Meningitis: History and Discovery
Meningitis is inflammation of the meninges, the three protective membranes that wrap the brain and spinal cord. For most of human history it was a mysterious, often fatal illness recognised only by its terrible symptoms — sudden fever, a stiff, arched neck, splitting headache, intolerance of light, and coma. Untangling it took more than a century of patient work: Robert Whytt gave the first clear account of tuberculous meningitis in a posthumous book of 1768; Gaspard Vieusseux described the epidemic (meningococcal) form after a Geneva outbreak in 1805; Anton Weichselbaum identified the bacterium, the meningococcus, in 1887; and Heinrich Quincke's lumbar puncture (1891) finally let physicians sample the cerebrospinal fluid and see the disease directly. Antiserum, then sulfa drugs and antibiotics, and finally vaccines transformed an almost-certain death sentence into a largely preventable, usually treatable illness. This page traces that story, distinguishing carefully between the bacterial, viral, and tuberculous forms.
Table of Contents
- What the Meninges Are and What Goes Wrong
- Ancient and Early Descriptions
- Robert Whytt and Tuberculous Meningitis (1768)
- Vieusseux and the Geneva Epidemic of 1805
- Weichselbaum and the Meningococcus (1887)
- Quincke's Lumbar Puncture (1891)
- From Antiserum to Sulfa Drugs and Antibiotics
- Vaccines and the Modern Era
- Research Papers and References
- Connections
- Featured Videos
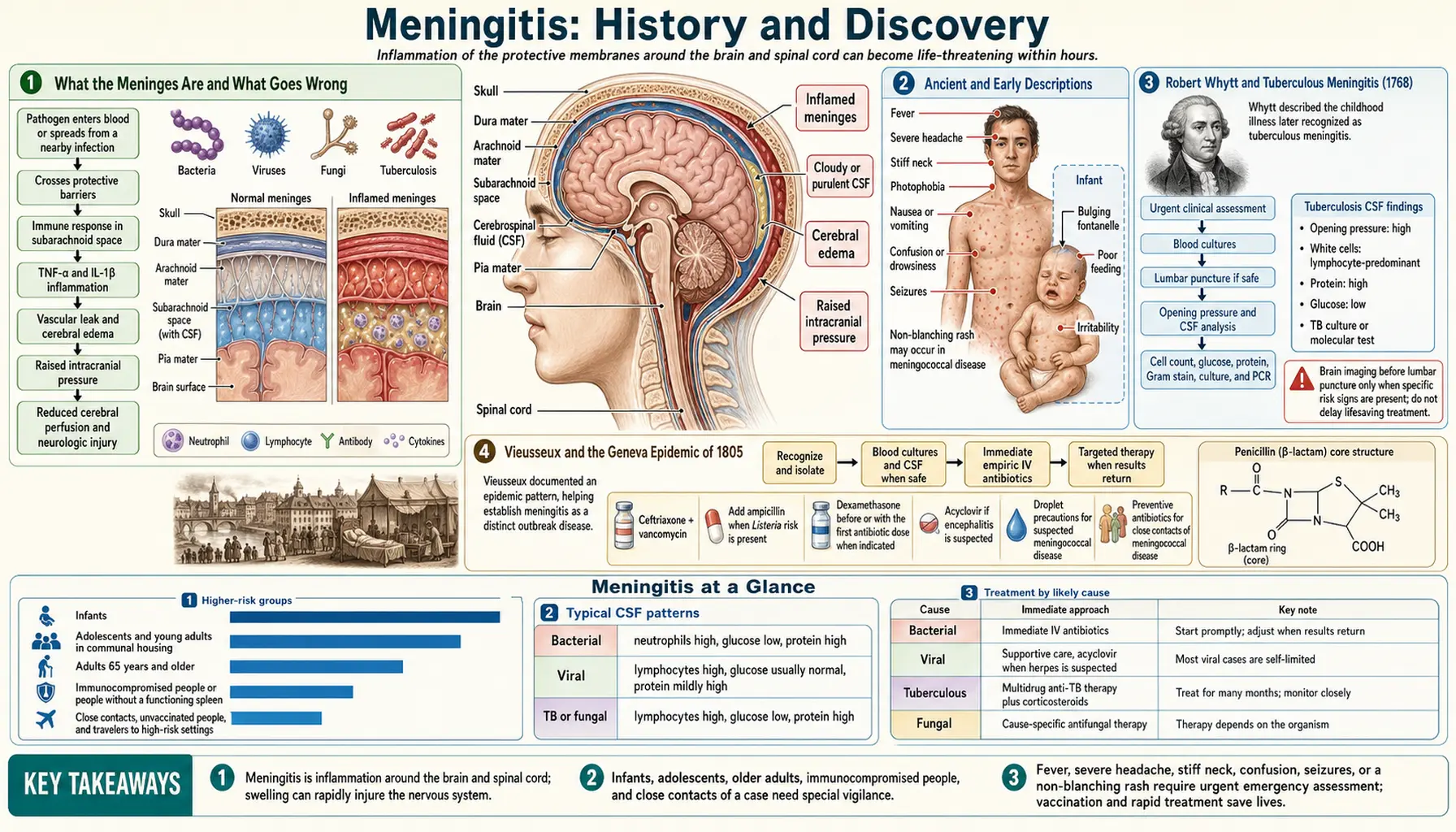
What the Meninges Are and What Goes Wrong
The brain and spinal cord do not sit bare inside the skull and spine; they are sheathed in three layered membranes called the meninges — from outermost to innermost, the tough dura mater, the web-like arachnoid mater, and the delicate pia mater that hugs the surface of the brain itself. Between the arachnoid and pia lies the subarachnoid space, filled with clear cerebrospinal fluid (CSF) that cushions the central nervous system. Meningitis is inflammation of these membranes and of the fluid that bathes them. Because the inflamed tissue lies in a rigid bony box, swelling has nowhere to go, which is why the disease so quickly produces crushing headache, a rigid neck, and, in severe cases, pressure on the brain itself.
The word meninges comes from the Greek for "membrane," and the classic triad of symptoms — fever, headache, and a stiff neck (later joined by the signs physicians call Kernig's and Brudzinski's) — has been recognised, if not understood, since antiquity. What changed over the centuries was not the symptoms but the explanation: only gradually did physicians learn that this single clinical picture could be produced by several very different causes.
