Tuberculosis: History and Discovery
Tuberculosis is one of the oldest diseases known to afflict humanity — its scars survive in Egyptian mummies and in the curved spines of skeletons thousands of years old, and Hippocrates described its wasting form, phthisis, as the deadliest illness of his age. Yet its true nature stayed hidden for millennia. This page traces the long road from ancient observation to scientific proof: the unifying pathology of René Laennec, the naming of the disease by Johann Lukas Schönlein, Jean-Antoine Villemin’s demonstration that it was contagious, Robert Koch’s 1882 discovery of the bacterium Mycobacterium tuberculosis, and finally the vaccine and the first true cure. Throughout, dates and discoverers are stated only where reputable sources agree, and the historic names — consumption and the white plague — are kept in their proper place.
Table of Contents
- An Ancient Disease: Mummies, Bones, and Hippocrates
- Consumption and the White Plague
- Laennec, the Stethoscope, and a Unified Pathology
- Naming the Disease: Schönlein and “Tuberculosis”
- Villemin Proves It Is Contagious (1865)
- Robert Koch and the Discovery of the Bacterium (1882)
- The BCG Vaccine and the Tuberculin Legacy
- Streptomycin: The First True Cure (1943)
- From Sanatorium to the Modern Era
- Research Papers and References
- Connections
- Featured Videos
An Ancient Disease: Mummies, Bones, and Hippocrates
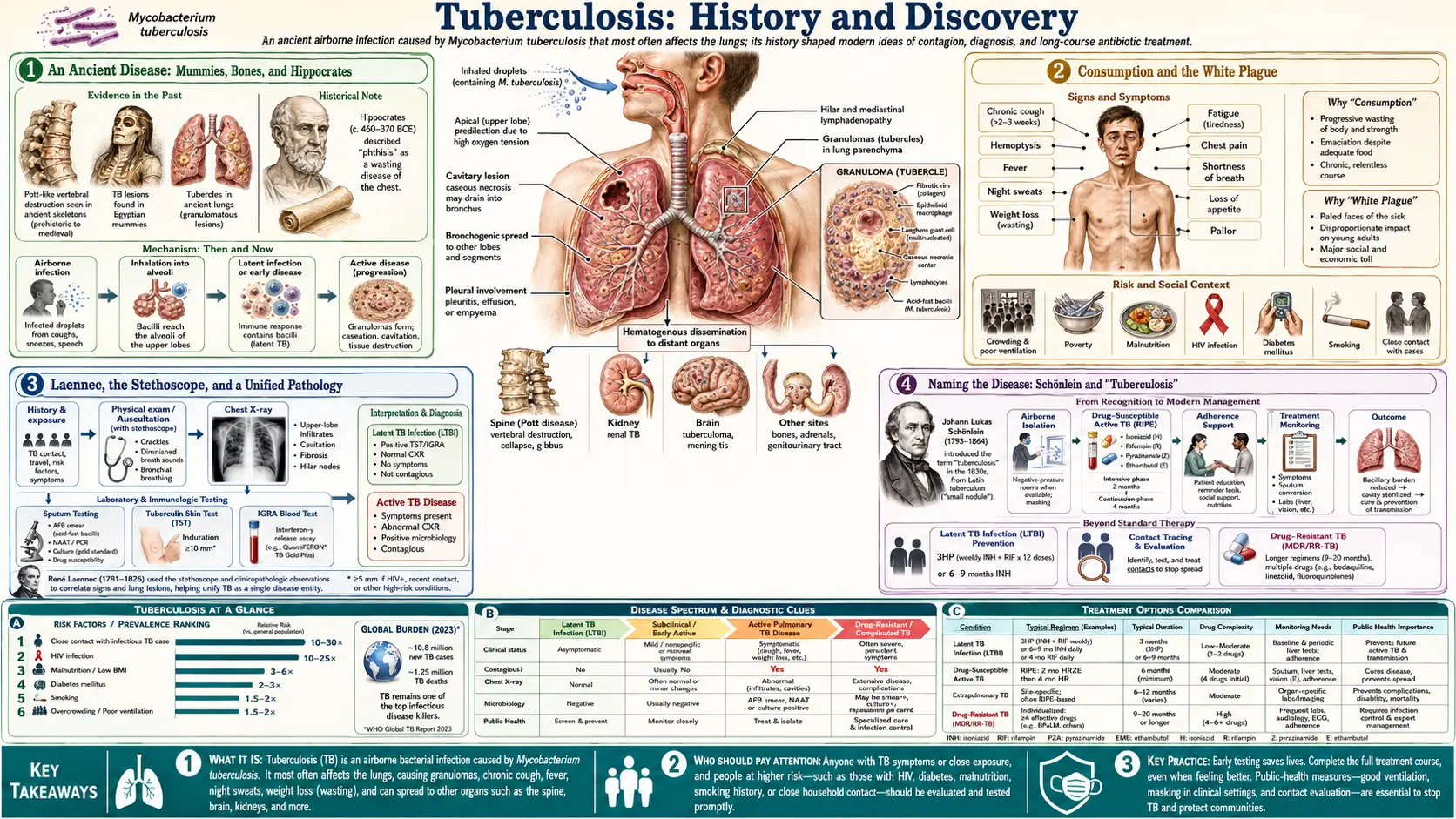
Tuberculosis has shadowed the human species for thousands of years, and unlike most ancient illnesses it left a physical record that modern science can read directly. When the disease settles in the spine it destroys the vertebrae and collapses the backbone into a sharp angular hump — a deformity now called Pott’s disease after the English surgeon Percivall Pott, who gave its classic clinical description in 1779. Skeletons bearing exactly this deformity have been recovered from ancient Egypt, with one predynastic spine roughly 5,000 years old showing the telltale kyphotic collapse, and tuberculous changes have since been confirmed in numerous mummies. The hunch-backed figures in some Egyptian art are widely thought to depict the same condition.
The evidence is not merely anatomical. Using the polymerase chain reaction, researchers have recovered fragments of Mycobacterium tuberculosis DNA from ancient Egyptian and other mummified and skeletal remains, placing the bacterium itself — not just a look-alike deformity — in human bodies millennia before anyone knew germs existed. Paleopathologists regard Pott’s disease as one of the oldest demonstrable diseases of humankind, documented in remains from Iron Age Europe, dynastic Egypt, and pre-Columbian South America alike.
