Hepatitis C: History and Discovery
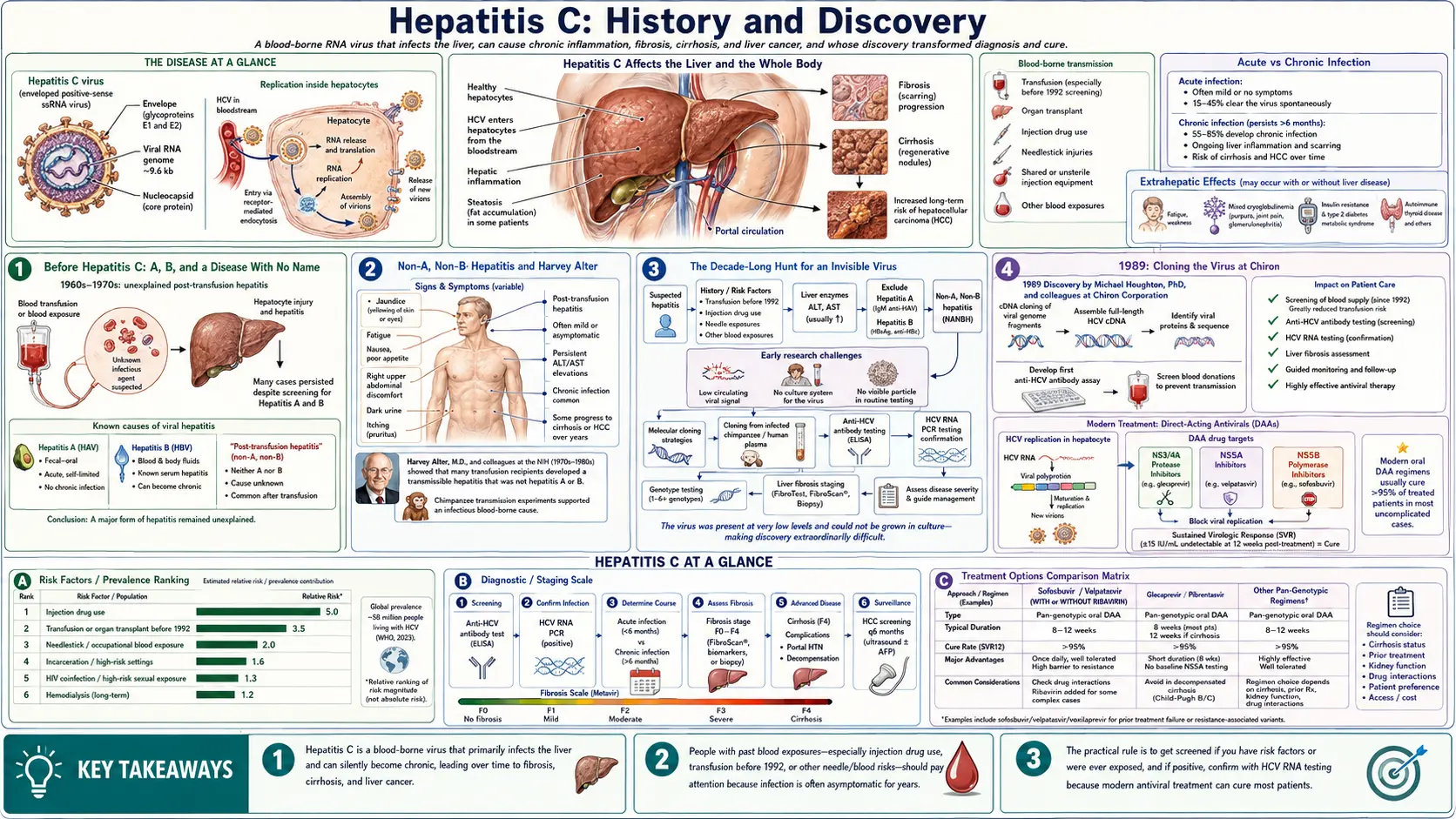
Hepatitis C is a viral infection of the liver that, for most of the twentieth century, hid in plain sight. After the viruses of hepatitis A and hepatitis B were identified, a stubborn, mysterious form of liver inflammation kept appearing in people who had received blood transfusions — an illness clinicians could only name by what it was not: “non-A, non-B hepatitis.” This page traces the detective story that followed: how Harvey J. Alter and colleagues at the U.S. National Institutes of Health proved in the 1970s that an unknown virus was responsible; how Michael Houghton, Qui-Lim Choo and George Kuo at Chiron Corporation — working with Daniel W. Bradley at the CDC — finally cloned and named the Hepatitis C virus (HCV) in 1989 using a bold new molecular method; how Charles M. Rice supplied the final proof that the virus alone caused the disease; and how blood screening and, ultimately, direct-acting antiviral drugs turned a once-incurable chronic infection into one that is now routinely cured. Alter, Houghton and Rice shared the 2020 Nobel Prize in Physiology or Medicine for this work.