It is essential to distinguish the main types, because their history, danger, and treatment differ sharply. Bacterial meningitis — caused chiefly by the meningococcus (Neisseria meningitidis), the pneumococcus (Streptococcus pneumoniae), and historically Haemophilus influenzae type b — is the most dangerous, killing rapidly without treatment. Tuberculous meningitis, caused by Mycobacterium tuberculosis spreading to the meninges, is slower but was equally fatal before antibiotics. Viral (aseptic) meningitis, most often caused by enteroviruses, is usually far milder and self-limiting. The history below follows each thread, because medicine discovered them at different times and by different routes.
Ancient and Early Descriptions
The symptoms of meningitis are old, even if the diagnosis is young. Ancient Greek physicians, including writers in the Hippocratic tradition, described patients seized by fever, severe headache, neck stiffness, delirium, and the backward-arching of the body that physicians now call opisthotonos — a picture entirely consistent with meningitis, though the Greeks had no way to know its cause and folded it into broader categories of "brain fever" and acute febrile illness. Similar descriptions recur through medieval and Renaissance medical writing. Because these accounts named no specific membrane disease and no causative agent, they are best read as recognitions of the syndrome rather than discoveries of meningitis as we now define it.
A clearer step came in the early modern period as anatomists, dissecting the dead, began to connect the symptoms with visible inflammation and fluid around the brain. The eighteenth century's growing interest in correlating bedside signs with post-mortem findings — the method championed by Giovanni Battista Morgagni in his 1761 work on the "seats and causes of diseases" — created the intellectual setting in which a specific membrane disease of the brain could finally be defined. It is against this background that Robert Whytt produced the first description modern readers recognise as a distinct form of meningitis.
Throughout this long pre-modern era, no one separated the bacterial, viral, and tuberculous forms, because the germ theory of disease lay centuries away. What the ancients bequeathed was an accurate, repeatedly confirmed picture of how meningitis looks — a clinical portrait so consistent that it would later let physicians recognise the disease at the bedside long before any laboratory could confirm it.
Robert Whytt and Tuberculous Meningitis (1768)
The first clear, systematic clinical description of a specific form of meningitis is credited to Robert Whytt (1714–1766), an Edinburgh physician and one of the leading figures of the Scottish medical Enlightenment. Whytt studied a series of children — about a dozen cases — who sickened and died with a characteristic, slowly progressing illness of the brain. His account, Observations on the Dropsy in the Brain, was published posthumously in 1768, two years after his death, when his son issued an edition of his collected works. (The "dropsy" in the title reflects Whytt's belief that a watery exudate accumulating in the brain caused the disease — the language of his era, before the cause was known.)