Tuberculosis also entered the written record early. The Greek physician Hippocrates, around 400 BCE, described phthisis — the Greek word for “wasting” — as the most widespread and most fatal disease of his time, marked by fever, cough, and a relentless consuming of the body. He even warned colleagues against visiting patients in the late stages, a hint that physicians sensed something dangerous about the illness long before contagion could be proven. From this deep antiquity the disease would travel, under many names, all the way to the modern laboratory.
Consumption and the White Plague
For most of recorded history tuberculosis was known not by that name but by its effects. The most common English term was consumption, because the disease seemed literally to consume the sufferer — flesh, strength, and color all wasting away over months or years. The classical Greek phthisis carried the same meaning and remained in medical use into the nineteenth century. When the lungs were primarily involved, physicians spoke of pulmonary consumption or pulmonary phthisis.
By the eighteenth and nineteenth centuries tuberculosis had become so pervasive across Europe and North America that it acquired a darker epithet: the white plague. The name set it beside the medieval “black death,” and the “white” evoked both the pallor of its victims and the pale, drawn appearance that became tragically familiar. At its peak the disease is estimated to have caused an enormous share of all deaths in industrializing cities, striking the crowded poor especially hard while sparing no social class. It killed slowly and visibly, with chronic cough, breathlessness, drenching night sweats, fever, and — the sign families dreaded most — blood in the sputum.
This ubiquity matters for the history that follows. Because tuberculosis was everywhere, it was also intensely studied and argued over, and the long search for its cause was driven by the sheer weight of suffering it imposed — the pressure that eventually pushed a handful of physicians to overturn centuries of mistaken belief.
Laennec, the Stethoscope, and a Unified Pathology
For most of history, the many faces of tuberculosis — the wasting lung disease, the collapsed spine, the swollen neck glands of scrofula, the milky “tubercles” found scattered through the organs at autopsy — were treated as separate, unrelated illnesses. The figure who did more than anyone to draw them together was the French physician René Théophile Hyacinthe Laennec (1781–1826). In 1816 Laennec invented the stethoscope, originally a simple rolled wooden tube, which for the first time let a physician listen systematically to the sounds inside a living chest and correlate them with what was later found at autopsy.
