Polycystic Ovary Syndrome: History and Discovery
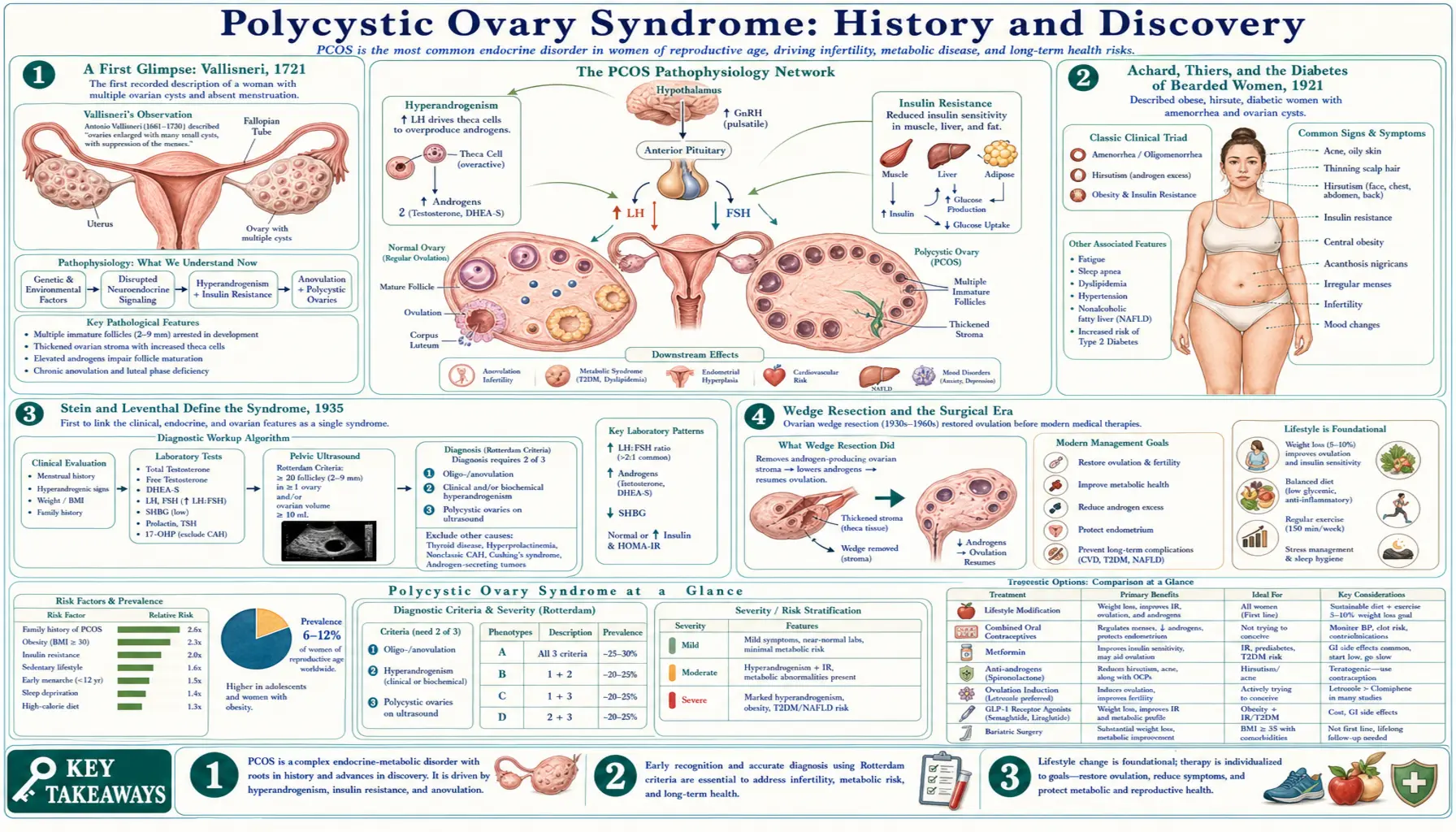
Polycystic ovary syndrome (PCOS) is among the most common hormonal conditions in women of reproductive age, yet its story is one of slow recognition, mistaken names, and shifting ideas. An Italian anatomist sketched its enlarged, glistening ovaries in 1721; a pair of French physicians tied androgen excess to diabetes in 1921; and in 1935 two Chicago gynecologists, Irving F. Stein and Michael L. Leventhal, finally drew amenorrhea, hirsutism, and polycystic ovaries together into a single recognizable syndrome — the “Stein-Leventhal syndrome.” The twentieth century reframed it again, first as an ovarian disorder, then — after Burghen and colleagues in 1980 — as a condition rooted in insulin resistance, and the 2003 Rotterdam criteria standardized how it is diagnosed. This page traces that 300-year arc and ends with the most consequential recent development of all: in 2026 a global consensus retired the “polycystic ovary” label as a misnomer, because the “cysts” are not cysts at all.
