Acute Colonic Pseudo-Obstruction (Ogilvie's Syndrome)
- Overview — What Is Ogilvie's Syndrome?
- Pathophysiology — Autonomic Imbalance and the Colon
- Causes and Risk Factors
- Clinical Presentation — Massive Distension Without Obstruction
- Diagnosis — Imaging and Distinguishing True Obstruction
- Complications — Cecal Perforation and Ischemia
- Treatment — Conservative, Neostigmine, and Colonoscopy
- Neostigmine — The PONEC Trial and Practical Use
- Surgery — When All Else Fails
- Prognosis and Prevention
- Research Papers
- Connections
Overview — What Is Ogilvie's Syndrome?
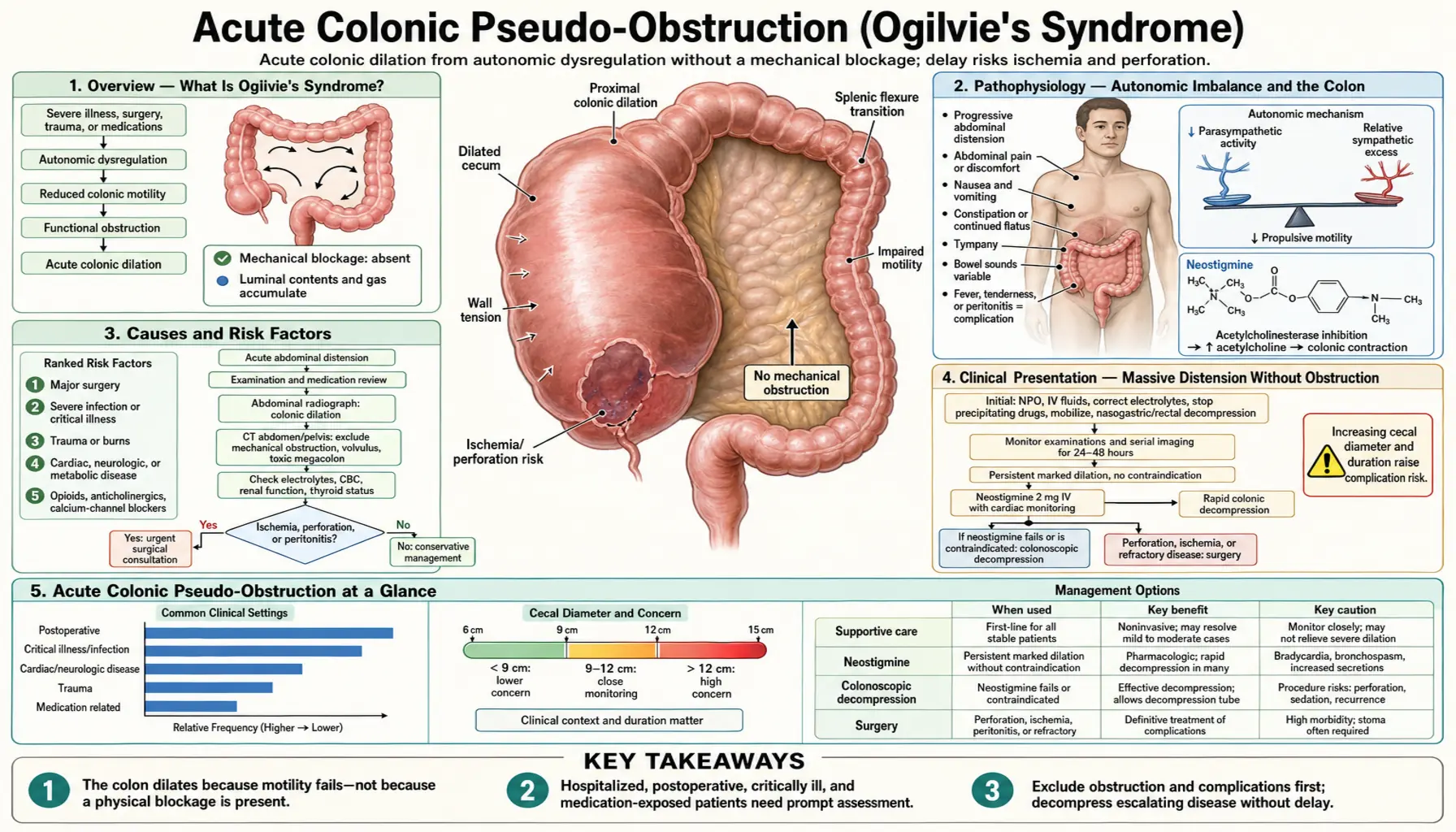
Acute colonic pseudo-obstruction (ACPO), also called Ogilvie's syndrome, is a condition in which the colon undergoes massive dilation in the complete absence of any mechanical blockage. The bowel behaves as though it is obstructed — it stops moving, fills with gas, and distends to dangerous proportions — yet a CT scan or colonoscopy reveals no tumor, stricture, hernia, or volvulus blocking the lumen. The obstruction is entirely functional: the colon's nervous system is not sending the signals needed for peristalsis.
