Susac Syndrome
Susac Syndrome — also called retinocochleocerebral vasculopathy — is a rare autoimmune disease that attacks the tiny blood vessels of the brain, retina, and inner ear all at once. It was first described by Dr. John Susac in 1979. Because the classic triad of symptoms rarely appears all together at first, many patients are misdiagnosed with multiple sclerosis, a psychiatric illness, or a series of small strokes before the true diagnosis is made. With the right treatment, most people stabilize — but getting there quickly matters enormously for protecting sight, hearing, and memory.
Table of Contents
- What Is Susac Syndrome?
- How It Damages the Body
- Signs and Symptoms
- Getting a Diagnosis
- Why It Gets Misdiagnosed
- Treatment Options
- Outlook and Long-Term Recovery
- Key Research Papers
- Connections
- Featured Videos
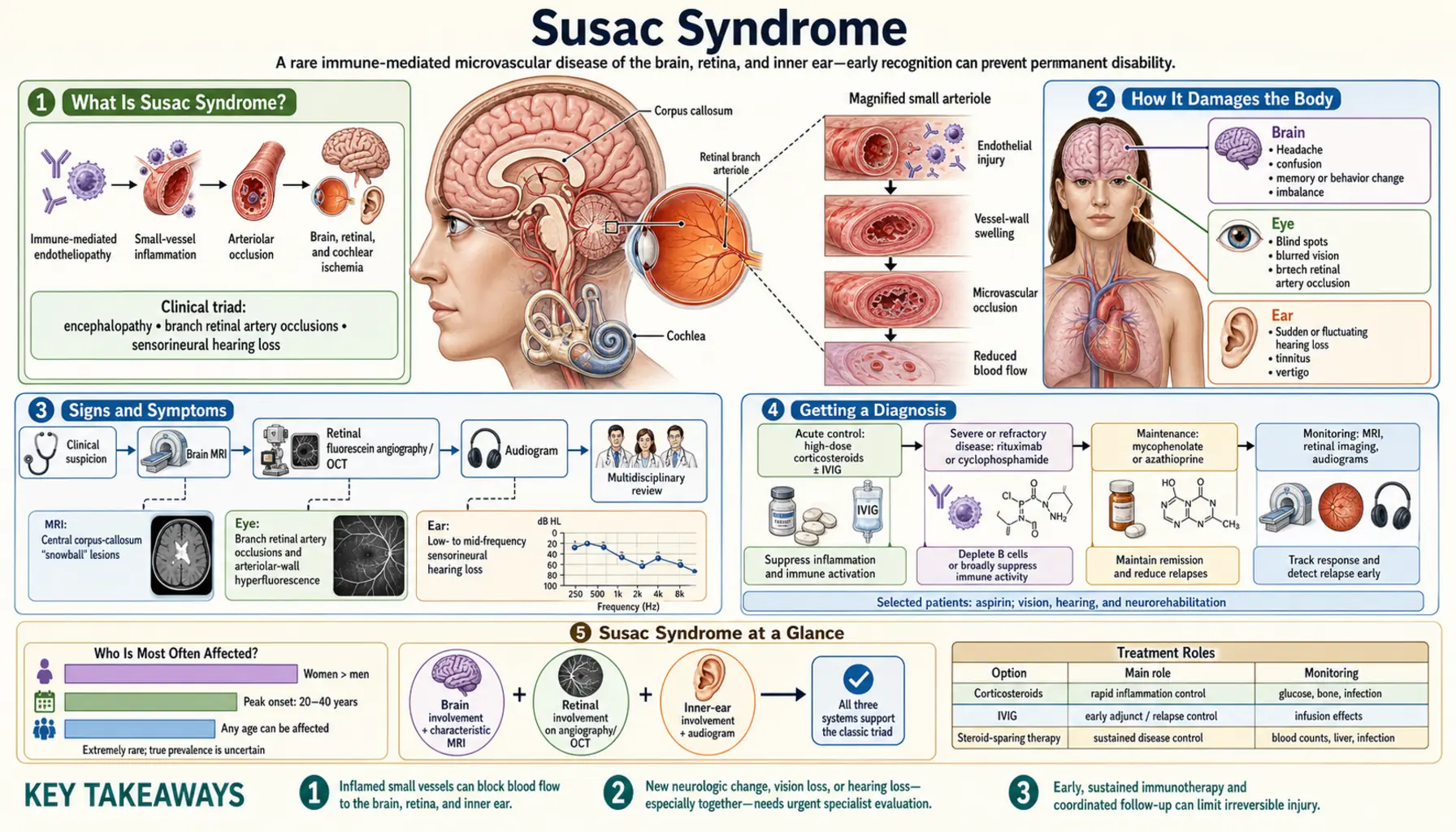
What Is Susac Syndrome?
