: a randomized controlled trial. Am J Sports Med. 2015;43(7):1704-1711. — doi:10.1177/0363546515584760
- History and early description of tennis elbow (Runge 1873; Morris 1882; Major 1883) — PubMed: tennis elbow history
- Jumper’s knee / patellar tendinopathy — description and staging (Blazina 1973) — PubMed: jumper’s knee Blazina
- Rotator cuff — historical landmarks (Codman 1934; Smith 1834) — PubMed: rotator cuff history
- Eccentric exercise for tendinopathy — origins and evidence (Curwin & Stanish 1984; Alfredson 1998) — PubMed: eccentric exercise tendinopathy
- De Quervain’s tenosynovitis — history and pathology — PubMed: de Quervain tenosynovitis history
External Authoritative Resources
- StatPearls (NCBI Bookshelf) — Tendinosis
- MedlinePlus — Tendinitis
- PubMed — All research on tendinopathy terminology