The syndrome is named for Sir William Heneage Ogilvie, the British surgeon who described two cases in 1948. Both patients had retroperitoneal malignant infiltration of the celiac plexus, and Ogilvie proposed that autonomic nerve involvement disrupted colonic motility. His name has since been attached to the syndrome even in cases with quite different causes.
ACPO is almost exclusively a disease of hospitalized, critically ill patients. It develops after major surgery, trauma, serious medical illness, or prolonged opiate use — situations that overwhelm the autonomic nervous system's regulation of gut function. Recognizing it quickly matters enormously because treatment of ACPO is the opposite of treatment for true mechanical obstruction: surgery is usually the wrong answer for ACPO, while delaying drug treatment allows the colon to dilate further and perforate.
Pathophysiology — Autonomic Imbalance and the Colon
The colon's motility is governed by the autonomic nervous system through two competing pathways. Parasympathetic innervation — delivered to the left colon and rectum through the pelvic nerves (S2–S4) and to the right colon through the vagus nerve — promotes colonic contractions, peristalsis, and stool propulsion. Sympathetic innervation from the thoracolumbar splanchnic nerves (T6–L2) inhibits colonic motility and promotes fluid absorption and sphincter tone.
In ACPO, this balance is disrupted by an excess of sympathetic tone combined with reduced parasympathetic drive. The inhibitory sympathetic system dominates; the colon stops contracting; gas and fluid accumulate; the bowel dilates massively. The right colon — innervated predominantly by the vagus, which is more vulnerable to disruption in critically ill patients — is disproportionately affected. Gas accumulates primarily in the cecum and ascending colon, which dilate to dramatic diameters.
The cecum is the most vulnerable site for two interconnected reasons:
- Laplace's Law: Wall tension in a tube equals pressure multiplied by radius (T = P × r). The cecum has the largest diameter in the colon; at any given intraluminal pressure, the wall tension in the cecum is therefore greatest. Higher tension means higher risk of ischemia and perforation.
- Thin wall: The cecal wall is thinner than the sigmoid or descending colon. Thin walls under high tension are more prone to ischemic necrosis and rupture.
A cecal diameter exceeding 9–10 cm is considered worrying; a diameter exceeding 12 cm carries significant risk of perforation. Perforation of an unprepared, bacterially colonized colon causes fecal peritonitis, which has a mortality rate exceeding 40% even with prompt surgical intervention.
The pathophysiology explains why pharmacological restoration of parasympathetic tone — using neostigmine, an acetylcholinesterase inhibitor that prolongs the action of acetylcholine at parasympathetic nerve endings — so effectively and rapidly reverses ACPO. Within minutes of neostigmine infusion, the parasympathetic-inhibitory imbalance is corrected, peristalsis resumes, and gas explosively evacuates.
Causes and Risk Factors
ACPO almost always develops in the context of a serious underlying illness or recent surgery. The trigger is any condition that disrupts autonomic regulation of the colon — creating the sympathetic-parasympathetic imbalance that halts colonic motility.
