Glaucoma: History and Discovery
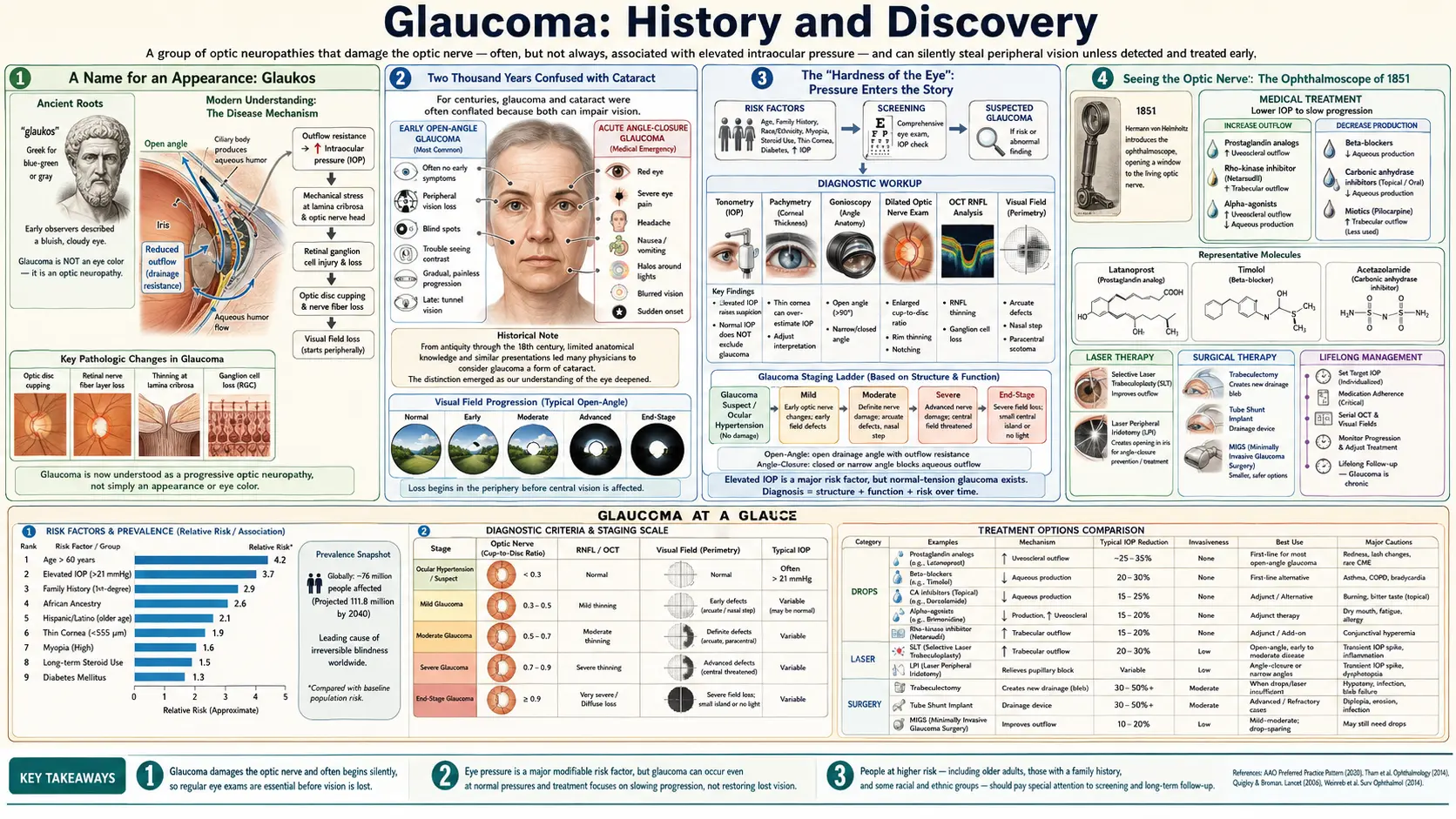
The word glaucoma descends from the ancient Greek glaukos — gleaming, blue-green, or grey — a Hippocratic-era label that lumped together various causes of blindness in the elderly and was long confused with cataract. For more than two thousand years the term named an appearance, not a mechanism. Only slowly did the picture sharpen: by the seventeenth and eighteenth centuries the eye's "hardness," or elevated internal pressure, began to be tied to the disease; the invention of the ophthalmoscope by Hermann von Helmholtz in 1851 let physicians actually see the cupped optic nerve; Albrecht von Graefe of Berlin introduced iridectomy as a surgical treatment for acute glaucoma in 1857; and Hjalmar Schiøtz made the bedside measurement of eye pressure practical with his impression tonometer in 1905. Today glaucoma is understood not as a pressure reading but as an optic neuropathy — a progressive loss of nerve fibres at the back of the eye, often but not always accompanied by raised pressure.
