Meditation
Meditation is a family of mental-training practices in which you deliberately and repeatedly steady your attention — usually on the breath, a word, a sensation, or an attitude like kindness — and gently return to it each time your mind wanders. It is one of the most-studied mind–body practices, but the evidence is uneven. The strongest, most consistent findings are for anxiety, depression, and chronic pain, where well-conducted reviews show real but modest benefits — roughly on the order of what you might get from many other active self-care approaches, not a cure. A landmark 2014 review in JAMA Internal Medicine found moderate-quality evidence that mindfulness programs reduce anxiety, depression, and pain, but only low or insufficient evidence that they improve mood, attention, sleep, eating, or weight. Meditation is also recognized by the American Heart Association as a reasonable add-on (not a replacement) for cardiovascular risk reduction, with small blood-pressure benefits. It is generally very safe, inexpensive, and something you can start today — while understanding that it is a complement to, not a substitute for, treatment of serious illness.
Interactive Visualization The Stress Response — fire a stressor and watch cortisol rise Adrenaline spikes in a second, cortisol follows in minutes — then compare acute stress with chronic, and watch the feedback loop blunt. Launch →
Table of Contents
- What Meditation Actually Is
- The Main Types — and Which to Try
- Stress & Anxiety
- Blood Pressure & Heart
- Depression & Pain
- Brain, Attention & Aging
- How to Start (No App Required)
- Cautions & Realistic Expectations
- Key Research Papers
- Connections
- Featured Videos
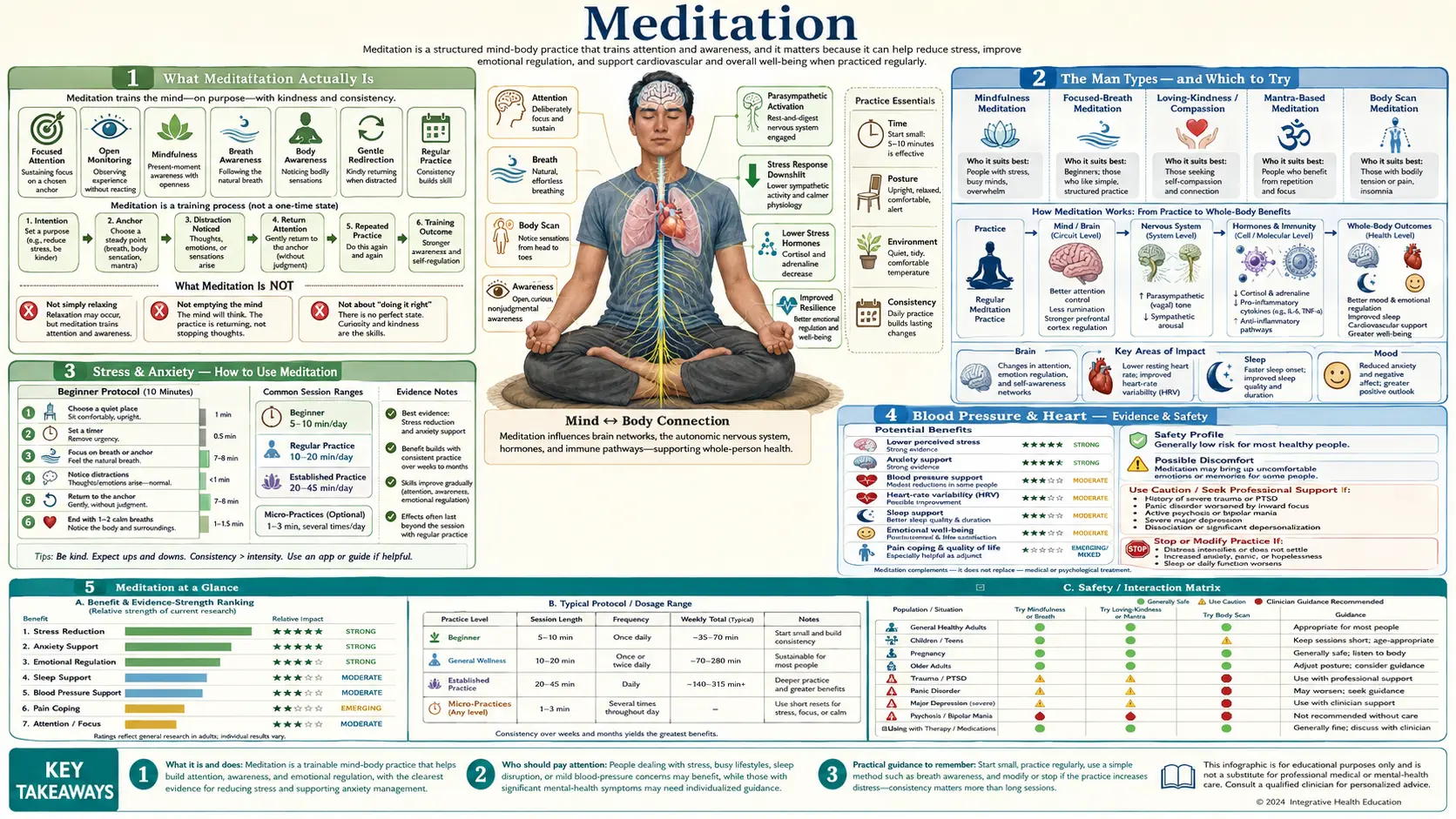
What Meditation Actually Is
Meditation is not one thing. It is an umbrella term for practices that train attention and awareness, usually to produce a calmer, clearer, or more stable state of mind. The common thread is simple: you choose something to pay attention to, you notice when your mind drifts (it always does), and you bring it back — over and over. That “noticing and returning” is the practice. It is a bit like reps at the gym for your attention.
Two myths are worth clearing up right away. First, meditation is not about emptying your mind or stopping all thoughts. A wandering mind is not failure; noticing the wandering and gently returning is the entire skill. People who quit because they “can’t stop thinking” have usually misunderstood the goal. Second, meditation does not require any religion or belief system. Although many techniques have roots in Buddhist, Hindu, and other contemplative traditions, the forms studied in clinics — especially mindfulness-based programs — are taught in entirely secular, skills-based ways in hospitals, schools, and workplaces.
