SAM-e (S-Adenosylmethionine)
SAM-e (pronounced "sammy," short for S-adenosylmethionine) is a molecule your body makes on its own, around the clock, from the amino acid methionine and the cellular energy carrier ATP. It is not something you eat directly in any meaningful amount — it is manufactured inside your cells and used almost immediately. Its role is unusually central: SAM-e is the body's universal methyl donor, the chemical that hands off a small carbon group needed to build brain chemicals, protect cell membranes, regulate genes, and keep cartilage and the liver healthy. Because it sits at such a busy crossroads, SAM-e became a supplement with a genuinely stronger evidence base than most — there is real, repeatedly-tested support for it in depression, osteoarthritis, and certain liver conditions. It also carries a few real cautions that matter, especially for anyone with bipolar disorder or taking antidepressants. This page explains what SAM-e actually is, the biochemistry in plain language, what the research honestly shows, and how it is used.
Table of Contents
- What SAM-e Is
- SAM-e and the Methylation Cycle
- SAM-e's Three Jobs in the Body
- SAM-e for Depression
- SAM-e for Osteoarthritis (Joint Pain)
- SAM-e for Liver Conditions
- Safety, Warnings & Who Should Be Careful
- Using SAM-e: Forms, Dosing & Practical Tips
- Research Papers
- Connections
- Featured Videos
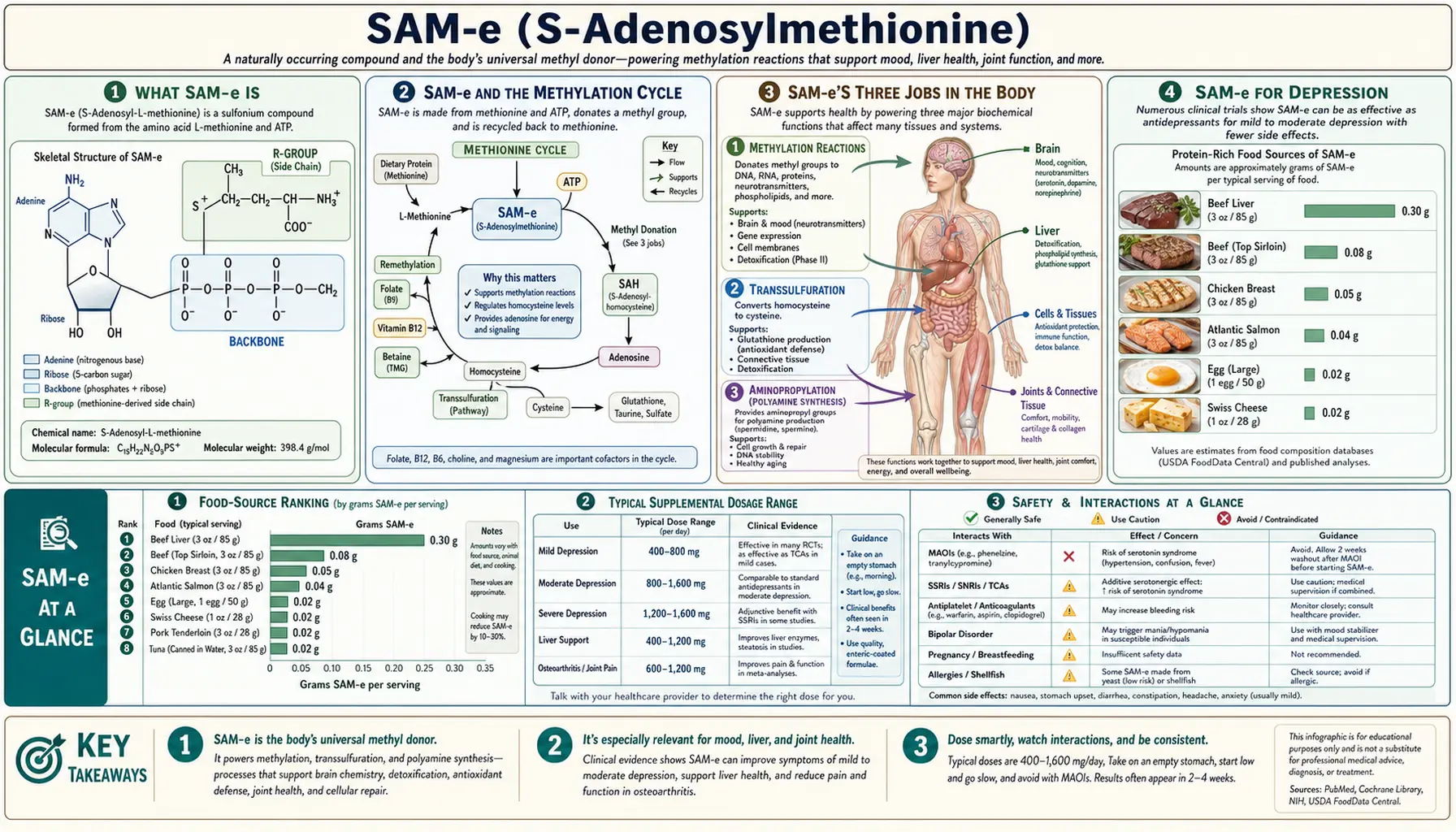
What SAM-e Is
SAM-e is a naturally occurring compound found in every living cell. Chemically, it is methionine — one of the essential amino acids from the protein you eat — joined to adenosine, a piece borrowed from ATP, the molecule cells use to carry energy. That combination is made by an enzyme called methionine adenosyltransferase (MAT). The reaction is expensive: to build one molecule of SAM-e, a cell spends a whole molecule of ATP, which is unusual and tells you how important the product is.
The critical thing to understand is that SAM-e is essentially an internal molecule. Unlike a vitamin or a mineral, you do not get useful amounts of SAM-e from food — it is too unstable to survive digestion in quantity. Your body instead synthesizes all the SAM-e it needs, and it makes a great deal of it: an adult produces and uses several grams of SAM-e every single day, recycling the same building blocks over and over. The liver is the busiest producer, accounting for a large share of the body's total.