Table of Contents
- A Name for an Appearance: Glaukos
- Two Thousand Years Confused with Cataract
- The "Hardness of the Eye": Pressure Enters the Story
- Seeing the Optic Nerve: The Ophthalmoscope of 1851
- Von Graefe and the Iridectomy of 1857
- Measuring the Pressure: Schiøtz and Tonometry
- Drops and Drainage: A Century of Treatment
- The Modern Idea: Glaucoma as an Optic Neuropathy
- Research Papers and References
- Connections
- Featured Videos
A Name for an Appearance: Glaukos
The history of glaucoma begins not with a disease but with a colour word. The Greek adjective glaukos (γλαυκóς) was a famously imprecise term that could mean gleaming, silvery, pale, grey, or blue-green — Homer applied it to the sea and to the eyes of the goddess Athena. When the Hippocratic writers (working in the era of Hippocrates, roughly 460–370 BCE) turned it to medicine, glaukosis described an eye whose pupil had taken on a dull, gleaming, sea-grey or greenish cast — a sign, they observed, that often appeared in the elderly and heralded the loss of sight.
It is important to be honest about what this ancient term did and did not mean. Glaukos named an appearance, the altered colour of the pupil, and not any underlying cause. The Hippocratic authors had no concept of intraocular pressure, no way to examine the inside of the living eye, and no notion that the optic nerve could waste away. To them, as the historian Christopher Leffler and colleagues document, "glaucoma" was simply one of several words attached to an old person going blind with a discoloured pupil. The name has endured for two and a half millennia, but the idea behind it has been almost completely rebuilt.
Even within antiquity the term was contested. Later Greek physicians in the Hippocratic tradition often preferred hypochysis or hypochyma — literally an "outpouring" or "underflowing" of fluid behind the pupil — for the same blinding condition, a sign that glaukoma never quite satisfied a rigorous medical definition. From its very origin, then, the word was a loose, observational label awaiting a mechanism that medicine would not supply for another two thousand years.
Two Thousand Years Confused with Cataract
The single greatest source of confusion in the long history of glaucoma is that, for most of it, glaucoma and cataract were not reliably told apart. The reason is simple and visual: a mature white cataract turns the pupil pale or grey, and so does an eye in acute angle-closure glaucoma, which can show a hazy green-grey pupil. To an examiner without instruments, peering at an undilated pupil by daylight, the two could look much the same — and a dense white cataract, visible without any dilation, was by far the commoner cause of a discoloured pupil. Many an eye the ancients called glaukos was almost certainly cataract.
The disentangling came astonishingly late. Across the medieval Islamic and European traditions the terms drifted and overlapped, and conditions causing blindness with a normal-looking eye — which is how chronic open-angle glaucoma typically presents — were filed under still other names such as amaurosis, gutta serena, or "black cataract." According to the etymological record, cataract and glaucoma were not clearly distinguished in the medical literature until around 1705, when the older sense of glaucoma began to be separated from the lens opacity we now call cataract. Only after surgeons learned, in the eighteenth century, that cataract was a clouding of the lens — couched or later extracted — could the leftover cases of blindness-with-pressure be recognised as a distinct disease.
This tangled nomenclature is why historians caution against reading modern glaucoma back into ancient texts too confidently. When a classical or medieval author wrote glaukoma, he may have meant cataract, may have meant glaucoma, and may have meant something else entirely. The Leffler review, aptly titled What was Glaucoma Called Before the 20th Century?, traces exactly this migration of names and is the careful modern guide to which old word meant which modern disease.
The "Hardness of the Eye": Pressure Enters the Story
The decisive conceptual shift — from glaucoma as a colour to glaucoma as a pressure — began in the seventeenth century with a clinical observation that anyone can still make today by gently pressing a fingertip to a closed eyelid: some blind eyes feel abnormally hard. The English oculist Richard Banister, in an appendix he added in 1622 to an English edition of Jacques Guillemeau's treatise on diseases of the eye, recorded that in certain incurable cases "the Eye be grown more solid and hard, then naturally it should be." Banister is generally credited as the first writer to link a palpably hardened eye to this category of untreatable blindness — the first faint outline of the idea of raised intraocular pressure.