Post-surgical causes (most common overall):
- Orthopedic surgery — particularly hip and knee replacement, spine surgery; retroperitoneal dissection disrupts the lumbar sympathetic chain and pelvic parasympathetics
- Cardiac surgery — cardiopulmonary bypass, cardiac revascularization; hemodynamic fluctuations + prolonged opiates
- Caesarean section and obstetric surgery — pelvic nerve disruption + post-operative opiates + abrupt hormonal shift
- Abdominal and pelvic surgery — direct retroperitoneal dissection; resection of adjacent viscera
- Renal transplantation — pelvic dissection + immunosuppressant medications + opiates
Medical illness triggers:
- Sepsis and severe infection — systemic inflammatory response disrupts autonomic tone throughout the body
- Trauma — particularly spinal cord injury (interrupts direct autonomic pathways) and retroperitoneal hematoma
- Myocardial infarction and cardiac failure — reduced splanchnic perfusion
- Neurological disease — Parkinson's disease, multiple sclerosis, stroke; central nervous system disorders that disrupt autonomic outflow
- Severe burns — systemic inflammatory response + prolonged immobility + opiates
- Respiratory failure on mechanical ventilation — positive pressure ventilation reduces venous return; sedation + opiates
Metabolic and electrolyte disturbances:
- Hypokalemia — potassium is required for smooth muscle polarization; hypokalemia impairs colonic contractility directly
- Hypomagnesemia — magnesium is a cofactor for many smooth muscle enzymes
- Hyponatremia — disrupts membrane potentials; impairs neuromuscular function
- Hypothyroidism — reduces gut motility at every level; can precipitate or perpetuate ACPO
- Hyperglycemia — impairs autonomic nerve function; diabetic autonomic neuropathy is a predisposing background
Medications:
- Opiates — among the most important contributors; mu-opioid receptor activation in the gut directly inhibits enteric neuron firing and smooth muscle contraction; post-operative opiate analgesia is a major driver in surgical ACPO
- Anticholinergic agents — block parasympathetic muscarinic receptors; directly impair the cholinergic drive to the colon
- Antipsychotics (particularly first-generation: haloperidol, chlorpromazine) — anticholinergic side effects
- Tricyclic antidepressants — significant anticholinergic burden
- Calcium channel blockers — reduce smooth muscle contractility
Clinical Presentation — Massive Distension Without Obstruction
ACPO develops over days rather than hours, distinguishing it from the acute abdominal catastrophe of true mechanical obstruction or colonic volvulus. Patients — typically already in the hospital, recovering from surgery or managing a serious illness — develop a progressively distending abdomen that may become enormous before the underlying condition is recognized.
Cardinal symptoms and signs:
- Abdominal distension — the hallmark; often massive and visually dramatic; the abdomen may be so distended it interferes with breathing, particularly in post-surgical patients who are already lying flat; tympanitic to percussion (a drum-like resonance from the gas-filled colon)
- Abdominal discomfort — a sense of fullness, pressure, or dull aching; notably, discomfort is often less severe than the dramatic degree of distension would suggest; this relative discordance between appearance and pain level is a clinical clue that distinguishes ACPO from true obstruction, where pain is typically more prominent
- Nausea and vomiting — especially bilious vomiting from the functional ileus
- Constipation and failure to pass flatus — the patient stops having bowel movements; absence of flatus is a key sign of complete functional obstruction
- Diminished or absent bowel sounds — the "silent abdomen" of ileus; in contrast, mechanical obstruction characteristically produces high-pitched, tinkling bowel sounds from vigorous peristalsis against the blockage
- Respiratory compromise — in severe cases, the massively distended colon elevates the diaphragm and restricts ventilation; patients may develop hypoxia, particularly if already on mechanical ventilation or post-operative
Alarming signs that suggest perforation or ischemia:
- Fever (temperature greater than 38.5°C) — suggests transmural inflammation or bacterial translocation
- Peritoneal signs: localized tenderness, rebound tenderness, guarding, rigidity — indicate perforation or impending perforation
- Hemodynamic instability: tachycardia, hypotension — suggest sepsis from bacterial translocation or perforation
- Leukocytosis with left shift, rising lactate — systemic signs of ischemia or infection
The presence of any peritoneal signs transforms the management picture entirely — this is now a surgical emergency regardless of cecal diameter, and the patient requires urgent operative intervention rather than pharmacological decompression.
Diagnosis — Imaging and Distinguishing True Obstruction
The fundamental diagnostic challenge in ACPO is distinguishing it from large bowel obstruction (LBO) from a mechanical cause — because the treatments are nearly opposite. In LBO, the mechanical blockage must be relieved (surgically or endoscopically) as the primary intervention; pharmacological approaches are ineffective. In ACPO, surgery is usually wrong as a first step and neostigmine or colonoscopic decompression is right.