What makes SAM-e special is the chemical group it carries: a methyl group — a single carbon atom with three hydrogens attached (–CH₃). SAM-e holds this methyl group in a "high-energy" state, loosely enough that it can be handed off to hundreds of different molecules. Chemists call SAM-e the principal biological methyl donor. When you hear the word "methylation" in nutrition or genetics, SAM-e is almost always the molecule doing the donating. That single job — giving away methyl groups — ripples outward into mood, joint health, liver function, and the switching on and off of genes.
Because the supply of SAM-e depends on the supply of methionine (from dietary protein) and on the B-vitamins that keep the surrounding chemistry running, SAM-e sits at the center of a small, elegant loop that is worth understanding.
SAM-e and the Methylation Cycle
SAM-e is one station on a continuous chemical loop that biochemists call the methylation cycle (or the methionine cycle). Following it once explains most of what SAM-e does and, importantly, why your B-vitamin status matters so much.
The loop runs in four steps:
- Methionine → SAM-e. The amino acid methionine combines with ATP to become SAM-e. SAM-e is now "loaded," carrying its transferable methyl group.
- SAM-e → SAH. SAM-e donates that methyl group to some target molecule — a neurotransmitter, a stretch of DNA, a membrane fat, and so on. Having given away its methyl group, SAM-e becomes S-adenosylhomocysteine, or SAH.
- SAH → homocysteine. SAH is quickly broken down, releasing homocysteine — the same homocysteine measured on some lab panels as a marker of cardiovascular and metabolic health.
- Homocysteine → back to methionine (or onward). Homocysteine can be re-methylated back into methionine, closing the loop so the whole cycle can run again.
That last step is where the B-vitamins come in, and it is the reason a page about an amino-acid-derived molecule keeps mentioning vitamins. To turn homocysteine back into methionine, the body needs a fresh methyl group, which it gets from folate (vitamin B9, in its active 5-methyl-tetrahydrofolate form) using vitamin B12 as an essential helper for the enzyme that does the transfer. A second, backup route uses betaine, a substance the body makes from choline. If folate or B12 run short, homocysteine cannot be efficiently recycled: it builds up, methionine regeneration slows, and the cell's ability to keep making SAM-e can falter.
This interlock is why low B12 or low folate can look, chemically, like a SAM-e problem — and why depression linked to B-vitamin deficiency, high homocysteine, and low SAM-e tend to cluster together in the research. It is also why some clinicians who use SAM-e recommend making sure folate, B12, and vitamin B6 are adequate first, so the cycle has what it needs to keep turning. If you are curious about your own numbers, the homocysteine blood test is the standard window into how well this cycle is running.