Table of Contents
- A First Glimpse: Vallisneri, 1721
- Achard, Thiers, and the “Diabetes of Bearded Women,” 1921
- Stein and Leventhal Define the Syndrome, 1935
- Wedge Resection and the Surgical Era
- From Stein-Leventhal to “Polycystic Ovary Syndrome”
- The Insulin Insight: Burghen, 1980
- Defining the Diagnosis: NIH 1990 and Rotterdam 2003
- A Name Under Question — and the 2026 Rename
- Legacy: What the History Teaches
- Research Papers and References
- Connections
- Featured Videos
A First Glimpse: Vallisneri, 1721
The earliest known anatomical description of what we now call polycystic ovary syndrome is usually credited to the Italian scientist and physician Antonio Vallisneri in 1721, more than two centuries before the condition acquired a name. In an account preserved in the historical literature, Vallisneri described a young married peasant woman, moderately stout and infertile, whose ovaries were larger than normal, lumpy, shiny, and whitish on the surface, and about the size of pigeon (dove) eggs. That vivid image — enlarged, glistening, smooth-surfaced ovaries in an infertile woman — maps closely onto the gross appearance of polycystic ovaries seen at surgery centuries later.
It is important to be precise about what this record does and does not establish. Vallisneri documented the anatomy — the visible morphology of the ovaries in one infertile woman — not a defined clinical syndrome with diagnostic criteria. He could not have known about the hormones, the ovulatory dysfunction, or the metabolic features that modern medicine ties together. His observation is best understood as the first surviving glimpse of the ovarian appearance, a single anatomical snapshot rather than a discovery of the disease as a whole. This attribution is reported in peer-reviewed historical reviews of PCOS, which name Vallisneri as the first to describe the characteristic ovaries.
Earlier still, physicians stretching back to antiquity had noticed loose threads of the same picture — women with irregular or absent periods who also showed masculinizing features such as excess body hair. Such scattered observations, however, were never assembled into a coherent entity. For nearly two hundred years after Vallisneri the trail goes largely cold, and the modern history of the syndrome does not resume in earnest until the twentieth century, when the connection between androgen excess, metabolism, and the ovaries began to come into focus.
Achard, Thiers, and the “Diabetes of Bearded Women,” 1921
The next major milestone came in 1921, when the French physicians Charles Achard and Joseph Thiers published a description that, for the first time in the modern record, explicitly linked androgen excess to disordered glucose metabolism. They reported a woman who combined masculinizing features — including excess facial and body hair — with diabetes, and the striking phrase associated with their account, le diabète des femmes à barbe (“the diabetes of bearded women”), has echoed through the literature ever since. The constellation later became known as the Achard-Thiers syndrome.
Why does a 1921 paper about diabetes belong in the history of PCOS? Because it planted, almost a lifetime early, the single idea that would eventually reorganize the entire field: that hyperandrogenism (too much male-type hormone) and a metabolic problem with blood sugar are somehow yoked together in the same patients. At the time the mechanism was a mystery, and the observation sat largely as a clinical curiosity rather than a unifying theory. It would take until 1980 for that metabolic thread — specifically insulin — to be pulled to the center of how PCOS is understood, as described below.