The main families you will encounter are:
- Mindfulness / MBSR: paying open, non-judgmental attention to whatever is happening right now — breath, body, sounds, thoughts — without trying to change it. The best-known structured version is Mindfulness-Based Stress Reduction (MBSR), an 8-week course developed by Jon Kabat-Zinn at the University of Massachusetts in the late 1970s.
- Focused-attention: resting attention on a single anchor (often the breath) and returning to it whenever you drift. This is the foundation most beginners start with.
- Loving-kindness / compassion: deliberately generating goodwill toward yourself and others, often by silently repeating phrases like “may you be well, may you be at ease.”
- Mantra / Transcendental Meditation (TM): silently repeating a word or sound to settle the mind. TM is a specific trademarked program; generic mantra meditation is free and unbranded.
- Body scan: moving attention slowly through the body, part by part, noticing sensations without judging them. It is a core component of MBSR and a gentle entry point for people who find breath-focus difficult.
The Main Types — and Which to Try
There is no single “best” meditation; the right one is the one you will actually do. Here is a practical map of what each type tends to be good for, so you can pick a starting point rather than agonize over the “correct” method.
- Breath-focused (focused-attention) — best first stop for almost everyone. Simple, portable, nothing to buy. Good for general stress, building the basic “return your attention” skill, and for short daily sessions.
- Mindfulness / MBSR — best for stress, anxiety, and reactivity. The structured 8-week MBSR course is the most heavily researched format. Good if you want a guided, time-limited program with a teacher and a clear curriculum.
- Body scan — best for chronic pain, tension, and people who can’t sit still. Lying down is fine. Helps you relate differently to physical sensations rather than fighting them.
- Loving-kindness / compassion — best for harsh self-criticism, loneliness, irritability, or burnout. Useful when the problem is less “racing mind” and more “being hard on yourself.”
- Mantra / TM — best for people who find a repeated word easier than watching the breath. You do not need to pay for a branded program to get the core benefit; any neutral word repeated silently works.