SAM-e's Three Jobs in the Body
SAM-e branches into three distinct chemical pathways. Each one is the reason for a specific supplement use, so it is worth taking them one at a time.
1. Methylation — building brain chemicals and membranes
This is SAM-e's headline role and the one behind its use for mood. As the universal methyl donor, SAM-e supplies the methyl group for a long list of reactions, including:
- Neurotransmitters. The making and breaking-down of dopamine, norepinephrine, and serotonin all involve methylation steps that draw on SAM-e. Melatonin, the sleep hormone, is also produced through a SAM-e-dependent methylation. This chemistry is the plausible basis for SAM-e's antidepressant effects.
- Cell membranes. SAM-e helps convert one membrane fat (phosphatidylethanolamine) into another (phosphatidylcholine), which keeps cell membranes fluid and healthy — a process especially important in the liver and in nerve cells.
- Genes (DNA and histones). Adding methyl groups to DNA is one of the main ways the body switches genes on and off without changing the underlying code — the field known as epigenetics. SAM-e is the methyl source for this, linking nutrition to gene regulation.
- Creatine. A large share of the body's daily methylation is spent making creatine for muscle energy, again with SAM-e as the donor.
2. Transsulfuration — making glutathione (antioxidant defense)
The homocysteine produced downstream of SAM-e does not have to loop back to methionine. It can instead be pushed forward down a route called transsulfuration, which converts it (via cystathionine) into the amino acid cysteine. Cysteine is the rate-limiting ingredient for glutathione, the body's master antioxidant and the liver's main tool for neutralizing toxins. This branch requires vitamin B6 as a cofactor. It explains a good part of SAM-e's interest in liver disease: healthy SAM-e levels support glutathione production, and glutathione protects liver cells from oxidative damage.
3. Aminopropylation — polyamines, cartilage, and cell growth
SAM-e has a third, less-famous trick. After being decarboxylated, it can donate a different chemical group (an aminopropyl group) to build molecules called polyamines (spermidine and spermine), which cells need for growth, repair, and DNA stabilization. This pathway is invoked to explain SAM-e's effect on joint cartilage: SAM-e appears to support the cartilage cells (chondrocytes) that manufacture the proteoglycan cushioning of a joint, which is the rationale behind its use in osteoarthritis.
Three jobs, three supplement stories: methylation drives the depression research, transsulfuration underlies the liver work, and aminopropylation supports the osteoarthritis use. All three trace back to the same molecule.
SAM-e for Depression
Depression is SAM-e's most-studied use, and the evidence is genuinely more substantial than for the vast majority of supplements — though it is not without gaps, and honesty requires laying out both sides.
The case in favor. SAM-e has been tested against depression since the 1970s, first in Europe (where an injectable form was used in hospitals) and later as an oral supplement. Across dozens of trials, the general pattern has been that SAM-e outperforms placebo and performs roughly on par with older tricyclic antidepressants, sometimes with a faster onset. Two findings are especially interesting to patients:
- As an add-on to standard antidepressants. A well-designed 2010 randomized trial found that adding SAM-e (800 mg twice daily) to an SSRI in people who had not responded to the SSRI alone produced meaningfully higher response and remission rates than adding a placebo. This "augmentation" use — SAM-e alongside a prescription antidepressant, under a doctor's supervision — is one of its most practical and best-supported applications.
- As a stand-alone option. Some head-to-head trials have compared SAM-e directly with prescription antidepressants such as escitalopram, generally finding it in the same ballpark, which is why clinician-oriented reviews list it as a reasonable option for people who cannot tolerate conventional drugs.
The honest caveats. A 2016 Cochrane systematic review — the most rigorous kind — concluded that while SAM-e did not appear clearly worse than standard antidepressants, the overall evidence base was still limited in quality and quantity, with trials that were often small, short, or industry-linked, and it called for larger, better studies before firm conclusions could be drawn. In other words: promising and plausible, backed by real biochemistry and multiple positive trials, but not yet the ironclad, replicated evidence a prescription drug must clear. SAM-e also acts as an activating antidepressant, which is central to its most important safety warning (see Safety).
The practical takeaway most reviewers reach is measured: SAM-e is a reasonable, evidence-supported option for depression — particularly as a physician-supervised add-on to an antidepressant, or for someone who cannot tolerate standard drugs — but it should be used as part of a real treatment plan, not as a casual self-prescription for serious depression.