What makes Whytt's work a landmark is its precision. He recorded everything that could be observed at the bedside without modern laboratory tools, and he divided the illness into three stages according to changes in the character of the pulse — an early systematic attempt to chart the disease's course. The condition he described is now recognised as tuberculous meningitis: the form that arises when Mycobacterium tuberculosis seeds the meninges, typically in a child, during the bloodstream spread of tuberculosis. It is for this first clear description that Whytt is remembered in the history of paediatrics and neurology.
It is worth being precise about what Whytt did and did not establish. He gave an excellent clinical description and a plausible-for-its-time mechanism, but he could not have known the disease was caused by the tubercle bacillus — that organism would not be identified by Robert Koch until 1882, well over a century later. Whytt's achievement was descriptive and classificatory: he marked off a distinct, recognisable disease of the brain's membranes from the general fog of childhood fevers. That act of careful separation is exactly the kind of work on which later, cause-finding science would build.
Vieusseux and the Geneva Epidemic of 1805
If Whytt described the slow, sporadic, tuberculous form, the explosive epidemic form — what we now call meningococcal meningitis — was first clearly described a generation later by the Swiss physician Gaspard Vieusseux (1746–1814). In the early months of 1805, a frightening outbreak struck the area around Geneva, killing roughly thirty-three people in about three months, many of them children and young adults who were well in the morning and dead within a day or two. Vieusseux observed the outbreak closely and wrote it up, presenting his account in 1806 in the Journal de Médecine, Chirurgie et Pharmacie.
Vieusseux's report is regarded as the earliest comprehensive clinical description of epidemic cerebrospinal meningitis. He set down the now-classic features — abrupt onset, violent headache, high fever, stiff and retracted neck, vomiting, prostration, the purplish skin spots (petechiae) that signal meningococcal infection in the blood, and frequent rapid death — and noted the disease's tendency to strike in clusters. A closely related outbreak was described in New England the very next year, 1806, by the American physicians Lothario Danielson and Elias Mann, confirming that this was a recognisable epidemic entity on both sides of the Atlantic.
An important point of historical honesty: Vieusseux described the epidemic disease, not its cause. He could only suspect, not prove, that an external agent was responsible; the idea that a specific microbe caused it was a reasonable hypothesis of the era but lay beyond the reach of 1805 science. The cases he documented were almost certainly meningococcal, but that identification is a retrospective judgement made possible only after the bacterium was discovered eight decades later. Vieusseux gave medicine the clinical and epidemiological portrait of epidemic meningitis; finding the culprit fell to others.
Weichselbaum and the Meningococcus (1887)
The decisive step from describing the epidemic to naming its cause came in 1887, when the Viennese pathologist Anton Weichselbaum (1845–1920) identified the bacterium responsible for epidemic cerebrospinal meningitis. Working in the era when Koch's methods had made bacteriology rigorous, Weichselbaum examined the cerebrospinal fluid and tissues of patients who had died of meningitis. In a series of cases — he reported isolating the organism from six of eight patients with sporadic meningitis (the other two yielded the pneumococcus) — he found a distinctive coffee-bean-shaped diplococcus lying characteristically inside the body's immune cells.
He named it Diplococcus intracellularis meningitidis, a description encoded in three parts: Diplococcus for its paired, twin-sphere shape; intracellularis for its location inside white blood cells; and meningitidis for the disease it caused. The organism is known today as Neisseria meningitidis — the meningococcus — and it remains one of the leading causes of bacterial meningitis worldwide. Bacteriological study of the epidemics that followed, especially after 1897, firmly established this organism as the principal cause of epidemic cerebrospinal meningitis.
Weichselbaum's discovery is the hinge of the whole story. It distinguished the specific microbe (the meningococcus) from the disease it produced (epidemic meningitis) and from the diagnostic problem of detecting it. Once the cause was a known, culturable bacterium, meningitis could in principle be diagnosed in the laboratory, fought with agents aimed at that specific germ, and eventually prevented by a vaccine raised against it. Everything that followed — antiserum, sulfa drugs, antibiotics, and vaccines — depended on knowing what one was fighting.