Susac Syndrome is a rare autoimmune disease in which the body's own immune cells mistakenly attack the inner lining of tiny blood vessels in three specific organs: the brain, the retina (the light-sensing layer at the back of the eye), and the cochlea (the hearing organ of the inner ear). When these micro-vessels become inflamed and blocked, tissues downstream are starved of oxygen and begin to die.
The condition predominantly affects young women between the ages of 20 and 50, with the peak occurring in the third and fourth decades of life. Women are affected about three times more often than men. Because it is so rare — estimated at fewer than a few hundred new cases per year globally — many physicians have never seen a case, and the path to diagnosis is often long and frustrating for patients.
The hallmark clinical triad consists of:
- Encephalopathy — confusion, memory loss, personality change, and cognitive slowing from brain involvement
- Branch retinal artery occlusions (BRAOs) — blocked small arteries in the retina causing visual field loss
- Sensorineural hearing loss (SNHL) — damage to the cochlea causing hearing loss, tinnitus, and vertigo
Crucially, all three elements of the triad are rarely present at the same time when a patient first seeks care. Symptoms typically appear sequentially over weeks to months, which is one of the key reasons diagnosis is so frequently delayed. Patients often see a neurologist, an ophthalmologist, and an ear-nose-throat (ENT) specialist separately — each treating a piece of the puzzle without connecting it to a single unifying disease.
How It Damages the Body
The underlying mechanism of Susac Syndrome is an autoimmune attack on the endothelium — the delicate single-cell layer that lines every blood vessel. In Susac, the immune system specifically targets the endothelium of small blood vessels (microvasculature) in the brain, retina, and cochlea. The precise trigger that starts this attack is still unknown.
Current evidence points to CD8+ cytotoxic T-lymphocytes as the primary effectors. These T-cells appear to recognize and destroy endothelial cells in the microvasculature of the affected organs. Anti-endothelial cell antibodies and complement deposition have also been found in biopsy samples and blood, suggesting a broader immune dysregulation. Importantly, no specific diagnostic antibody has been identified — meaning there is no blood test equivalent to an AQP4 antibody in neuromyelitis optica or an MOG antibody in MOG antibody disease.
The result of this immune attack is inflammatory occlusion — the vessel walls swell, the lumen narrows, and blood flow stops. This plays out differently in each of the three affected organs:
In the Brain
The corpus callosum — the thick bundle of nerve fibers connecting the brain's two hemispheres — is the most characteristic site of injury. Inflammation and occlusion in the tiny perforating arteries that supply the central white matter of the corpus callosum produce small round areas of tissue death. On MRI, these appear as distinctive "snowball" lesions: small, punched-out bright spots floating in the center of the corpus callosum. The basal ganglia, thalamus, leptomeninges, and subcortical white matter are also frequently involved. As brain tissue dies, encephalopathy follows.