It is worth stressing how tentative this was, and labelling it honestly as the period's working hypothesis rather than settled science. Banister had no instrument to measure pressure and no theory of where it came from; he had only a finger and a careful eye. Through the eighteenth century other surgeons and oculists repeated and refined the observation that hardness accompanied certain blinding eyes, and the suspicion grew that an internal tension might be doing the damage. But cause and effect remained unproven: physicians could feel that some blind eyes were hard, yet they could not say whether the hardness caused the blindness, resulted from it, or merely accompanied it.
Even so, Banister's note marks a genuine turning point. For the first time the disease was being defined by something happening inside the eye — a physical state of the globe — rather than by the shade of the pupil seen from outside. Over the following two centuries this thread of "the hard eye" would be pulled steadily forward, until elevated intraocular pressure stood at the centre of the entire concept of glaucoma. The historian F. Krogmann's survey, pointedly titled 2000 Years Under Pressure, takes this slow ascent of the pressure idea as the organising theme of glaucoma's whole history.
Seeing the Optic Nerve: The Ophthalmoscope of 1851
For all of recorded history before the mid-nineteenth century, the interior of the living eye was a sealed black box. Physicians could inspect the cornea, the iris, and the surface of a cataract, but the retina and the optic nerve — where glaucoma actually does its damage — lay beyond reach behind a dark pupil. That barrier fell in 1851, when the German physicist and physiologist Hermann von Helmholtz invented the ophthalmoscope. His device, which he called an Augenspiegel ("eye mirror"), used a perforated mirror to throw light into the eye and let the observer look back along the same path to the illuminated retina; the term "ophthalmoscope" itself came into general use about three years later, in 1854.
The consequences for glaucoma were immediate and profound. With Helmholtz's instrument, observers could at last see the optic disc — the head of the optic nerve — in the living eye, and in glaucomatous eyes they found it abnormally hollowed, or cupped, as if the centre had been pressed inward. The anatomist and physiologist Heinrich Müller is credited with describing and naming this glaucomatous "cupping" of the optic disc in 1856. Müller offered the natural interpretation of the day: that raised pressure inside the eye was physically pushing the nerve head backward, excavating the cup. This pressure-pushes-the-cup explanation should be read as the leading nineteenth-century hypothesis; it captured a real and reproducible finding, and pointed in the right direction, but the full story of how pressure injures the nerve would prove far more subtle.
What mattered was that glaucoma now had a visible, internal lesion. The discolored pupil of the Greeks had given way, in a single generation, to a structure a physician could actually examine and follow over time: the cupped optic nerve. The ophthalmoscope turned glaucoma from a guess about appearances into a disease with anatomy — and it set the stage for the surgery that would arrive only a year after Müller named the cup.
Von Graefe and the Iridectomy of 1857
The towering clinical figure in nineteenth-century glaucoma is Albrecht von Graefe (1828–1870), who worked at the University of Berlin and is widely regarded as a founder of modern scientific ophthalmology. Von Graefe seized on Helmholtz's new ophthalmoscope, used it to study glaucomatous cupping, produced an early classification of the disease, and pioneered the measurement of the visual field to map the creeping loss of sight that glaucoma causes. His central contribution to treatment came in 1857, when he introduced iridectomy — the surgical removal of a small wedge of iris — as a treatment for glaucoma, most dramatically for the agonising, sight-threatening attacks of what we now call acute angle-closure glaucoma.
The result, in those acute cases, could be near-miraculous for the era. An eye in acute angle-closure glaucoma is rock-hard, blindingly painful, and racing toward permanent blindness within days; von Graefe's iridectomy could break such an attack, relieve the pain, soften the eye, and save vision — the first reliably effective operation in the long history of the disease. In light of the modern understanding of angle-closure, the reason iridectomy works is clear: removing a piece of iris reopens or bypasses the blocked drainage angle and lets the trapped fluid escape, dropping the pressure. Von Graefe achieved his cures empirically, by bold and careful observation, well before that drainage mechanism was fully worked out.