In his landmark 1819 treatise on mediate auscultation (listening through an instrument), Laennec laid out a detailed pathology of tuberculosis. He argued that the tubercle — the small nodular lesion — was the fundamental, unifying feature of the disease wherever it appeared in the body, and he described how these lesions progressed, softened, and cavitated in the lungs. By tying the bedside signs he could hear to the lesions he could see after death, Laennec transformed tuberculosis from a vague clinical impression into a describable, trackable disease process. Tragically, Laennec himself is generally believed to have died of tuberculosis, in 1826, at the age of forty-five.
It is worth being precise about what Laennec did and did not establish. He unified the pathology — he showed that the tubercle was the common thread — but he did not identify a cause, and he did not prove the disease was contagious. Indeed, like most French physicians of his era, he leaned toward the view that consumption was constitutional or hereditary rather than transmissible. His contribution was the essential groundwork: a clear, lesion-based definition of the disease that later investigators could build upon.
Naming the Disease: Schönlein and “Tuberculosis”
The word tuberculosis itself is younger than the disease by thousands of years. It derives from the Latin tuberculum, meaning a small swelling or nodule — a direct reference to the tubercles that Laennec had placed at the center of the pathology. The German physician Johann Lukas Schönlein (1793–1864) is credited with introducing the term in the 1830s; the date is most often given as 1834, though some sources cite his first published use slightly earlier. Schönlein proposed “tuberculosis” precisely because the tubercle was the common element across the disease’s many forms.
Historians add an important caveat that this page keeps in view for accuracy: Schönlein’s naming was a naming, not a complete unification of every entity then recognized. He applied the term to disease characterized by tubercles, but the older categories — scrofula, phthisis, consumption — were not all immediately folded under the single banner by his coinage alone. The full conceptual merger of these conditions into one disease with one cause would not be settled until Koch’s work nearly half a century later. What Schönlein supplied was the durable name the world still uses.
The distinction between describing, naming, and explaining a disease runs through this whole history. The ancients described the wasting illness; Laennec unified its pathology around the tubercle; Schönlein named it tuberculosis; Villemin would show it was transmissible; and only Koch would discover its cause. Treating these as one event flattens a story that actually unfolded over centuries through many hands.
Villemin Proves It Is Contagious (1865)
Through the early nineteenth century the dominant view, especially in France, held that consumption was hereditary or constitutional — something a person was born prone to, not something they caught. The decisive challenge to that belief came from a French military physician, Jean-Antoine Villemin (1827–1892). Having noticed that soldiers crowded together in barracks seemed to develop tuberculosis at high rates — a pattern that looked more like an infection than an inheritance — Villemin set out to test the idea experimentally.
In the spring of 1865, Villemin inoculated rabbits with tuberculous material taken from humans (and, in further work, from cattle). He placed small fragments of tubercle and infected fluid into a wound behind the animals’ ears, keeping uninoculated rabbits as controls. The inoculated animals developed widespread tuberculous lesions; the controls did not. From this Villemin drew the conclusion that overturned centuries of doctrine: tuberculosis was a specific, transmissible, infectious disease caused by an inoculable agent, capable of passing from humans to animals, from cattle to animals, and from animal to animal. He published these findings in his treatise Études sur la Tuberculose.
Crucially, Villemin proved transmissibility without yet identifying what was transmitted — he demonstrated that an infectious agent existed without isolating or seeing it. His results, when presented, were at first resisted: many French physicians clung to the hereditary theory, and some German skeptics objected that merely introducing foreign matter into tissue could produce tubercle-like reactions. Yet Villemin had reframed the entire question. The search was no longer for a constitutional weakness but for a contagious cause — a germ — and that reframing set the stage directly for Robert Koch.
Robert Koch and the Discovery of the Bacterium (1882)
The single most important moment in the scientific history of tuberculosis came on the evening of 24 March 1882, when the German physician and microbiologist Robert Koch (1843–1910) addressed the Berlin Physiological Society and announced that he had identified the cause of the disease: a slender, rod-shaped bacterium, the tubercle bacillus, today called Mycobacterium tuberculosis. Where Villemin had proven that tuberculosis was contagious, Koch revealed the actual living agent responsible.