Quincke's Lumbar Puncture (1891)
Knowing the cause was one thing; seeing it in a living patient was another. That became possible through the single most important diagnostic advance in the history of meningitis: the lumbar puncture, introduced by the German internist Heinrich Quincke (1842–1922) in 1891. Quincke presented the technique publicly at the Congress of Internal Medicine in Wiesbaden on 8 April 1891. By passing a fine needle between the lower lumbar vertebrae (typically the L3–L4 interspace) into the subarachnoid space, he could safely withdraw cerebrospinal fluid from a conscious patient — below the level where the spinal cord ends, so the cord itself is not at risk.
Quincke's original motivation was partly therapeutic: he reasoned that draining fluid might relieve dangerous pressure in children with hydrocephalus and in tuberculous meningitis. But the procedure's greatest gift turned out to be diagnostic. For the first time, physicians could examine the CSF directly — measure its pressure, judge whether it was clear or cloudy, count its cells, measure its protein and sugar, and, crucially, culture it for bacteria. A cloudy fluid teeming with neutrophils and low in glucose pointed to bacterial meningitis; a clear fluid with lymphocytes suggested the viral or tuberculous forms. The lumbar puncture turned a guessing game into a test.
The importance of this cannot be overstated, and it ties the earlier discoveries together. Weichselbaum's meningococcus could now be found in fluid drawn from a living patient rather than only at autopsy; the different types of meningitis — bacterial, viral, tuberculous — could finally be told apart at the bedside; and, within a few years, the very same spinal route would be used to deliver treatment directly to the infected fluid. Quincke was nominated for a Nobel Prize in 1909 for this work. Lumbar puncture and CSF analysis remain, to this day, the cornerstone of diagnosing meningitis.
From Antiserum to Sulfa Drugs and Antibiotics
Before any effective treatment existed, epidemic bacterial meningitis was a near-certain killer — case-fatality on the order of seventy to eighty per cent or higher. The first real therapy arrived through the work of Simon Flexner (1863–1946) at the Rockefeller Institute. During a severe New York epidemic beginning in 1905–1906, Flexner developed an antimeningococcal antiserum by immunising horses, and — recognising that the medicine had to reach the infected fluid around the brain — injected it directly into the spinal canal (the intrathecal route opened up by Quincke's technique). First used in human patients during a 1907 epidemic in Ohio, the serum cut the death rate roughly in half; by 1913 Flexner could report on some 1,300 treated patients, with mortality reduced to around thirty per cent. It was a partial victory, but the first one, and it remained the only specific therapy for nearly three decades.
The transformation came with the sulfonamides. In a landmark report published in JAMA on 24 April 1937, Francis Schwentker, Sidney Gelman, and Perrin Long described treating ten patients who had meningococcal meningitis with sulfanilamide; nine recovered. Sulfa drugs proved at least as effective as serum and far simpler to give, and they drove mortality from cerebrospinal fever down dramatically — from roughly seventy per cent toward twenty per cent or less. Cheap, stable, and easy to administer, sulfonamides carried the main therapeutic burden through the late 1930s and the Second World War, almost a decade before penicillin became widely available.
Then came the antibiotics. Penicillin, mass-produced during the 1940s, was highly active against the meningococcus and the pneumococcus and became a mainstay of treatment. Equally important for the slow, deadly tuberculous form was streptomycin, isolated in 1943 in Selman Waksman's laboratory (by graduate student Albert Schatz), the first drug effective against Mycobacterium tuberculosis — meaning that tuberculous meningitis, until then essentially always fatal, became treatable for the first time. Later antibiotics, including third-generation cephalosporins such as ceftriaxone, refined and broadened this success. The combined effect was historic: a disease that had been an almost-certain death sentence became, for most patients reached in time, a survivable illness.
Vaccines and the Modern Era
Treatment saves the sick; vaccines prevent people from ever falling ill, and the late twentieth century's great achievement against meningitis was prevention. The breakthrough came with conjugate vaccines, which chemically link a bacterium's sugar coat to a protein so that even infants — whose immune systems respond poorly to plain sugars — mount strong, lasting protection. The first and most dramatic success was against Haemophilus influenzae type b (Hib), once the leading cause of bacterial meningitis in young children. The first Hib conjugate vaccines were licensed beginning in 1987 and brought into routine infant use around 1990; within a few years invasive Hib disease in vaccinated populations fell by roughly 99 per cent, all but erasing a disease that had struck tens of thousands of children a year.