Plain abdominal radiograph (the first test):
A supine abdominal X-ray is the appropriate first imaging step in a patient with abdominal distension in the hospital setting. In ACPO, the characteristic pattern is:
- Massively dilated right colon: cecum + ascending colon + transverse colon filled with gas; the cecum is typically the most dramatically dilated segment
- Gaseous dilation abruptly stops at the splenic flexure in classic cases (the junction of sympathetic and parasympathetic innervation territories), though dilation can sometimes extend into the left colon
- The small bowel may show some air-fluid levels (from the functional ileus), but typically less than in mechanical small bowel obstruction
- Absence of a discrete transition point where proximal dilated bowel meets collapsed distal bowel — this pattern suggests pseudo-obstruction rather than mechanical blockage
- Cecal diameter measurement is critical: measure on the AP supine film; record it; this number drives urgency of intervention
CT abdomen and pelvis with intravenous contrast (standard of care for confirmation):
- Confirms the pattern of colonic dilation and identifies the exact extent
- Identifies a transition point if one exists — a true mechanical obstruction typically shows a sharply defined transition from dilated proximal to collapsed distal bowel, with identifiable cause (mass, hernia, volvulus)
- Rules out closed-loop obstruction, volvulus, and colonic malignancy
- Pneumatosis intestinalis (gas within the bowel wall) or pneumoperitoneum (free air under the diaphragm) = perforation or impending ischemia; these findings mandate urgent surgery
- Evaluates mesenteric vessels for ischemia (colonic wall thickening, absence of contrast enhancement, mesenteric edema)
- Can identify underlying retroperitoneal or pelvic pathology that may be precipitating the autonomic disruption
Laboratory evaluation:
- Complete blood count: leukocytosis suggests ischemia or perforation
- Comprehensive metabolic panel: look for hypokalemia, hyponatremia, hypomagnesemia, hyperglycemia — all are reversible contributors to ACPO
- Thyroid-stimulating hormone: hypothyroidism is an important and correctable cause
- Lactate: elevated in bowel ischemia; rising lactate with signs of ACPO warrants urgent surgical consultation
- Blood cultures if fever is present
Complications — Cecal Perforation and Ischemia
The serious complications of ACPO arise from two processes that often coexist: ischemic necrosis of the colonic wall from overdistension, and bacterial translocation and perforation when the ischemic wall breaks down.
Ischemic necrosis: As the cecum dilates beyond 10–12 cm, the wall tension calculated by Laplace's Law approaches and then exceeds the perfusion pressure in the submucosal vessels. The mucosa — the most metabolically active and poorly perfused layer — becomes ischemic first. Mucosal ischemia allows intraluminal bacteria to invade the wall layers (bacterial translocation), producing local infection and accelerating wall breakdown. Eventually the full thickness of the wall may become necrotic — a process called transmural ischemia — which typically precedes frank perforation.
Perforation: When the ischemic wall ruptures, the bowel contents — which in an unprepared colon are densely bacterially colonized — spill into the peritoneal cavity. This produces fecal peritonitis, a catastrophic form of bacterial peritonitis with extremely high mortality. Published mortality rates for ACPO complicated by perforation range from 40% to over 70%, even with prompt surgical intervention. The high mortality reflects both the severity of fecal peritonitis and the serious underlying conditions these patients already have.
Risk thresholds for cecal diameter:
- Cecal diameter less than 9 cm: low immediate perforation risk; conservative management appropriate
- Cecal diameter 9–12 cm: moderate risk; appropriate for pharmacological intervention (neostigmine) or colonoscopic decompression; duration of dilation matters (greater than 3–4 days increases risk even at lower diameters)
- Cecal diameter greater than 12 cm: high risk; prompt intervention strongly indicated; some guidelines recommend neostigmine at this threshold without waiting for conservative measures to fail
Important caveat: perforation can occur at cecal diameters below 12 cm, particularly if the dilation has been sustained over many days or if the bowel is ischemic. The absence of peritoneal signs does not exclude beginning mucosal ischemia. Serial examination and imaging are essential components of conservative management.
Treatment — Conservative, Neostigmine, and Colonoscopy
Treatment follows a stepwise approach, escalating from conservative measures to pharmacological intervention to endoscopic decompression to surgery, based on response, cecal diameter, and clinical condition. The presence of peritoneal signs or perforation bypasses this stepwise approach and mandates immediate surgical consultation.