The Achard-Thiers observation also illustrates a recurring feature of this history: the syndrome was approached from several directions at once — by anatomists looking at ovaries, by gynecologists treating infertility, and by physicians puzzling over hair growth and diabetes — and these separate vantage points were only gradually recognized as views of one underlying condition.
Stein and Leventhal Define the Syndrome, 1935
The defining moment in the modern history of PCOS arrived in 1935, when two gynecologists at Michael Reese Hospital in Chicago, Irving Freiler Stein Sr. and Michael Leo Leventhal, published Amenorrhea Associated with Bilateral Polycystic Ovaries in the American Journal of Obstetrics and Gynecology (1935; volume 29, pages 181–185). The work had been presented the previous autumn at the Central Association of Obstetricians and Gynecologists meeting in New Orleans (November 1934). What set this paper apart from everything before it was that Stein and Leventhal reported a series of patients — classically described as seven women — who shared a recognizable pattern, rather than an isolated case.
Their patients showed a clinical picture that combined absence of menstruation (amenorrhea) or irregular cycles, excess body hair (hirsutism), and, in many, obesity, together with ovaries that were bilaterally enlarged and studded with small fluid-filled spaces — the “polycystic” appearance. Crucially, Stein and Leventhal could visualize the enlarged ovaries in living women using a now-obsolete technique called pneumoroentgenography (gynecography), in which gas introduced into the pelvis outlined the ovaries on X-ray. This allowed them to connect the outward symptoms with the internal ovarian morphology in the same patients — the conceptual leap that turned scattered observations into a named syndrome.
In recognition of this achievement the condition was, for decades, known as the Stein-Leventhal syndrome, a term still encountered today and still used as a synonym for PCOS. Their 1935 report is rightly regarded as the foundational clinical description, and the pair are commonly called the first true investigators of the disorder — with the explicit caveat, made throughout the modern historical literature, that Vallisneri had described the ovaries themselves two centuries earlier. The eightieth anniversary of the paper was marked in 2015 by a commemorative review in the same journal, a measure of how durable their contribution has proved.
Wedge Resection and the Surgical Era
Stein and Leventhal did not merely describe the syndrome — they offered a treatment, and a surprisingly effective one for its time. Their therapy was bilateral ovarian wedge resection: surgically removing a wedge-shaped portion of each enlarged ovary. The operation was originally undertaken in part to obtain tissue and reduce ovarian size, but it produced an unexpected and welcome result — many women resumed regular menstruation, and a substantial fraction who had been infertile went on to conceive. Stein later reported that the great majority of his patients regained menstrual function after the procedure.
For several decades wedge resection was the established surgical answer for anovulatory PCOS and a genuine source of hope for women facing infertility. Over time, however, its drawbacks became clear. The major problem was the formation of post-surgical adhesions — internal scar tissue around the ovaries and tubes — which could itself impair fertility, effectively trading a hormonal cause of infertility for a mechanical one. As safer and more effective medical options for inducing ovulation emerged in the second half of the twentieth century, open wedge resection by laparotomy was largely abandoned.
The surgical idea did not vanish, however; it evolved. Beginning with the work of Gjønnæss, who described laparoscopic ovarian “drilling” in 1984, surgeons sought to reproduce the ovulation-restoring benefit of wedge resection through small, targeted punctures or cauterization of the ovarian surface using minimally invasive keyhole surgery, aiming to avoid the heavy adhesions of the old operation. Laparoscopic ovarian drilling remains a second-line option for selected patients today. This surgical lineage — from open wedge resection in 1935 to laparoscopic drilling decades later — is one of the clearest threads of continuity in the history of PCOS treatment.
From Stein-Leventhal to “Polycystic Ovary Syndrome”
Through the mid-twentieth century the eponym “Stein-Leventhal syndrome” gradually gave way to more descriptive, mechanism-oriented names. As investigators came to view the ovary itself as the seat of the disorder, terms such as polycystic ovarian disease (PCOD) and, increasingly, polycystic ovary syndrome (PCOS) entered general use. The shift in language tracked a shift in thinking: away from honoring the original describers and toward naming the most visible anatomical feature — the many small follicles giving the ovary its characteristic appearance on examination and, later, on ultrasound.