Table of Contents
- Before Hepatitis C: A, B, and a Disease With No Name
- Non-A, Non-B Hepatitis and Harvey Alter
- The Decade-Long Hunt for an Invisible Virus
- 1989: Cloning the Virus at Chiron
- Charles Rice and the Final Proof
- Blood Screening and the End of Transfusion Hepatitis
- Direct-Acting Antivirals: From Interferon to Cure
- The 2020 Nobel Prize and the Road to Elimination
- Research Papers and References
- Connections
- Featured Videos
Before Hepatitis C: A, B, and a Disease With No Name
For centuries, doctors recognized epidemic jaundice — a yellowing of the skin and eyes signaling liver injury — without understanding its cause. By the mid-twentieth century it had become clear that “viral hepatitis” was not one disease but several. Two patterns were distinguished clinically and then biologically: hepatitis A, spread mainly through contaminated food and water and usually self-limiting, and hepatitis B, spread through blood and bodily fluids and capable of becoming chronic. The discovery of the hepatitis B surface antigen (the “Australia antigen”) by Baruch Blumberg in the 1960s — work that earned Blumberg a share of the 1976 Nobel Prize — gave the world its first blood test for a hepatitis virus and opened the modern era of hepatitis virology.
That breakthrough had an unexpected consequence: it revealed how much remained unexplained. Once blood banks could screen donors for hepatitis B, and once tests for hepatitis A followed, physicians expected post-transfusion hepatitis to largely disappear. It did not. A substantial fraction of people who received transfusions still developed liver inflammation weeks or months later, and their blood tested negative for both known viruses. Something else — unseen and unnamed — was being transmitted in the blood supply.
This is the gap into which Hepatitis C history begins. The disease existed, was common, and was dangerous, yet for years it had no agent, no test, and no name beyond a placeholder. Understanding how that placeholder became a named, cloned, and ultimately curable virus is one of the great achievements of modern medicine.
Non-A, Non-B Hepatitis and Harvey Alter
The central figure in the early chapter is Harvey J. Alter, a physician-scientist at the U.S. National Institutes of Health (NIH) Clinical Center, working in transfusion medicine. In the mid-1970s, studying blood from transfusion recipients and donors, Alter and his colleagues demonstrated systematically that most cases of post-transfusion hepatitis were caused neither by the hepatitis A virus nor by the hepatitis B virus. The cases were real, often led to chronic liver disease, and were clearly transmissible — but the culprit was none of the known agents.
Because the agent could be defined only by exclusion, the condition was given the deliberately provisional name “non-A, non-B hepatitis” (NANBH). Alter’s group showed that blood from affected patients could transmit the disease to chimpanzees — then the only susceptible experimental animal — and that the infectious material behaved like a virus, including being reduced by treatments that inactivate viral particles. As the official 2020 Nobel summary put it, Alter’s methodical work “defined a new, distinct form of chronic viral hepatitis.” A scientist at the U.S. Food and Drug Administration, Edward Tabor, independently used chimpanzee transmission studies to reach compatible conclusions, strengthening the case that an unknown transmissible virus was responsible.
Alter’s contribution was not the isolation of a virus — the tools of the day could not yet do that — but something arguably just as important: he proved, rigorously, that a specific unidentified infectious agent existed and was contaminating transfused blood. He turned a vague clinical impression into a defined scientific problem, and in doing so he set the agenda for the manhunt that followed. For this body of work Alter would later share the Nobel Prize.