Step 1 — Conservative management (for mild cases: cecal diameter less than 12 cm, no peritoneal signs, duration less than 48–72 hours):
- Nothing by mouth (NPO) and bowel rest — eliminates further accumulation of swallowed air and ingested material
- Nasogastric tube suction — reduces swallowed air, which contributes to colonic gas load through the ileocecal valve
- Rectal tube placement — a Foley catheter or rectal decompression tube passed into the rectosigmoid can allow gas to vent from the left colon; limited benefit for right colon dilation but may provide some relief
- Correct metabolic abnormalities — this is essential and often underperformed: replace potassium to greater than 4.0 mEq/L; replace magnesium; correct sodium abnormalities; treat hypothyroidism; optimize glycemic control
- Ambulation — position changes and walking redistribute intraluminal gas and may stimulate peristalsis; patients who can safely ambulate should be encouraged to do so
- Discontinue offending medications — opiates are the most important; transitioning to non-opiate analgesia (ketorolac, acetaminophen, regional nerve blocks) may allow colonic motility to recover; also discontinue anticholinergics, antipsychotics, calcium channel blockers if clinically possible
- Conservative management alone achieves resolution in approximately 25–45% of patients within 24–48 hours; daily or twice-daily abdominal X-rays monitor cecal diameter
Step 2 — Pharmacological decompression with neostigmine: If conservative measures fail after 24–48 hours, or if cecal diameter is greater than 12 cm at presentation, neostigmine is the first-line pharmacological treatment (covered in detail in the next section).
Step 3 — Colonoscopic decompression: For patients in whom neostigmine is contraindicated or who fail to respond to neostigmine, colonoscopic decompression is the next intervention. The procedure is performed without bowel preparation (which is impossible in this setting and potentially dangerous). A colonoscope is advanced as far as possible into the dilated colon, and gas is aspirated as the scope is withdrawn. A decompression tube can be placed in the right colon to maintain decompression after the procedure. Success rates are 70–90% for initial decompression, but recurrence occurs in up to 40% of patients. The procedure is technically challenging because the colon is unprepared, dilated, and the patient is often medically fragile.
Neostigmine — The PONEC Trial and Practical Use
Neostigmine is an acetylcholinesterase inhibitor — it blocks the enzyme that breaks down acetylcholine at the neuromuscular junction and at parasympathetic nerve endings. By prolonging acetylcholine's action, neostigmine restores the parasympathetic drive to the colon, triggers peristaltic contractions, and allows the trapped gas and liquid to be expelled. The response when it works is immediate, dramatic, and unmistakable.
The PONEC Trial (Ponec et al., 1999, NEJM): This landmark randomized placebo-controlled trial established neostigmine as the standard of care for ACPO. Twenty-one patients received a single dose of intravenous neostigmine (2 mg over 3–5 minutes), and 20 received saline placebo. The results were striking:
- Neostigmine group: 10 of 11 patients (91%) responded with rapid colonic decompression — loud bowel sounds, passage of large amounts of gas and liquid stool, and visible reduction in abdominal distension within 30 minutes of infusion
- Placebo group: 0 of 10 patients responded
- Response was typically evident within 4–30 minutes of the infusion — the speed of response is one of the most striking aspects of the treatment
- 11 of the 19 nonresponders who crossed over to neostigmine then responded, further confirming the drug's efficacy
- The dramatic, near-immediate bowel decompression observed in responders — sometimes described as an "explosion" of gas and stool — underscored that the pathophysiology of ACPO is purely functional and immediately reversible by restoring cholinergic tone
Practical administration protocol:
- Dose: 2 mg intravenous over 3–5 minutes (slow infusion; rapid bolus increases side effects)
- Monitoring: Continuous cardiac monitoring during infusion and for at least 30 minutes afterward; bedside pulse oximetry; blood pressure monitoring
- Atropine at bedside: 0.5–1 mg atropine must be immediately available before neostigmine is given; it reverses bradycardia and bronchospasm if they occur
- Patient positioning: Patient should be in bed; prone or right-lateral decubitus position may help direct gas toward the right colon and cecum for expulsion
- Expected side effects: Abdominal cramping (common; often described as severe cramping immediately before the large bowel movement); hypersalivation; diaphoresis; nausea; bradycardia (most concerning; usually transient)
Contraindications to neostigmine:
- Suspected or confirmed mechanical bowel obstruction — neostigmine cannot propel stool through a physical blockage and increases the risk of perforation
- Heart rate less than 60 beats per minute (baseline bradycardia) — neostigmine causes further bradycardia through parasympathetic stimulation of the sinoatrial node
- Active bronchospasm or severe reactive airway disease — cholinergic stimulation causes bronchoconstriction
- Recent myocardial infarction or hemodynamic instability — the vasovagal effects of neostigmine are poorly tolerated
- Pregnancy — limited safety data; clinical judgment required
- Beta-blocker use and significant cardiac conduction disease are relative contraindications that require individualized risk assessment
A second dose of neostigmine can be given if the first dose produces a partial response; some protocols allow a second 2 mg dose 3–4 hours after the first if response is incomplete. Repeat dosing beyond two attempts has diminishing returns. After successful decompression with neostigmine, recurrence occurs in 10–20% of patients; a repeat dose can be effective for recurrent ACPO.