The choice of the word “polycystic” was understandable but, with hindsight, unfortunate. The numerous small round structures that crowd the ovary in this condition are not pathological cysts in the everyday sense; they are immature ovarian follicles whose development has stalled. Each is a tiny, fluid-containing follicle arrested partway through maturation rather than a true cyst that needs removal or that signals danger. This distinction — cyst versus arrested follicle — is not a pedantic quibble; as described in the renaming section below, it has caused real and lasting confusion for patients and clinicians for generations.
The arrival of pelvic ultrasound in the late twentieth century reinforced the ovary-centered name, because the “string of pearls” or “black pearl necklace” pattern of many small follicles around the ovarian rim became an easily imaged, almost iconic hallmark of the condition. Ironically, the very imaging that made “polycystic” so vivid also helped reveal that the appearance is common, non-specific, and not by itself proof of disease — a tension that the formal diagnostic criteria of 1990 and 2003 would have to confront.
The Insulin Insight: Burghen, 1980
For decades PCOS was treated essentially as a reproductive and ovarian problem. That framework was decisively widened in 1980, when G. A. Burghen, J. R. Givens, and A. E. Kitabchi published Correlation of Hyperandrogenism with Hyperinsulinism in Polycystic Ovarian Disease in the Journal of Clinical Endocrinology & Metabolism (1980; volume 50, page 113). Studying women with polycystic ovarian disease against controls, they found that the affected women had elevated insulin levels and demonstrated a significant correlation between high circulating insulin (hyperinsulinemia) and high androgens (hyperandrogenism).
This was the pivotal modern insight. It revived, with hard hormone measurements, the half-century-old hint of Achard and Thiers that androgen excess and a glucose-handling problem travel together — and it relocated PCOS from a purely gynecologic disorder to a metabolic-endocrine one. The emerging model held that insulin resistance (the body's tissues responding poorly to insulin) drives the pancreas to secrete excess insulin, and that this surplus insulin acts on the ovary to amplify androgen production, helping explain the hirsutism, the disrupted ovulation, and the frequent association with weight gain and, later in life, type 2 diabetes.
The practical consequences were enormous. Once hyperinsulinemia was recognized as a central driver in many patients, it became logical to treat PCOS with insulin-sensitizing drugs. Velazquez and colleagues reported in 1994 that the diabetes medication metformin reduced insulin, androgens, and blood pressure while helping to restore normal menstruation in women with PCOS — opening a metabolic avenue of treatment that complemented the older reproductive approaches and that remains widely used. The insulin story is why modern care for PCOS attends as much to blood sugar, weight, and cardiovascular risk as to fertility.
Defining the Diagnosis: NIH 1990 and Rotterdam 2003
By the late twentieth century PCOS was widely recognized but inconsistently defined — different clinics and countries diagnosed it differently, which made research hard to compare and patients hard to count. The first major attempt to impose order came at a 1990 expert conference sponsored by the U.S. National Institutes of Health (through the NICHD). The resulting NIH 1990 criteria framed PCOS chiefly as an androgen-excess disorder of exclusion, requiring (in order of emphasis) clinical and/or biochemical hyperandrogenism plus oligo- or anovulation, after other conditions that mimic it had been ruled out. Notably, the 1990 criteria did not require the polycystic ovaries to be visible on ultrasound.
The most influential redefinition followed at a 2003 workshop in the Netherlands, producing the Rotterdam criteria, published in 2004 in Fertility and Sterility and Human Reproduction under the ESHRE/ASRM consensus (the European and American reproductive-medicine societies). Rotterdam broadened the definition by requiring any two of three features: (1) oligo- or anovulation, (2) clinical and/or biochemical hyperandrogenism, and (3) polycystic ovarian morphology on ultrasound. Because only two of the three are needed, Rotterdam recognizes several subtypes — including women who meet the definition without overt hyperandrogenism — and so casts a wider net than the 1990 NIH definition.