Koch’s achievement rested on extraordinary technical innovation. The bacterium is notoriously difficult to see and to grow, and Koch developed special staining methods to make it visible under the microscope and painstaking techniques to cultivate it in pure culture outside the body. He then satisfied a rigorous standard of proof — the logic later formalized as Koch’s postulates — by isolating the organism from diseased tissue, growing it in pure culture, and using that culture to reproduce the disease in healthy experimental animals. This chain of evidence established M. tuberculosis as the definitive cause rather than a mere bystander, and Koch’s lecture is often called one of the most important in the history of medicine.
The date has become a permanent marker in global health: the World Health Organization observes World Tuberculosis Day on 24 March each year to commemorate Koch’s announcement. For his work on the disease, Robert Koch was awarded the Nobel Prize in Physiology or Medicine in 1905. Honesty about the historical record requires one important note alongside the triumph: a few years after his discovery Koch promoted a preparation called tuberculin as a potential cure for tuberculosis. As a treatment it failed and the claim damaged his reputation — but tuberculin found lasting value in a different role, as the basis of the skin test still used to detect tuberculosis infection.
The BCG Vaccine and the Tuberculin Legacy
Identifying the germ opened two great practical frontiers: preventing infection with a vaccine, and curing those already infected with a drug. The vaccine came first. At the Pasteur Institute in France, the bacteriologist Albert Calmette and the veterinarian Camille Guérin set out to create a safe, weakened strain of the closely related cattle bacterium Mycobacterium bovis. Beginning around 1908, they repeatedly subcultured the strain — passing it through fresh growth medium well over two hundred times across roughly thirteen years — until it had lost the power to cause progressive disease while still provoking protective immunity.
The result was the bacille Calmette-Guérin, or BCG, vaccine. It was first given to a human infant in 1921 — a newborn whose mother had died of tuberculosis — and the child remained well. Named for its two creators, BCG went on to become one of the most widely administered vaccines in human history, given to infants across much of the world and still in use today. Its protection is partial and variable, strongest against severe childhood forms of tuberculosis such as TB meningitis, which is why the search for better vaccines continues; but BCG remains a landmark as the first and still the only licensed vaccine against the disease.
The vaccine’s arrival also illustrates how Koch’s “failed” tuberculin found redemption. Tuberculin could not cure tuberculosis, but injected into the skin it produces a reaction in people whose immune systems have already encountered the bacterium. That property became the tuberculin skin test — a simple, durable tool for detecting infection that, in updated form, has been used for over a century. Together, BCG and the tuberculin test turned Koch’s discovery into instruments of public health: one to prevent disease, the other to find hidden infection.
Streptomycin: The First True Cure (1943)
For all the progress in understanding and prevention, one thing remained beyond reach into the 1940s: a drug that could actually kill the tubercle bacillus inside a patient. Tuberculosis had resisted every weapon. The early wonder drugs were useless against it — the sulfonamides could not touch it, and even penicillin, which transformed the treatment of so many infections, had essentially no effect on M. tuberculosis. A person with active tuberculosis still faced, as their forebears had, only rest, nourishment, fresh air, and hope.
That changed in the laboratory of Selman Waksman at Rutgers University, where a research program systematically screened soil microorganisms for substances that could inhibit bacteria. In 1943, the graduate student Albert Schatz — working with Waksman and the researcher Elizabeth Bugie — isolated streptomycin from a soil bacterium, Streptomyces griseus. Streptomycin proved to be the first antibiotic effective against Mycobacterium tuberculosis, and when it was first given to gravely ill tuberculosis patients in the mid-1940s the effect could be dramatic. For the first time in human history, tuberculosis was curable with a drug.
The discovery’s legacy carries an honest complication. The Nobel Prize in Physiology or Medicine in 1952 was awarded to Waksman alone “for his discovery of streptomycin.” Schatz, who had performed the bench isolation, contested this; he later took legal action and was recognized as a co-discoverer of streptomycin, and historians today credit his central role. The science itself advanced just as quickly: doctors soon learned that streptomycin used alone allowed the bacteria to become resistant, a problem solved by combining drugs — isoniazid (introduced in the early 1950s) and later rifampin among them — into the multi-drug regimens that remain the foundation of tuberculosis treatment.