Honesty requires a clear boundary here, because patients read these pages. Iridectomy was a genuine breakthrough for acute angle-closure glaucoma, and a form of it (and the gentler modern laser iridotomy) remains a standard, sight-saving intervention for angle-closure today. It was not a cure for the commoner, silent, chronic open-angle glaucoma, in which the drainage angle is not anatomically shut, and von Graefe's own results in those cases were far less consistent. Still, his work transformed the field: he founded the world's first ophthalmological society and a long-lived ophthalmology journal, and his name endures in instruments and signs taught to eye surgeons to this day.
Measuring the Pressure: Schiøtz and Tonometry
Once raised pressure stood at the centre of the glaucoma concept, an obvious problem remained: how to measure it. Estimating eye pressure by pressing with the fingertips — digital tonometry — is crude and wildly observer-dependent; two examiners feeling the same eye routinely disagreed. Nineteenth-century physicians, including von Graefe, experimented with mechanical instruments to read the pressure objectively, but none was simple, portable, and trustworthy enough for everyday clinical use. Measuring the very quantity that defined the disease remained frustratingly out of reach.
The breakthrough came in 1905, when the Norwegian ophthalmologist Hjalmar Schiøtz (1850–1927) introduced his impression (indentation) tonometer. Schiøtz's device was elegantly simple: rested on the anaesthetised cornea of a reclining patient, a small plunger of known weight pressed in, and the depth to which it indented the eye — read off a calibrated scale and converted by a table — gave the intraocular pressure in millimetres of mercury. A softer eye let the plunger sink further; a hard, high-pressure eye resisted it. For the first time, eye pressure could be put on a number that different clinicians, in different places, could compare.
The Schiøtz tonometer was rugged, inexpensive, and accurate enough to become the world's standard for measuring intraocular pressure for more than half a century, and it made population screening for raised pressure conceivable. It was eventually superseded for routine clinical work by the applanation tonometer developed by Hans Goldmann in the mid-twentieth century — which measures the force needed to flatten a small, fixed area of cornea and remains the clinical reference standard — and today by non-contact "air-puff" and rebound devices. But Schiøtz's 1905 instrument was the hinge on which glaucoma care turned from impression into measurement.
Drops and Drainage: A Century of Treatment
While surgeons advanced operations and instrument-makers refined tonometers, a parallel history unfolded in the pharmacy. The medical (drop) treatment of glaucoma is conventionally dated to 1862, when the alkaloid physostigmine was isolated from the West African Calabar bean; applied to the eye it constricts the pupil and was found to lower intraocular pressure, and a related agent, pilocarpine, became a mainstay miotic for over a century. Roughly forty years later the pressure-lowering effect of adrenaline (epinephrine) was recognised, opening a second pharmacological avenue. This drug-by-drug history is the subject of Tony Realini's concise review, A History of Glaucoma Pharmacology.
The twentieth century then brought a steady cascade of new pressure-lowering classes. Oral and topical carbonic anhydrase inhibitors (beginning with acetazolamide in the 1950s) cut the eye's production of fluid; topical beta-blockers such as timolol, introduced in the late 1970s, became the dominant therapy of their era; and the prostaglandin analogues (latanoprost and its successors, from the 1990s) improved fluid drainage so effectively, with once-daily dosing, that they are now the usual first-line treatment. Alpha-agonists and, more recently, Rho-kinase inhibitors have added further options. Surgery, too, diversified far beyond iridectomy — into the fluid-shunting trabeculectomy, the laser procedures (laser trabeculoplasty and peripheral iridotomy), drainage implants, and the gentler family of "minimally invasive glaucoma surgeries."
One sober thread runs through this entire therapeutic history, and it deserves plain statement: every one of these treatments, from the Calabar bean to the newest implant, works chiefly by lowering intraocular pressure. Lowering pressure is, to this day, the only intervention proven in large clinical trials to slow glaucomatous vision loss — which is precisely why the long quest to feel, then see, then measure, and finally control eye pressure has been the spine of the whole story. Glaucoma cannot yet be cured and lost vision cannot be restored, but pressure-lowering treatment, started early, can preserve the sight a person still has.
The Modern Idea: Glaucoma as an Optic Neuropathy
The most important development of the late twentieth and early twenty-first centuries is conceptual rather than technological: medicine stopped defining glaucoma as high pressure and began defining it as a disease of the optic nerve. The decisive clue was clinical. Large studies established two stubborn facts that a pure pressure theory cannot accommodate. First, many people walk around with intraocular pressure above the statistical "normal" range yet never develop nerve damage — they have ocular hypertension, not glaucoma. Second, and more striking, a substantial fraction of people develop the unmistakable cupped disc and the characteristic loss of visual field while their measured pressure stays within the normal range — so-called normal-tension (or low-tension) glaucoma.