The Rotterdam framework is the most widely used today and underpins current international guidelines, though it has been debated ever since. Critics note that the broader, two-of-three approach captures milder phenotypes and leans on an ovarian-ultrasound criterion that is common in healthy young women, while supporters value its recognition that PCOS is a spectrum rather than a single fixed picture. A later Androgen Excess and PCOS Society statement re-emphasized hyperandrogenism as the core feature. The existence of three competing criteria sets — NIH 1990, Rotterdam 2003, and AE-PCOS 2006 — is itself a telling sign of how genuinely difficult this syndrome has been to pin down.
A Name Under Question — and the 2026 Rename
For years, clinicians and patient advocates argued that “polycystic ovary syndrome” was an actively harmful misnomer. The objections were concrete. First, the “cysts” are not cysts — they are arrested follicles, so the name describes something that, strictly speaking, isn’t there. Second, by foregrounding the ovary, the name obscured that PCOS is a whole-body, multi-system condition involving insulin resistance, metabolism, weight, skin, fertility, and mental health — not merely an ovarian problem. Third, the ovary-centric label was blamed for diagnostic delay and fragmented care, with a large share of patients reporting long waits and multiple clinicians before diagnosis. Some affected individuals who do not identify as women, and emerging discussion of analogous androgen-metabolic traits in men, further strained a name anchored to the ovary.
That long-running debate reached a resolution in 2026. On May 12, 2026, a global consensus — published in The Lancet and announced by bodies including the Endocrine Society — introduced a new name: Polyendocrine Metabolic Ovarian Syndrome (PMOS). The initiative was the product of roughly fourteen years of international collaboration led by Professor Helena Teede (Monash University) together with colleagues including Professor Terhi Piltonen, Anuja Dokras, and patient-advocate leaders, drawing on more than 50 patient and professional organizations and tens of thousands of survey responses from people with lived experience. The new name was chosen to foreground the condition's hormonal (“polyendocrine”) and metabolic nature while retaining the ovarian dimension.
The change is being introduced gradually rather than overnight: reports describe a multi-year transition, with the new terminology slated for full adoption in the next international guideline update toward the end of the decade. In practice this means readers will encounter both names for some time — the long-familiar “PCOS” and the newer “PMOS” — referring to the same condition. On this site the page is kept under its long-standing “polycystic ovary syndrome” title for familiarity and continuity of inbound links, with this history documenting the rename so the connection is clear.
It is worth stating plainly what the rename is and isn’t. It does not change the underlying biology, the diagnostic features, or the treatments; a person diagnosed with PCOS has the same condition whatever it is called. What it changes is emphasis and accuracy — replacing a label built around a structure that was never truly cystic with one that signals a hormonal and metabolic disorder of the whole body. In that sense the 2026 rename is the natural endpoint of the very history told on this page: each era renamed the condition to match its best current understanding, and this is simply the latest, and arguably most accurate, of those renamings.
Legacy: What the History Teaches
The three-century history of PCOS is unusually instructive because it shows, in miniature, how medicine actually learns. The same condition was seen first as an anatomical oddity (Vallisneri's glistening ovaries, 1721), then as a metabolic curiosity (Achard and Thiers' diabetes of bearded women, 1921), then as a gynecologic syndrome (Stein and Leventhal, 1935), then as an insulin-driven endocrine-metabolic disorder (Burghen and colleagues, 1980), and finally as a multi-system whole-body condition deserving a new name (the 2026 PMOS consensus). Each framing was a real advance, and each was incomplete on its own.
The history also carries a caution about names. “Polycystic ovary syndrome” was a reasonable description in its day, but the single misleading word “cystic” arguably shaped how patients, clinicians, and researchers thought about the disorder for generations — narrowing attention to the ovary when the metabolism, the skin, the cardiovascular system, and mental health were all in play. The decades-long effort to rename it is a reminder that the words medicine chooses are not neutral labels but lenses that can clarify or distort.