The Decade-Long Hunt for an Invisible Virus
Knowing a virus existed was not the same as finding it. Through the late 1970s and 1980s, laboratories around the world tried and failed to isolate the non-A, non-B agent by conventional virology. The virus could not be reliably grown in cell culture, was present in blood at extraordinarily low concentrations, and could not be seen under the electron microscope in any consistent, identifiable form. Classical methods — culture the organism, visualize it, raise antibodies against it — simply did not work. For roughly a decade the agent remained, in practice, invisible.
The one experimental handle that did exist was the chimpanzee. Infected human plasma could transmit the disease to chimpanzees, which meant researchers had a way to produce and titrate infectious material and to test whether a candidate molecule came from the true agent. At the U.S. Centers for Disease Control and Prevention (CDC), Daniel W. Bradley worked extensively with the chimpanzee model and helped characterize the physical and chemical properties of the agent, including evidence that it was a small, lipid-enveloped virus. This painstaking animal work produced the high-titer infectious plasma that would prove essential to the eventual breakthrough.
What was needed was a fundamentally different strategy — one that did not require seeing or culturing the virus at all, but could instead fish its genetic material directly out of infected blood. That strategy came from the rapidly maturing field of molecular cloning, and it was pursued by a team at a young California biotechnology company.
1989: Cloning the Virus at Chiron
The decisive breakthrough came in 1989 from Chiron Corporation, then a young biotechnology firm in Emeryville, California. A team led by Michael Houghton and including Qui-Lim Choo and George Kuo, collaborating with Daniel W. Bradley at the CDC (who supplied infectious chimpanzee material), set out to identify the agent by molecular cloning rather than by classical virology — a then-novel and high-risk approach for an unknown pathogen.
Their method was ingenious. The team extracted nucleic acids from the blood of an infected chimpanzee and used them to build a large complementary DNA (cDNA) library — a collection of DNA fragments representing whatever genetic material was present, including, they hoped, fragments of the unknown virus. The central problem was finding the proverbial needle: which of the countless clones, if any, came from the virus? The team’s crucial insight was to screen the library not with a known probe but with blood serum from a non-A, non-B hepatitis patient, reasoning that such a patient’s immune system would carry antibodies against the virus’s own proteins. They looked for clones that produced a protein those antibodies recognized.
After an exhaustive search through millions of clones, a single positive clone emerged. It did not match any human or chimpanzee gene; it corresponded to a previously unknown RNA virus, related to the Flavivirus family (the group that includes yellow fever and dengue viruses). The team named it the Hepatitis C virus (HCV). For the first time, the invisible agent had a genome, a name, and — critically — a defined protein that could be used to build a diagnostic test. The findings were published in 1989, and the molecular-cloning strategy itself became a landmark demonstration that a pathogen could be identified directly from its nucleic acids without ever being grown or seen.
Charles Rice and the Final Proof
Cloning the virus answered “what is it?” but left a rigorous scientific question open: did this newly cloned virus, by itself, actually cause the disease — or was it merely a passenger that traveled alongside the true agent? Proving causation required showing that genetic material from the cloned virus alone could produce hepatitis. That proof came from Charles M. Rice, then at Washington University in St. Louis (and later at The Rockefeller University in New York).
Rice and his colleagues recognized that early attempts to make infectious HCV from cloned DNA failed in part because the assembled viral genome contained inactivating errors and because a previously overlooked region at the end of the genome was essential for replication. Rice engineered a corrected, full-length viral RNA — building a so-called consensus sequence that, at each position, used the most common (and presumably functional) genetic letter rather than a deleterious variant — and included the required genome region. When this engineered RNA was injected directly into the liver of a chimpanzee, it produced a genuine, replicating infection and clinical hepatitis.
This was, in the words of the Nobel committee, “the final proof that Hepatitis C virus alone could cause the unexplained cases of transfusion-mediated hepatitis.” Notably, Jens Bukh and colleagues at the NIH independently reported the construction of functional full-length HCV clones around the same time (1997), and the achievement is often credited jointly. Rice’s work closed the logical loop opened by Alter two decades earlier: an unknown agent had been shown to exist, then cloned and named, and now definitively shown to be the cause of the disease.