In the Retina
Inflamed microvasculature in the retina occludes the branch retinal arteries — the small vessels that supply segments of the retina. These branch retinal artery occlusions (BRAOs) in Susac tend to be multiple, bilateral, and located in the peripheral retina (away from the central fovea). This distinguishes them from the typical single, large, central BRAOs caused by blood clots or emboli in older patients with vascular risk factors. The peripheral retina occlusions cause peripheral visual field defects — missing patches in side vision — that patients may not notice immediately.
In the Cochlea
Damage to the cochlear microvasculature causes endolymphatic hydrops — a buildup of fluid in the inner ear's lymph system — and direct hair cell death from ischemia. The resulting sensorineural hearing loss affects low and mid frequencies first, which is the opposite of hearing loss from noise exposure or aging (which typically starts in the high frequencies). Patients often report a muffled, full, or distorted quality to low-pitched sounds. Tinnitus (ringing or buzzing) and vertigo (a spinning sensation) are common companions to the hearing loss.
Signs and Symptoms
Susac Syndrome can feel like several unrelated illnesses happening at once — or in sequence over months. Here is what patients commonly experience:
Cognitive and Neurological Symptoms
Brain involvement is often the most disabling feature in the long run. Patients describe a sudden or gradual change in their thinking: memory gaps, difficulty concentrating, slowed processing, word-finding difficulties, and confusion. Personality changes are common and deeply unsettling for families — a previously easy-going person may become irritable, paranoid, or emotionally labile. Some patients develop frank psychosis with hallucinations, leading to hospitalization in psychiatric units before the neurological diagnosis is made. Severe cases can progress to profound dementia over months if untreated.
Headaches are very common, often severe, and may be the first symptom. Some patients experience seizures. A sense of general fatigue and "brain fog" is nearly universal.
Visual Symptoms
Because the retinal occlusions tend to affect peripheral rather than central vision, some patients do not notice vision changes at first — or dismiss them as fleeting. Over time, patients may notice patchy blind spots, tunnel vision, or difficulty seeing to one side. Floaters (small moving shadows in vision) can occur. Acute, dramatic central vision loss can happen if a BRAO reaches the macula but this is less common in Susac than in other causes of retinal artery occlusion.
Hearing and Balance Symptoms
The hearing loss in Susac often comes on gradually and may be asymmetric — worse in one ear than the other, at least initially. Patients report sounds becoming muffled or distorted, particularly voices and low-pitched noises. A roaring or buzzing tinnitus in the affected frequency range is typical. Vertigo episodes — a sudden spinning sensation that can cause falls — occur in many patients and may be the first symptom that brings them to medical attention.
Disease Course Patterns
Susac Syndrome runs one of two courses:
- Monophasic: A single episode of disease activity lasting months to a few years, followed by remission. This pattern tends to produce less permanent damage if caught and treated early.
- Polycyclic (relapsing-remitting): Periods of active inflammation alternating with relative quiet. Each flare can add new injury to the brain, retina, or cochlea. This pattern is more challenging to manage and more likely to result in lasting deficits.
Across both patterns, active disease typically spans 2 to 5 years before eventually burning out. The cognitive effects, however, often persist long after the vasculopathy has quieted.
Getting a Diagnosis
There is no single blood test that confirms Susac Syndrome. Diagnosis rests on combining the clinical picture with results from several specialized tests. If your doctors suspect Susac, the following workup is standard:
MRI of the Brain
This is the most powerful diagnostic tool. The "snowball" lesions of Susac are small, round, punched-out bright spots on T2 and FLAIR sequences, located in the central white matter of the corpus callosum. This central location is the key distinguishing feature: in multiple sclerosis, corpus callosum lesions sit at the periphery and project outward perpendicular to the ventricular walls (the classic "Dawson fingers"). In Susac, they cluster in the center — giving the corpus callosum a "Swiss cheese" appearance on sagittal views. Leptomeningeal enhancement (contrast lighting up the brain's surface membranes), gray matter lesions, and deep gray matter (basal ganglia, thalamus) involvement may also be present.