For anyone living with this condition today, the practical lesson of its history is hopeful. A disorder that was once treatable only by removing wedges of ovary, with no understanding of its cause, is now approached through a rich toolkit — lifestyle and metabolic management, insulin-sensitizing and ovulation-inducing medications, dermatologic and fertility care, and increasingly individualized treatment — built on a far deeper understanding of the hormones and metabolism involved. The story is still being written; the 2026 rename is the latest chapter, not the last.
Research Papers and References
The references below combine the key primary papers in the history of PCOS with peer-reviewed historical reviews and authoritative resources. Where a stable DOI or PubMed identifier is available it is linked directly; otherwise a curated PubMed topic-search link is provided. Each link opens in a new tab. Historical primary descriptions (Vallisneri, 1721; Achard & Thiers, 1921) are named in the article as historical sources and are documented through the modern review literature cited here.
- Stein IF, Leventhal ML. Amenorrhea associated with bilateral polycystic ovaries. American Journal of Obstetrics and Gynecology. 1935;29(2):181–185. — doi:10.1016/S0002-9378(15)30642-6
- Burghen GA, Givens JR, Kitabchi AE. Correlation of hyperandrogenism with hyperinsulinism in polycystic ovarian disease. The Journal of Clinical Endocrinology & Metabolism. 1980;50(1):113–116. — doi:10.1210/jcem-50-1-113
- The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Fertility and Sterility. 2004;81(1):19–25. — doi:10.1016/j.fertnstert.2003.10.004 · PMID 14711538
- Szydlarska D, Machaj M, Jakimiuk A. History of discovery of polycystic ovary syndrome. Advances in Clinical and Experimental Medicine. 2017;26(3):555–558. — doi:10.17219/acem/61987 · PMID 28791833
- Adashi EY, Cibula D, Peterson M, Azziz R. The polycystic ovary syndrome: the first 150 years of study. F&S Reports. 2023;4(1):2–18. — PMC10028479
- Azziz R, Adashi EY. Stein and Leventhal: 80 years on. American Journal of Obstetrics and Gynecology. 2016;214(2):247.e1–247.e11. — doi:10.1016/j.ajog.2015.12.013 Search PubMed
- Velazquez EM, Mendoza S, Hamer T, Sosa F, Glueck CJ. Metformin therapy in polycystic ovary syndrome reduces hyperinsulinemia, insulin resistance, hyperandrogenemia, and systolic blood pressure, while facilitating normal menses and pregnancy. Metabolism. 1994;43(5):647–654. — doi:10.1016/0026-0495(94)90209-7
- NIH 1990 expert-conference criteria for PCOS (Zawadzki & Dunaif; NICHD-sponsored conference, April 1990) PubMed: NIH 1990 PCOS diagnostic criteria
- Achard-Thiers syndrome — “diabetes of bearded women” (1921) and the history of hyperandrogenism with glucose intolerance PubMed: Achard-Thiers syndrome history
- Polyendocrine Metabolic Ovarian Syndrome (PMOS) — the 2026 global consensus renaming of PCOS PubMed: PMOS renaming consensus
- Laparoscopic ovarian drilling for PCOS (descendant of Stein-Leventhal wedge resection; Gjønnæss, 1984) PubMed: ovarian drilling and wedge resection
- Insulin resistance and PCOS — mechanisms and clinical implications (updated reviews) PubMed: insulin resistance in PCOS
- Diagnostic criteria for PCOS — comparison of NIH 1990, Rotterdam 2003, and AE-PCOS 2006 definitions PubMed: PCOS diagnostic criteria comparison
- History and evolving understanding of polycystic ovary syndrome (Vallisneri to the present) PubMed: PCOS history Vallisneri to present
External Authoritative Resources
- NICHD (U.S. National Institutes of Health) — Polycystic Ovary Syndrome
- Endocrine Society — PCOS / PMOS patient information
- PubMed — All research on polycystic ovary syndrome
Connections
- Polycystic Ovary Syndrome (PCOS)
- Insulin Resistance
- Metabolic Syndrome
- Infertility
- Ovarian Cysts
- Type 2 Diabetes
- All Conditions