SAM-e for Osteoarthritis (Joint Pain)
The second well-studied use is osteoarthritis, the common "wear-and-tear" arthritis in which the cartilage cushioning a joint gradually breaks down, causing pain and stiffness in knees, hips, and hands.
The case in favor. Beginning in the 1980s, a series of clinical trials compared SAM-e head-to-head with anti-inflammatory painkillers (NSAIDs) such as ibuprofen, naproxen, and celecoxib. The recurring result was striking: SAM-e produced pain relief and functional improvement comparable to the NSAIDs, but with noticeably fewer side effects — particularly fewer of the stomach and gut problems that limit long-term NSAID use. A 2004 double-blind trial comparing SAM-e (1,200 mg/day) with celecoxib captured the trade-off nicely: celecoxib relieved pain faster in the first month, but by the second month SAM-e had caught up and the two were equally effective. That points to SAM-e's main practical drawback for joints: a slower onset. It is not a fast painkiller — benefits typically build over several weeks — so it suits chronic, ongoing joint pain rather than acute flare-ups.
The mechanism fits: through its aminopropylation pathway, SAM-e appears to support the cartilage-making chondrocytes and may have mild anti-inflammatory effects of its own.
The honest caveats. A 2009 Cochrane review looked critically at the osteoarthritis trials and found that only a handful met its strict quality bar. On that narrower, higher-standard basis, the reviewers judged the evidence inconclusive — not because the trials were negative, but because the well-controlled ones were small, potentially biased, and too few to be certain the benefit is real and clinically meaningful. So the fair summary is: multiple individual trials are encouraging and SAM-e's tolerability advantage over NSAIDs is a genuine attraction, but the top-tier evidence remains thinner than the number of positive studies might suggest. It is a reasonable thing to try for chronic osteoarthritis pain — with patience for its slow onset and realistic expectations.
SAM-e for Liver Conditions
SAM-e's third evidence area is the liver — fitting, because the liver is where the body makes most of its SAM-e in the first place. In several chronic liver diseases, the enzyme that produces SAM-e works poorly, so liver SAM-e levels drop, which in turn starves the liver of the glutathione it needs to protect itself. Restoring SAM-e is therefore a logical therapy, and in a number of countries (notably in parts of Europe and Asia) prescription SAM-e — sometimes given by injection — is used clinically for liver problems.
The clearest use is intrahepatic cholestasis, a condition in which bile flow within the liver slows or stalls, causing bile components to back up into the bloodstream (bringing itching, jaundice, and abnormal liver tests). This includes intrahepatic cholestasis of pregnancy (ICP), a distressing late-pregnancy condition of intense itching and elevated bile acids. SAM-e has been used, often alongside the better-established drug ursodeoxycholic acid, to try to improve bile flow and relieve symptoms. Reviews and meta-analyses suggest SAM-e can improve some biochemical markers (such as bilirubin and liver enzymes) in cholestatic liver disease.
The honest caveats. Two limits are important. First, the quality of the evidence is modest: a 2015 meta-analysis of SAM-e in chronic liver disease noted improvements in certain markers but flagged the small size and variable quality of the trials, and a 2012 clinical review reached a similar "biologically plausible, some benefit, but robust randomized evidence still limited" conclusion. Second, for cholestasis of pregnancy specifically, Cochrane's assessment of the various treatments found ursodeoxycholic acid to be the better-studied first choice, with SAM-e's role more of an adjunct. The bottom line: SAM-e is a recognized, clinically-used liver therapy in some countries with a sound rationale, but it is not a do-it-yourself treatment for liver disease. Liver conditions — and anything in pregnancy — require medical supervision, and SAM-e here belongs in a doctor's hands, not a self-care routine.
Safety, Warnings & Who Should Be Careful
SAM-e is generally well tolerated by most people, and it has a long track record. Most side effects are mild and dose-related. But it carries two warnings that are genuinely important, and those deserve top billing.
The bipolar warning (most important)
Because SAM-e acts as an activating antidepressant, it can push mood upward — and in a person with bipolar disorder, that upward push can tip into mania or hypomania (a dangerous, over-elevated, agitated, sleepless, impulsive state). There are documented reports of exactly this. Anyone with bipolar disorder, or a strong family history of it, should not take SAM-e except under the supervision of a psychiatrist. This is the single most important cautionary point about SAM-e.