Fluorescein Angiography (FFA)
An ophthalmologist injects a fluorescent dye into a vein in your arm, then photographs the blood flow through the retinal vessels. In Susac, FFA reveals multiple peripheral branch retinal artery occlusions, arteriolar wall staining (leakage of dye indicating inflammation), arteriovenous shunting, and segmental arterial narrowing. Finding multiple peripheral BRAOs in a young patient — especially a young woman — is highly suggestive of Susac until proven otherwise. FFA can detect retinal occlusions before they cause noticeable visual symptoms, making it a critical tool for early diagnosis and monitoring.
Audiogram
Formal hearing testing shows sensorineural hearing loss predominantly affecting low and mid frequencies. This pattern — a notch or dip in hearing at low pitches rather than the high-pitch loss of noise damage or aging — is characteristic of cochlear endolymphatic hydrops from Susac.
Optical Coherence Tomography (OCT)
OCT provides detailed cross-sectional imaging of the retinal layers. It can detect thinning of the retinal nerve fiber layer and ganglion cell layer corresponding to areas of past BRAO — even when the acute occlusion has resolved and may no longer be visible on FFA.
Cerebrospinal Fluid (CSF) Analysis
Lumbar puncture during active disease typically shows elevated protein and a pleocytosis (increased white blood cell count) — signs of central nervous system inflammation. Oligoclonal bands may occasionally be present, which can further complicate distinction from MS. Unlike MS, however, the pleocytosis in Susac often includes a notable proportion of red blood cells from the microhemorrhages caused by vessel wall inflammation.
Anti-Endothelial Cell Antibodies
Research labs can test for antibodies directed against endothelial cell antigens. However, these tests are not sensitive or specific enough for routine clinical use — a negative result does not rule out Susac, and a positive result requires clinical correlation.
Why It Gets Misdiagnosed
Susac Syndrome is one of the most commonly misdiagnosed neurological conditions — not because physicians are careless, but because the disease mimics several far more common conditions, and the three-organ triad rarely presents completely at once. Understanding the most common misdiagnoses helps patients advocate for themselves.
Multiple Sclerosis (MS)
This is by far the most frequent misdiagnosis. Both conditions affect young women, both cause white matter lesions on MRI, both may produce cognitive symptoms and visual disturbances, and both may show oligoclonal bands in the CSF. The critical distinction lies in the location of corpus callosum lesions: MS produces Dawson fingers at the periphery; Susac produces central snowballs. A careful neuroradiologist experienced with both conditions can usually tell them apart, but this is a subspecialty read — the distinction may be missed on routine reporting. Treatment for MS (interferons, glatiramer acetate) does not treat Susac and delays effective immunosuppression.
Psychiatric Illness
The psychiatric features of Susac — paranoia, psychosis, emotional dysregulation, personality change — are often the first manifestation that brings patients to medical attention. Without a brain MRI showing the characteristic snowball lesions, patients may be started on antipsychotics and admitted to inpatient psychiatric units. This misdiagnosis can persist for months, during which uncontrolled vasculopathy continues to damage the brain, retina, and cochlea. Any young person with new-onset psychosis should receive brain neuroimaging before a primary psychiatric diagnosis is assumed.
Transient Ischemic Attacks (TIAs) or Stroke
The visual field defects from retinal artery occlusion and the cognitive changes from brain ischemia can resemble TIAs or stroke, especially in the absence of visible snowball lesions on early imaging. Standard stroke workup (echocardiogram, Holter monitoring, hypercoagulable panel) will be negative, which should raise suspicion for a vasculitic or autoimmune cause.
Meniere's Disease
The low-frequency sensorineural hearing loss and vertigo of Susac closely resemble Meniere's disease, and patients with cochlear symptoms are frequently given this diagnosis. The distinction matters because the treatments differ entirely. If a patient with apparent Meniere's also develops cognitive changes or visual field loss, Susac should be urgently considered.