The resolution was to recognise that pressure is the leading risk factor for glaucoma, not its definition. Glaucoma is now understood as a progressive optic neuropathy: a chronic, characteristic loss of the retinal ganglion cells whose axons make up the optic nerve, producing the excavated cup that Heinrich Müller first drew in 1856 and the slowly contracting field of vision that von Graefe first charted. Raised intraocular pressure is the most important and the only readily treatable risk factor, but the individual nerve's vulnerability — influenced by blood flow, the structure of the supporting lamina, genetics, and age — helps explain why some nerves fail at "normal" pressure and others tolerate high pressure unharmed.
Seen this way, the whole arc of the history snaps into focus. The Greeks named a colour; Banister felt a hardness; Helmholtz's mirror revealed the cupped nerve; von Graefe learned to relieve the acute attack; Schiøtz put the pressure on a scale; the pharmacologists learned to lower it. The modern synthesis keeps all of these as partial truths and binds them together: glaucoma is an injury to the optic nerve, in which pressure is the chief but not the sole villain, detected by examining the nerve and the visual field and treated — for now — by lowering the pressure. Research today reaches beyond pressure altogether, toward neuroprotection and even regeneration of the optic nerve, in the hope of someday defending the sight that the glaukos eye has been quietly losing for twenty-five centuries.
Research Papers and References
The list below combines peer-reviewed historical reviews of glaucoma with curated PubMed and reference-resource links covering the etymology, the pressure concept, the ophthalmoscope, von Graefe's surgery, tonometry, and the modern optic-neuropathy model. Ancient and early-modern primary texts (the Hippocratic corpus, Guillemeau's and Banister's treatises) are named in the article as historical sources rather than as modern citations. Each external link opens in a new tab.
- Leffler CT, Schwartz SG, Giliberti FM, Young MT, Bermudez D. What was Glaucoma Called Before the 20th Century? Ophthalmology and Eye Diseases. 2015;7:21-33. — doi:10.4137/OED.S32004 (PMID 26483611; PMC4601337)
- Krogmann F, Lauer N. 2000 years under pressure — the history of glaucoma research. Acta Ophthalmologica. 2019;97(S263). — doi:10.1111/j.1755-3768.2019.8142
- Realini T. A History of Glaucoma Pharmacology. Optometry and Vision Science. 2011;88(1):36-38. — doi:10.1097/OPX.0b013e3182058ead (PMID 21131876)
- Etymology and ancient meaning of "glaucoma" / glaukos — PubMed: glaucoma history and etymology
- Richard Banister (1622) and the early link between "hardness of the eye" and intraocular pressure — PubMed: history of intraocular pressure and glaucoma
- Hermann von Helmholtz and the invention of the ophthalmoscope (1851) — PubMed: Helmholtz and the ophthalmoscope
- Heinrich Müller and the description of glaucomatous optic-disc cupping — PubMed: history of glaucomatous optic-disc cupping
- Albrecht von Graefe (1828–1870) and the introduction of iridectomy for glaucoma — PubMed: von Graefe and the development of ophthalmology
- Hjalmar Schiøtz and the history of the impression tonometer (1905) — PubMed: Hjalmar Schiøtz and his tonometer
- The history of intraocular-pressure measurement: before and after Schiøtz — PubMed: the pressure — before and after Schiøtz
- History of glaucoma surgery: from iridectomy to trabeculectomy and modern procedures — PubMed: history of glaucoma surgery
- Normal-tension glaucoma and glaucoma as a progressive optic neuropathy — PubMed: normal-tension glaucoma and optic neuropathy
- Intraocular pressure as a risk factor: evidence from the Ocular Hypertension and collaborative glaucoma trials — PubMed: intraocular pressure as a glaucoma risk factor
External Authoritative Resources
- National Eye Institute (NIH) — Glaucoma
- EyeWiki (American Academy of Ophthalmology) — History of Glaucoma
- PubMed — All research on the history of glaucoma
Connections
- Ophthalmology
- Glaucoma (Overview)
- All Conditions
- Cataracts
- Macular Degeneration
- Diabetes (and Diabetic Eye Disease)