Blood Screening and the End of Transfusion Hepatitis
The single most immediate public-health payoff of the 1989 discovery was a blood test. Because the Chiron team had cloned a viral protein, they could develop an antibody (anti-HCV) screening assay almost at once. The first-generation test became available around 1990, and improved, more sensitive assays were rolled out for routine donor screening in the early 1990s. The effect on the blood supply was dramatic and rapid.
Before screening, transfusion-associated non-A, non-B hepatitis had been alarmingly common — historical estimates placed the risk on the order of roughly one infection per 50 to 200 units of blood transfused, depending on the population and era. Once donor blood could be screened for HCV antibodies (and later, with nucleic-acid testing, for the virus’s genetic material directly), that risk collapsed toward near-zero. The Nobel committee summarized the result plainly: the discovery enabled highly sensitive blood tests that “essentially eliminated post-transfusion hepatitis” in many parts of the world, sparing countless people from chronic liver disease.
This is a key reason the discovery is so celebrated: even before any cure existed, simply identifying the virus saved an enormous number of lives by making the blood supply safe. People who received transfusions before screening began — widely, before 1992 in the United States — are recognized as having been at elevated risk and may benefit from one-time HCV testing.
Direct-Acting Antivirals: From Interferon to Cure
Identifying HCV and proving it caused disease set the stage for the final act: treatment. For two decades the mainstay was interferon (later pegylated interferon), eventually combined with the antiviral ribavirin. These regimens were long, often a year, frequently caused flu-like illness, depression, anemia and other side effects, and cured only a minority to roughly half of patients depending on the viral genotype. A reliable cure for most people remained out of reach.
The transformation came from direct-acting antivirals (DAAs) — drugs designed to block specific HCV proteins the virus needs to copy itself. The pivotal model that made rational drug development possible was the HCV replicon and cell-culture systems built on the foundational molecular work, allowing the virus’s replication to be studied and targeted in the laboratory. A landmark arrived in December 2013, when the U.S. Food and Drug Administration approved sofosbuvir (brand name Sovaldi, from Gilead Sciences), a nucleotide inhibitor of the viral polymerase. Sofosbuvir was the first drug shown to be safe and effective against certain HCV genotypes without interferon, a turning point in the field.
Sofosbuvir was quickly built into all-oral, interferon-free combination regimens (pairing it with other DAAs such as ledipasvir, velpatasvir, and others). These modern combinations cure more than 95% of patients in a typical course of 8 to 12 weeks, with few side effects and a simple pill-based schedule. The achievement is historic in a literal sense: chronic hepatitis C became the first chronic viral infection that is routinely curable with a short course of medication. It is worth being precise here — sofosbuvir alone in 2013 was a breakthrough, but the across-the-board, >95% cure rates reflect the pan-genotypic combination regimens that followed in the years after.
The 2020 Nobel Prize and the Road to Elimination
On 5 October 2020, the Nobel Assembly at Karolinska Institutet awarded the Nobel Prize in Physiology or Medicine jointly to Harvey J. Alter (NIH), Michael Houghton (University of Alberta), and Charles M. Rice (Rockefeller University) “for the discovery of Hepatitis C virus.” The committee described a logical chain: Alter defined a new transmissible disease, Houghton’s team isolated and named the virus, and Rice proved the virus alone could cause it — together enabling blood tests and curative drugs that have saved millions of lives.
One part of the credit history deserves an honest note. The Nobel Prize, by its rules, recognizes at most three individuals, and the 1989 cloning was a team effort. Michael Houghton himself had earlier drawn attention to this: in 2013 he declined the Canada Gairdner International Award — and was widely reported to have similarly objected to other major honors — because he felt his Chiron colleagues Qui-Lim Choo and George Kuo, and the CDC’s Daniel W. Bradley, were not being recognized alongside him. These collaborators’ contributions to identifying HCV are well documented and are named throughout this page in fairness to the full record, even though the Nobel statutes limited the formal award to three laureates.