Treatment Options
Susac Syndrome requires aggressive, early immunosuppression to halt the inflammatory cascade before permanent damage accumulates in the brain, retina, and cochlea. Once neurons and retinal ganglion cells die or hair cells in the cochlea are destroyed, they do not regenerate — so the window for prevention matters enormously. Treatment is typically managed by a neurologist, often in collaboration with a rheumatologist, ophthalmologist, and audiologist.
High-Dose Corticosteroids
Steroids are the first-line, immediate treatment in active Susac. For severe presentations — acute encephalopathy, rapid vision loss, or new hearing loss — intravenous pulse methylprednisolone (1000 mg daily for 3 to 5 days) is typically given first, followed by oral prednisone at approximately 1 mg per kilogram of body weight per day. Steroids quickly reduce vascular inflammation and can halt progression, but they carry significant side effects with long-term use (bone loss, weight gain, blood sugar elevation, increased infection risk) and cannot be relied upon alone as maintenance therapy.
Intravenous Immunoglobulin (IVIG)
IVIG is a cornerstone of Susac treatment and has some of the strongest clinical evidence for this specific condition. It is typically given at a dose of 2 g/kg over 2 days, repeated every 4 to 8 weeks throughout the active phase of disease. IVIG works by modulating the immune system through multiple mechanisms — blocking Fc receptors on immune cells, neutralizing pathogenic antibodies, and suppressing T-cell activation — without the side effects of long-term steroids. Many patients notice meaningful improvement in cognitive function and stabilization of hearing and vision within a few infusion cycles.
Mycophenolate Mofetil
Mycophenolate mofetil (1 to 2 grams per day in divided doses) is a steroid-sparing immunosuppressant that works by blocking the proliferation of lymphocytes. It is frequently added as maintenance therapy once the acute phase is controlled, allowing steroid doses to be tapered. It is generally well tolerated, though it requires monitoring of blood counts and kidney function.
Rituximab
Rituximab, a monoclonal antibody that depletes CD20+ B cells and indirectly reduces plasma cell activity, is reserved for refractory or severe cases that do not respond adequately to steroids, IVIG, and mycophenolate. It is given as intravenous infusions and can produce durable remissions in some patients. Because it carries risks including serious infection, it is used when the risk of untreated disease outweighs the treatment risk.
Aspirin
Low-dose aspirin (81 mg daily) is recommended as an adjunct to immunotherapy. As an antiplatelet agent, it helps reduce the risk of new thromboembolic retinal artery occlusions on top of the inflammatory occlusions. It does not replace immunosuppression but provides an additional layer of protection for the retinal vasculature at low cost and risk.
Hearing and Vision Rehabilitation
Alongside immunotherapy, hearing aids should be fitted early for any significant sensorineural hearing loss. Early amplification helps preserve auditory processing pathways even when the underlying cochlear damage is not fully reversible. For patients with severe, irreversible hearing loss that does not respond to medical treatment, cochlear implants can restore meaningful functional hearing. Vision rehabilitation specialists can help patients adapt to persistent visual field defects. Ophthalmologic monitoring with fluorescein angiography every 3 to 6 months is standard during active disease to detect new retinal occlusions before they cause additional permanent loss. Note that intravitreal anti-VEGF injections — used for other retinal conditions — are not helpful for the inflammatory occlusions of Susac.
Monitoring and Tapering
Once disease activity is controlled, treatment is gradually tapered while closely watching for signs of relapse on MRI, FFA, and audiogram. Many patients remain on low-dose maintenance immunosuppression for years. Cognitive rehabilitation, occupational therapy, and mental health support are important parts of comprehensive care for the lasting effects of encephalopathy.
Outlook and Long-Term Recovery
The prognosis for Susac Syndrome is highly variable and depends heavily on how quickly the diagnosis is made and treatment is started. For patients who reach effective immunosuppression before extensive damage accumulates, the outlook is meaningfully better than for those who endure months or years of misdiagnosis.