Serotonin syndrome (with antidepressants)
Because SAM-e influences serotonin-related chemistry, combining it with medications that also raise serotonin — SSRIs, SNRIs, MAOIs, tramadol, triptan migraine drugs, or St. John's Wort — carries a theoretical risk of serotonin syndrome, a potentially serious reaction of agitation, rapid heartbeat, high temperature, tremor, and confusion. In the depression-augmentation trials, SAM-e was combined with SSRIs safely under close medical supervision, so the combination is not automatically off-limits — but it should only be done with a doctor's knowledge and monitoring, never as a casual pairing you arrange yourself.
Common side effects and other cautions
- Digestive upset — nausea, gas, diarrhea, or an upset stomach, especially when starting or at higher doses.
- Insomnia, restlessness, anxiety, or headache — a consequence of SAM-e being activating. Taking it in the morning (not the evening) helps avoid sleep problems.
- Homocysteine. SAM-e metabolism generates homocysteine as a by-product. To keep that recycled efficiently, make sure folate, B12, and B6 are adequate; some clinicians pair SAM-e with a B-complex for this reason.
- Parkinson's disease. People taking levodopa should be cautious, as SAM-e's methylation activity could theoretically interfere with the drug — discuss with a neurologist.
- Pregnancy and breastfeeding. Although prescription SAM-e is used medically for cholestasis of pregnancy in some countries, that is a supervised clinical decision. General over-the-counter use during pregnancy or breastfeeding should only happen with a doctor's guidance.
- Surgery. Because of its effects on the nervous system, it is sensible to stop SAM-e a couple of weeks before scheduled surgery and tell your anesthesiologist.
None of this makes SAM-e a dangerous molecule — for a healthy person without bipolar disorder and not on serotonergic drugs, it is one of the better-tolerated supplements. But the bipolar and antidepressant-interaction points are real, not boilerplate, and they are the reason SAM-e is best used with a clinician in the loop.
Using SAM-e: Forms, Dosing & Practical Tips
SAM-e has a few real-world quirks that separate a good product and routine from a wasted one.
Stability and enteric coating
SAM-e is a chemically unstable molecule — it degrades with exposure to heat, moisture, and air, and it breaks down in stomach acid. Two practical consequences follow. First, always buy enteric-coated tablets (coated to survive the stomach and dissolve in the intestine, where SAM-e is absorbed); loose powder or cheap uncoated tablets can be largely useless by the time they reach you. Second, freshness and packaging matter: look for individually sealed blister packs rather than a big open bottle, check dates, and store it somewhere cool and dry. The more stable salt forms (SAM-e is usually sold as the "butanedisulfonate" or "tosylate" salt) hold up better. This instability is also part of why SAM-e is relatively expensive compared with everyday supplements — a genuine downside worth budgeting for, since effective doses are not small.
Take it on an empty stomach
SAM-e is absorbed best on an empty stomach — typically 30–60 minutes before a meal. Taking it with food can blunt absorption. The trade-off is that an empty stomach can worsen nausea in sensitive people; if that happens, a small titration (see below) usually helps more than taking it with food.
Typical dosing ranges
Doses in the research vary by use. These are the general ranges reported in studies, not a personal prescription — the right dose and whether to use SAM-e at all should be decided with a clinician, especially given the warnings above:
- Depression: commonly 800–1,600 mg per day, usually split into two doses (for example, the 800 mg-twice-daily regimen used in the SSRI-augmentation trial).
- Osteoarthritis: commonly 600–1,200 mg per day, with benefits building over several weeks rather than days.
- Liver conditions: higher doses are used clinically, but this is a supervised medical setting (sometimes intravenous), not a self-care dose.
Start low and build up. A widely used approach is to begin at the lower end (or even 200–400 mg) for the first several days and increase gradually. This "titration" reduces the nausea, anxiety, and jitteriness that a full dose can cause out of the gate, and it lets you find the lowest amount that works. Because SAM-e is activating, take the day's dose — or the larger share of a split dose — in the morning to protect your sleep. Give depression a couple of weeks and joints several weeks before judging whether it is helping.
Research Papers
- Lu SC. S-Adenosylmethionine. The International Journal of Biochemistry & Cell Biology. 2000;32(4):391–395. doi:10.1016/S1357-2725(99)00139-9 — A concise overview of SAM-e as the body's principal methyl donor and its central place in methylation, transsulfuration, and aminopropylation.