The story is not finished. With a safe blood supply and a curable infection, the World Health Organization has set a goal of eliminating viral hepatitis as a public-health threat by 2030 — targeting steep reductions in new infections and in hepatitis-related deaths. The remaining obstacles are no longer primarily scientific but practical: finding the millions of people who carry HCV without symptoms, expanding testing, and making the curative drugs affordable and accessible worldwide. The arc from an unnamed “non-A, non-B” illness to the realistic prospect of global elimination — in barely half a century — stands among the most hopeful narratives in the history of medicine.
Research Papers and References
The references below combine the foundational peer-reviewed papers in the discovery of Hepatitis C virus with curated PubMed topic-search links into the historical and clinical literature. Where a confident, stable identifier exists it is given as a DOI or PMID; otherwise a PubMed topic search is provided. Each link opens in a new tab at the National Library of Medicine, the journal of record, or the official Nobel and WHO pages.
- Choo QL, Kuo G, Weiner AJ, Overby LR, Bradley DW, Houghton M. Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science. 1989;244(4902):359-362. — doi:10.1126/science.2523562
- Kuo G, Choo QL, Alter HJ, et al. An assay for circulating antibodies to a major etiologic virus of human non-A, non-B hepatitis. Science. 1989;244(4902):362-364. — doi:10.1126/science.2496467
- Kolykhalov AA, Agapov EV, Blight KJ, Mihalik K, Feinstone SM, Rice CM. Transmission of hepatitis C by intrahepatic inoculation with transcribed RNA. Science. 1997;277(5325):570-574. — doi:10.1126/science.277.5325.570
- Bukh J, Purcell RH. A milestone for hepatitis C virus research: a virus generated in cell culture is fully viable in vivo (and the 1997 infectious-clone work). — PubMed: Bukh HCV infectious clone
- Lohmann V, Korner F, Koch J, Herian U, Theilmann L, Bartenschlager R. Replication of subgenomic hepatitis C virus RNAs in a hepatoma cell line. Science. 1999;285(5424):110-113. — doi:10.1126/science.285.5424.110
- Blight KJ, Kolykhalov AA, Rice CM. Efficient initiation of HCV RNA replication in cell culture. Science. 2000;290(5498):1972-1974. — doi:10.1126/science.290.5498.1972
- Alter HJ, Houghton M. Hepatitis C virus and eliminating post-transfusion hepatitis. Nature Medicine. 2000;6(10):1082-1086. — doi:10.1038/80394
- Houghton M. The long and winding road leading to the identification of the hepatitis C virus. Journal of Hepatology. 2009;51(5):939-948. — doi:10.1016/j.jhep.2009.08.004
- The Nobel Prize in Physiology or Medicine 2020 — official press release and scientific background (Alter, Houghton, Rice). — NobelPrize.org: 2020 Medicine press release
- Manns MP, Maasoumy B. Breakthroughs in hepatitis C research: from discovery to cure. Nature Reviews Gastroenterology & Hepatology. 2022;19(8):533-550. — doi:10.1038/s41575-022-00608-8
- Hepatitis C: milestones from discovery to clinical cure (historical review). — PubMed: HCV milestones from discovery to cure
- Sofosbuvir for chronic hepatitis C — pivotal trials and a decade of clinical use. — PubMed: sofosbuvir chronic hepatitis C
- Direct-acting antivirals achieving >95% sustained virologic response in chronic HCV. — PubMed: direct-acting antivirals HCV cure rate
- Non-A, non-B hepatitis: the chimpanzee transmission studies of the 1970s and 1980s. — PubMed: non-A non-B hepatitis chimpanzee transmission
External Authoritative Resources
- The Nobel Prize in Physiology or Medicine 2020 — Alter, Houghton & Rice
- World Health Organization — Hepatitis C fact sheet (and 2030 elimination goal)
- U.S. Centers for Disease Control and Prevention — Hepatitis C
Connections
- Infectious Disease
- Hepatitis C (Overview)
- Hepatitis (Viral Hepatitis Overview)
- Hepatitis B
- Cirrhosis
- Liver Disease
- Non-Alcoholic Fatty Liver Disease
- All Conditions