Surgery — When All Else Fails
Surgery is the treatment of last resort for ACPO in the absence of perforation, and its indication should be limited to specific, well-defined scenarios. The key principle is that ACPO is a functional disorder that rarely requires surgical resection of bowel — the colon itself is usually entirely normal and viable once decompression is achieved by other means.
Surgical indications in ACPO:
- Perforation — frank perforation with free air or fecal peritonitis; this is a true surgical emergency; neostigmine and colonoscopy have no role once perforation has occurred
- Ischemia without perforation — CT or clinical evidence of ischemic bowel (pneumatosis intestinalis, absent wall enhancement, peritoneal signs, rising lactate despite supportive care) warrants urgent surgical exploration
- Failure of all non-surgical measures — failure of conservative management AND neostigmine AND colonoscopic decompression in a patient with progressive dilation and clinical deterioration
Surgical options:
- Cecostomy — a tube cecostomy allows decompression of the cecum through a tube placed directly into the cecal lumen; a temporizing measure that preserves bowel continuity; appropriate when the bowel is viable and decompression alone is the goal
- Colonic resection — when ischemia or perforation involves a segment of colon, that segment must be resected; in perforation with fecal peritonitis, a Hartmann's procedure (resection with end colostomy and closure of the rectal stump) is usually performed rather than primary anastomosis, because anastomoses in the setting of peritonitis have very high leak rates
- Loop colostomy — rarely used; diverts the fecal stream proximal to an obstructed or ischemic segment; provides decompression without resection
Mortality for ACPO without perforation managed with neostigmine and colonoscopy is relatively low (less than 5% in most series) and reflects the underlying critical illness rather than ACPO itself. Mortality once perforation occurs rises sharply to 40–70%, underscoring the importance of timely pharmacological intervention to prevent this complication.
Prognosis and Prevention
The prognosis of ACPO itself — in the absence of perforation and without severe underlying illness — is generally good when recognized and treated promptly. Most patients who receive timely neostigmine decompression recover full colonic function with no long-term consequences. The colon is normal; the disorder is transient autonomic dysfunction; once corrected, the bowel resumes normal activity.
Prognostic factors:
- Cecal diameter at diagnosis — diameters greater than 12 cm are associated with higher complication rates even with treatment
- Duration of dilation before treatment — longer duration increases ischemia risk independent of diameter; patients who have been distended for more than 4–6 days are at higher risk even if diameter appears manageable
- Presence of peritoneal signs — indicates ischemia or early perforation; dramatically worsens prognosis
- Underlying critical illness — pneumonia, sepsis, multiorgan failure; ACPO mortality in these patients reflects the underlying condition
- Age and functional status — elderly patients with limited physiological reserve tolerate complications of ACPO poorly
Prevention strategies in high-risk patients:
- Early mobilization after surgery — even passive repositioning in immobile patients redistributes gas and stimulates peristalsis
- Minimize opiate use — multimodal analgesia protocols; regional anesthesia; non-opiate analgesics allow opiate dose reduction
- Correct electrolyte abnormalities proactively — maintain potassium and magnesium within normal range in post-operative and critically ill patients
- Early enteral nutrition — reduces gut bacterial overgrowth and maintains mucosal barrier integrity
- Alvimopan — a peripherally acting mu-opioid receptor antagonist; approved for accelerating GI recovery after bowel resection; blocks opiate effects in the gut while preserving systemic analgesia; may have a role in preventing ACPO in high-risk opiate-dependent patients
- Daily clinical assessment of abdominal examination in ICU and post-operative patients — serial abdominal girth measurement and bowel sound assessment; early recognition before critical cecal diameters are reached
Research Papers
- Ponec RJ, Saunders MD, Kimmey MB. Neostigmine for the treatment of acute colonic pseudo-obstruction. N Engl J Med. 1999;341(3):137–141. PMID: 10403850. DOI: 10.1056/NEJM199907153410301. The foundational RCT demonstrating 91% response rate to IV neostigmine vs 0% placebo.