From Sanatorium to the Modern Era
Before effective drugs, the principal institution of tuberculosis care was the sanatorium — a residential facility, often in the mountains or by the sea, where patients spent months or years in bed rest, fresh air, sunlight, and careful feeding, in the hope that the body might wall the disease off on its own. The sanatorium movement, which grew through the later nineteenth and early twentieth centuries, was as much about isolating the contagious as about treating them. With the arrival of streptomycin and the drugs that followed, the rationale for these institutions collapsed, and across the mid-twentieth century the great sanatoria emptied and closed.
The long arc of this history — from a disease etched into ancient bones, to a named pathology, to a proven contagion, to an identified bacterium, to a vaccine and a cure — is one of medicine’s clearest triumphs. Yet tuberculosis was not conquered. It remains one of the world’s leading infectious causes of death, sustained by poverty, crowding, and weakened immunity, and it has been made far more dangerous in two ways the discoverers could not foresee: its deadly partnership with HIV, which cripples the immune defenses that normally hold the bacterium in check, and the rise of multidrug-resistant tuberculosis, strains that defy the very antibiotics that once made the disease curable.
Drug resistance is, in a sense, the modern echo of an old lesson. Just as the first patients given streptomycin alone bred resistant bacteria, today’s misuse and interruption of treatment breed strains that resist multiple drugs at once. The history on this page is therefore not a closed chapter but a living one: the names and dates belong to the past, but the disease they describe is still very much present, and the work that Laennec, Villemin, Koch, Calmette, Guérin, Schatz, and Waksman began is not yet finished.
Research Papers and References
The references below combine peer-reviewed historical reviews of tuberculosis with curated PubMed topic-search links into the primary literature on its paleopathology, discovery, and treatment. Historical works named in the article — Hippocrates on phthisis, Laennec’s 1819 treatise on auscultation, Schönlein’s coinage, Villemin’s Études sur la Tuberculose, and Koch’s 1882 lecture — are cited in the text as historical sources. Each link opens at the publisher or at PubMed (National Library of Medicine) in a new tab. Where a single year or date is contested among sources (for example, the exact year Schönlein introduced the term), the article flags the uncertainty rather than asserting one figure as settled fact.
- Cambau E, Drancourt M. Steps towards the discovery of Mycobacterium tuberculosis by Robert Koch, 1882. Clinical Microbiology and Infection. 2014;20(3):196-201. — doi:10.1111/1469-0691.12555
- Daniel TM. The history of tuberculosis. Respiratory Medicine. 2006;100(11):1862-1870. — doi:10.1016/j.rmed.2006.08.006
- Barberis I, Bragazzi NL, Galluzzo L, Martini M. The history of tuberculosis: from the first historical records to the isolation of Koch’s bacillus. Journal of Preventive Medicine and Hygiene. 2017;58(1):E9-E12. — PubMed: PMID 28515626
- Frith J. History of tuberculosis. Part 1 — phthisis, consumption and the white plague. Journal of Military and Veterans’ Health. 2014;22(2):29-35. — JMVH: phthisis, consumption and the white plague
- Cave AJE. The evidence for the incidence of tuberculosis in ancient Egypt. British Journal of Tuberculosis. 1939;33(3):142-152. — doi:10.1016/S0366-0850(39)80016-3
- Daniel VS, Daniel TM. Old Testament biblical references to tuberculosis. Clinical Infectious Diseases. 1999;29(6):1557-1558. — doi:10.1086/313562
- Tuberculosis in ancient Egyptian mummies — molecular paleopathology — PubMed: TB in ancient Egyptian mummies
- Jean-Antoine Villemin and the infectious nature of tuberculosis — PubMed: Villemin and the infectious nature of TB
- René Laennec, the stethoscope, and the pathology of pulmonary phthisis — PubMed: Laennec, the stethoscope, and TB pathology
- Robert Koch, the tubercle bacillus, and Koch’s postulates — PubMed: Robert Koch and the tubercle bacillus
- BCG vaccine — history of Calmette, Guérin, and the first human use in 1921 — PubMed: BCG vaccine history
- Streptomycin, Schatz, Waksman, and the first cure for tuberculosis — PubMed: streptomycin and the first TB cure
- Pott’s disease (tuberculous spondylitis) — history and paleopathology — PubMed: Pott’s disease history
- History of the sanatorium movement and tuberculosis care — PubMed: the tuberculosis sanatorium movement
External Authoritative Resources
- CDC — History of World TB Day (24 March)
- World Health Organization — Tuberculosis fact sheet
- PubMed — All research on the history of tuberculosis