Cognitive symptoms are the most persistent long-term burden. Even after the vasculopathy quiets, many patients experience ongoing memory difficulties, processing speed deficits, and fatigue that require cognitive rehabilitation and workplace accommodations. Some patients recover significantly over years; others carry permanent deficits.
Hearing loss is often the least reversible of the three affected systems. The delicate cochlear hair cells destroyed by ischemia do not regenerate. Patients with hearing loss at diagnosis should not expect full recovery but can benefit substantially from hearing aids or cochlear implants.
Visual outcomes depend on the location and extent of retinal occlusions. Peripheral BRAOs that spare the macula often cause visual field defects that patients adapt to remarkably well over time. Some degree of spontaneous improvement is possible as collateral circulation develops around occluded areas.
Active disease typically spans 2 to 5 years before burning out — meaning the autoimmune process eventually quiets spontaneously. This is more predictable in the monophasic pattern. In polycyclic disease, relapse can occur after months or even years of apparent remission, and long-term vigilance is required. Even after apparent remission, patients are generally followed with periodic MRI and ophthalmologic evaluation because of the relapse risk.
Despite the serious nature of the condition, many patients with Susac Syndrome — particularly those diagnosed and treated early — go on to lead full and active lives. Patient advocacy groups and specialized neurology centers familiar with rare autoimmune encephalitides provide the best chance of prompt diagnosis and optimal management.
Key Research Papers
The following peer-reviewed studies form the scientific foundation for understanding Susac Syndrome. Links go directly to PubMed for full citations and abstracts.
- Search PubMed — The original description of retinocochleocerebral vasculopathy: the landmark case report by Dr. John Susac establishing the syndrome that bears his name.
- Search PubMed — Systematic review of Susac Syndrome: comprehensive analysis of clinical features, diagnostic findings, treatment outcomes, and natural history across published cases.
- Search PubMed — MRI snowball lesions in Susac Syndrome: detailed characterization of the pathognomonic central corpus callosum lesions and their distinction from MS and other demyelinating diseases.
- Search PubMed — Corpus callosum lesions distinguishing Susac from MS: quantitative analysis demonstrating the diagnostic value of lesion location (central vs. peripheral) on MRI.
- Dörr J et al., 2009 — Anti-endothelial cell antibodies in Susac Syndrome: investigation of autoantibody profiles and their potential role in the pathophysiology of the microvasculopathy.
- Search PubMed — Fluorescein angiography in Susac Syndrome: characterization of retinal vascular findings including peripheral BRAOs, arteriolar wall staining, and arteriovenous shunting.
- Search PubMed — Retinal findings in Susac Syndrome: multimodal retinal imaging study describing the full spectrum of ophthalmologic manifestations across a patient cohort.
- Search PubMed — MRI and CSF biomarkers in Susac Syndrome: prospective study examining the diagnostic and prognostic value of neuroimaging and cerebrospinal fluid analysis.
- Search PubMed — Audiologic aspects of Susac Syndrome: detailed audiometric characterization of the low-frequency sensorineural hearing loss pattern and its clinical significance.
- Search PubMed — Treatment of Susac Syndrome: comprehensive treatment protocol including high-dose steroids, IVIG, mycophenolate, and aspirin with clinical outcomes data.
- Search PubMed — Susac Syndrome review: broad clinical, pathophysiological, and therapeutic review synthesizing the current state of knowledge for clinicians.
- Trebst C et al., 2013 — Long-term outcome in Susac Syndrome: follow-up study examining cognitive, visual, and auditory outcomes years after diagnosis and treatment.
Connections
- Neurology
- Multiple Sclerosis
- MOG Antibody Disease
- Anti-NMDA Receptor Encephalitis
- Neuromyelitis Optica
- Cerebral Venous Thrombosis
- Vascular Dementia
- Hearing Loss — the cochlear leg of the Susac triad, and why audiograms and hearing aids matter early.