- Ogilvie H. Large-intestine colic due to sympathetic deprivation: a new clinical syndrome. Br Med J. 1948;2(4579):671–673 — Search PubMed. DOI: 10.1136/bmj.2.4579.671. The original 1948 description by Sir William Ogilvie — two patients with celiac plexus involvement and massive colonic dilation.
- Saunders MD, Kimmey MB. Systematic review: acute colonic pseudo-obstruction. Aliment Pharmacol Ther. 2005;22(10):917–925 — Search PubMed. DOI: 10.1111/j.1365-2036.2005.02668.x. Systematic review of epidemiology, pathophysiology, and management of ACPO.
- Rameshshanker R, Wilson A. Acute colonic pseudo-obstruction (Ogilvie's syndrome). Surg Oxf. 2018;36(1):31–37. DOI: 10.1016/j.mpsur.2017.11.008. Comprehensive review covering pathophysiology, clinical features, and stepwise management including cecal diameter thresholds.
- De Giorgio R, Knowles CH. Acute colonic pseudo-obstruction. Br J Surg. 2009;96(3):229–239 — Search PubMed. DOI: 10.1002/bjs.6480. Review of autonomic pathophysiology, clinical recognition, and evidence base for treatment modalities.
- Rex DK. Colonoscopy and acute colonic pseudo-obstruction. Gastrointest Endosc Clin N Am. 1997;7(3):499–508 — Search PubMed. Defines the technique, indications, and outcomes of colonoscopic decompression in ACPO.
- Loftus CG, Harewood GC, Baron TH. Assessment of predictors of response to neostigmine for acute colonic pseudo-obstruction. Am J Gastroenterol. 2002;97(12):3118–3122 — Search PubMed. DOI: 10.1111/j.1572-0241.2002.07121.x. Identifies clinical predictors of neostigmine response and recurrence.
- Johnson CD, Rice RP, Kelvin FM, Foster WL, Williford ME. The radiological evaluation of gross cecal distension: emphasis on cecal ileus. AJR Am J Roentgenol. 1985;145(6):1211–1217 — Search PubMed. DOI: 10.2214/ajr.145.6.1211. Establishes radiographic criteria for ACPO and cecal diameter thresholds for perforation risk.
- van der Spoel JI, Oudemans-van Straaten HM, Stoutenbeek CP, Bosman RJ, Zandstra DF. Neostigmine resolves critical illness-related colonic ileus in intensive care patients with multiple organ failure — a prospective, double-blind, placebo-controlled trial. Intensive Care Med. 2001;27(5):822–827. PMID: 11430542. DOI: 10.1007/s001340100913. Confirms neostigmine efficacy in critically ill ICU patients — a population distinct from the PONEC trial setting.
- Mehta R, John A, Nair P, Raj VV, Mustafa CP, Suvarna D, Balakrishnan V. Factors predicting successful outcome following neostigmine therapy in acute colonic pseudo-obstruction: a prospective study. J Gastroenterol Hepatol. 2006;21(2):459–461 — Search PubMed. DOI: 10.1111/j.1440-1746.2006.04175.x. Prospective data on neostigmine response predictors in clinical practice.
- Trevisani GT, Hyman NH, Church JM. Neostigmine: safe and effective treatment for acute colonic pseudo-obstruction. Dis Colon Rectum. 2000;43(5):599–603 — Search PubMed. DOI: 10.1007/BF02235561. Safety profile and outcomes data for neostigmine in a prospective series; supports routine use in appropriately selected patients.
- Sgouros SN, Vlachogiannakos J, Vassiliadis K, Bergele C, Stefanidis G, Nastos H, Avgerinos A, Mantides A. Effect of polyethylene glycol electrolyte balanced solution on patients with acute colonic pseudo-obstruction after resolution of colonic dilation. Endoscopy. 2006;38(9):884–888 — Search PubMed. DOI: 10.1055/s-2006-944584. Evaluates strategies to prevent ACPO recurrence after initial decompression.