- Bottiglieri T. S-Adenosyl-L-methionine (SAMe): from the bench to the bedside — molecular basis of a pleiotropic molecule. The American Journal of Clinical Nutrition. 2002;76(5):1151S–1157S. doi:10.1093/ajcn/76.5.1151S — A foundational review connecting SAM-e biochemistry to its clinical uses in mood, liver, and joints.
- Selhub J. Homocysteine metabolism. Annual Review of Nutrition. 1999;19(1):217–246. doi:10.1146/annurev.nutr.19.1.217 — The classic account of the methionine/homocysteine cycle, explaining why folate, B12, and B6 status governs SAM-e regeneration.
- Papakostas GI, Mischoulon D, Shyu I, Alpert JE, Fava M. S-adenosyl methionine (SAMe) augmentation of serotonin reuptake inhibitors for antidepressant nonresponders with major depressive disorder: a double-blind, randomized clinical trial. American Journal of Psychiatry. 2010;167(8):942–948. doi:10.1176/appi.ajp.2009.09081198 — The key trial showing SAM-e added to an SSRI improved response and remission in people who had not responded to the SSRI alone.
- Sarris J, Papakostas GI, Vitolo O, Fava M, Mischoulon D. S-adenosyl methionine (SAMe) versus escitalopram and placebo in major depression RCT: efficacy and effects of histamine and carnitine as moderators of response. Journal of Affective Disorders. 2014;164:76–81. doi:10.1016/j.jad.2014.03.041 — A head-to-head randomized comparison of SAM-e against a standard antidepressant and placebo.
- Galizia I, Oldani L, Macritchie K, et al. S-adenosyl methionine (SAMe) for depression in adults. Cochrane Database of Systematic Reviews. 2016;(10):CD011286. doi:10.1002/14651858.CD011286.pub2 — The rigorous systematic review; found SAM-e not clearly inferior to antidepressants but the evidence base still limited, calling for larger trials.
- Sharma A, Gerbarg P, Bottiglieri T, et al. S-Adenosylmethionine (SAMe) for neuropsychiatric disorders: a clinician-oriented review of research. The Journal of Clinical Psychiatry. 2017;78(6):e656–e667. doi:10.4088/JCP.16r11113 — A practical review summarizing the mood evidence and safety considerations for clinicians.
- Rutjes AWS, Nüesch E, Reichenbach S, Jüni P. S-Adenosylmethionine for osteoarthritis of the knee or hip. Cochrane Database of Systematic Reviews. 2009;(4):CD007321. doi:10.1002/14651858.CD007321.pub2 — The cautious systematic review that judged the higher-quality osteoarthritis trials too small and few to be conclusive.
- Najm WI, Reinsch S, Hoehler F, Tobis JS, Harvey PW. S-adenosyl methionine (SAMe) versus celecoxib for the treatment of osteoarthritis symptoms: a double-blind cross-over trial. BMC Musculoskeletal Disorders. 2004;5:6. doi:10.1186/1471-2474-5-6 — The trial showing SAM-e matched celecoxib for joint pain by the second month, with a slower onset.
- Anstee QM, Day CP. S-adenosylmethionine (SAMe) therapy in liver disease: a review of current evidence and clinical utility. Journal of Hepatology. 2012;57(5):1097–1109. doi:10.1016/j.jhep.2012.04.041 — A clinical review of SAM-e in liver disease: plausible mechanism and some benefit, but robust randomized evidence still limited.
- Guo T, Chang L, Xiao Y, Liu Q. S-adenosyl-L-methionine for the treatment of chronic liver disease: a systematic review and meta-analysis. PLOS ONE. 2015;10(3):e0122124. doi:10.1371/journal.pone.0122124 — A meta-analysis reporting improvements in some liver markers with SAM-e while flagging the modest quality of the trials.
- Gurung V, Stokes M, Middleton P, Milan SJ, Hague W, Thornton JG. Interventions for treating cholestasis in pregnancy. Cochrane Database of Systematic Reviews. 2013;(6):CD000493. doi:10.1002/14651858.CD000493.pub2 — The systematic review of treatments for intrahepatic cholestasis of pregnancy, placing SAM-e as an adjunct to better-studied ursodeoxycholic acid.
Connections
- Methionine
- Choline
- Vitamin B12
- Folate (Vitamin B9)
- Vitamin B6
- Cysteine
- Homocysteine Test
- All Amino Acids