The same strategy was turned on the other two leading bacterial causes. Pneumococcal conjugate vaccines (the 7-valent PCV7 from 2000, later expanded to PCV13 and beyond) sharply reduced meningitis and other invasive disease from Streptococcus pneumoniae. Meningococcal conjugate vaccines against several serogroups (A, C, W, and Y) followed, and a separate protein-based vaccine was eventually developed against serogroup B, which had resisted the sugar-conjugate approach. A landmark public-health campaign, MenAfriVac, introduced from 2010, was designed specifically to drive serogroup A epidemics out of Africa's "meningitis belt," with striking results.
Two honest caveats keep this triumphant arc in proportion. First, vaccines exist for the major bacterial causes but not for most viral meningitis — which, fortunately, is usually mild and self-limiting and needs supportive care rather than antibiotics. Second, bacterial meningitis has not been conquered: it still strikes, still kills, and still demands immediate antibiotics, because the disease can go from first symptom to death within hours. Yet the long historical journey — from Whytt's bedside notes and Vieusseux's account of a terrified Geneva, through Weichselbaum's microscope and Quincke's needle, to serum, sulfa, antibiotics, and vaccines — turned one of humanity's most feared sudden killers into a disease that can largely be prevented and, when caught in time, usually cured.
Research Papers and References
The references below combine peer-reviewed historical reviews with curated PubMed topic-search links into the history of meningitis, its discovery, and its treatment. Historical primary texts — Robert Whytt's Observations on the Dropsy in the Brain (1768) and Gaspard Vieusseux's 1806 report in the Journal de Médecine, Chirurgie et Pharmacie — are named in the article as historical sources rather than as modern citations. Each link opens in a new tab.
- Tyler KL. A history of bacterial meningitis. In: Handbook of Clinical Neurology (History of Neurology). 2010;95:417-433. — doi:10.1016/S0072-9752(08)02128-3
- Manchanda V, Gupta S, Bhalla P. Meningococcal disease: history, epidemiology, pathogenesis, clinical manifestations, diagnosis, antimicrobial susceptibility and prevention. Indian Journal of Medical Microbiology. 2006;24(1):7-19. — doi:10.4103/0255-0857.19888
- Whytt R. Observations on the Dropsy in the Brain (1768) — historical review: Pearce JMS. Robert Whytt (1714–1766): from dropsy in the brain to tuberculous meningitis. Irish Journal of Medical Science. 2014. — doi:10.1007/s11845-014-1106-3
- Pearce JMS. Heinrich Quincke and lumbar puncture — history of the procedure. — PubMed: Quincke and the history of lumbar puncture
- Schwentker FF, Gelman S, Long PH. The treatment of meningococcic meningitis with sulfanilamide (landmark article, April 24, 1937). JAMA. — PubMed (PMID 6363729): Schwentker, Gelman & Long, sulfanilamide for meningococcal meningitis
- Flexner S. The results of the serum treatment in thirteen hundred cases of epidemic meningitis. Journal of Experimental Medicine. 1913. — PubMed (PMID 19867668): Flexner's 1300-case serum-treatment series
- Anton Weichselbaum and the discovery of Neisseria meningitidis (1887) — PubMed: Weichselbaum and the discovery of the meningococcus
- Gaspard Vieusseux and the 1805 Geneva epidemic of cerebrospinal meningitis — PubMed: Vieusseux and the history of epidemic meningitis
- History of the concept of tuberculous meningitis — PubMed (PMID 33326957): History of the Concept of Tuberculous Meningitis
- Streptomycin and the history of tuberculosis treatment (Waksman and Schatz) — PubMed: streptomycin and the history of TB treatment
- Impact of Haemophilus influenzae type b (Hib) conjugate vaccines on bacterial meningitis — PubMed: Hib conjugate vaccine impact on meningitis
- Pneumococcal and meningococcal conjugate vaccines — prevention of bacterial meningitis — PubMed: conjugate vaccines and the prevention of bacterial meningitis
- Two centuries of struggle against meningococcal disease (historical review) — PubMed: history of meningococcal disease
- Viral (aseptic) meningitis — enteroviruses and the differential diagnosis of meningitis — PubMed: viral (aseptic) meningitis and enteroviruses