A reasonable plan: start with 5–10 minutes of breath focus daily. If you crave more structure, take a secular MBSR course (many are free or low-cost through hospitals and community centers). If self-criticism or stress about a health condition is the main issue, add a few minutes of loving-kindness or a body scan. Switching styles is fine — consistency matters far more than picking the “perfect” technique.
Stress & Anxiety
This is meditation’s strongest evidence area, and it is where you can be most confident the benefit is real — while keeping expectations honest. The most rigorous synthesis is the 2014 JAMA Internal Medicine review by Goyal and colleagues, which pooled 47 randomized trials with over 3,500 participants and graded the quality of the evidence. Comparing mindfulness programs against an active control (so that ordinary attention and the placebo of “doing something” were accounted for), they found moderate-quality evidence of benefit for anxiety, with an effect size of about 0.38 at 8 weeks (95% CI 0.12–0.64), tapering to roughly 0.22 at 3–6 months. For depressive symptoms the effect was about 0.30 at 8 weeks.
What does an effect size near 0.3–0.4 mean in plain terms? It is a small-to-moderate effect — noticeable and worthwhile for many people, but not dramatic, and broadly comparable to other active self-management approaches. Importantly, the same review found no evidence that meditation was superior to other active treatments such as medication, exercise, or other behavioral therapies. So the fair summary is: meditation reliably helps with stress and anxiety to a modest degree, and it is a legitimate option — not a uniquely powerful one.
The most-studied delivery vehicle is MBSR, the 8-week mindfulness course. A separate, broader 2010 meta-analysis (Hofmann and colleagues, 39 studies) reported larger effects for anxiety and mood in clinical populations, though that analysis included less-controlled study designs, which tends to inflate apparent benefits. Taken together, the picture is encouraging but should be stated carefully: for everyday stress and clinical anxiety, mindfulness helps a moderate amount, and the better-controlled the study, the more modest the effect tends to look.
Blood Pressure & Heart
Meditation has crossed into mainstream cardiology, but with deliberately cautious wording. In 2017 the American Heart Association issued a scientific statement (Levine and colleagues) reviewing the evidence and concluded that meditation “may be considered as an adjunct” to standard, guideline-directed care — meaning it sits alongside, never instead of, proven treatments like blood-pressure medication, a heart-healthy diet, exercise, not smoking, and cholesterol management.
On blood pressure specifically, some forms of meditation are associated with small reductions — on the order of a few millimeters of mercury in various trials — but the AHA was explicit that the studies are often small, short, and of modest quality, so the certainty is limited. The honest framing matters here: if you have high blood pressure, meditation may help a little and is very unlikely to hurt, but it is not a replacement for prescribed antihypertensive treatment, and you should not stop or reduce medication based on a meditation practice. Think of it as a low-risk supporting player in a broader heart-health plan, not a primary therapy.
Depression & Pain
Two of the most practically useful findings concern preventing depression from coming back and living with chronic pain.
Preventing depression relapse (MBCT)
For people who have had repeated episodes of major depression, a specialized program called Mindfulness-Based Cognitive Therapy (MBCT) — mindfulness skills combined with cognitive-therapy tools — has solid evidence for relapse prevention. A 2016 individual-patient-data meta-analysis in JAMA Psychiatry by Kuyken and colleagues pooled 9 randomized trials with 1,258 patients and found that MBCT reduced the risk of relapse over 60 weeks, with a hazard ratio of 0.69 (95% CI 0.58–0.82) versus no MBCT. Compared specifically against active treatments — a group that included maintenance antidepressants — MBCT still showed a modest edge (hazard ratio 0.79, 95% CI 0.64–0.97). In plain language: for people with recurrent depression, MBCT is at least as effective as staying on maintenance antidepressants for preventing the next episode, which makes it a real, evidence-based alternative for those who prefer not to stay on medication indefinitely. (This is about preventing relapse in people who have recovered — not about treating an active, severe episode.)
Chronic pain
For ongoing pain, mindfulness can help — modestly. A 2017 systematic review (Hilton and colleagues, 38 randomized trials) found that mindfulness meditation was associated with a small reduction in pain and improvements in depression and quality of life, but rated the evidence as low quality, calling for larger, better-designed trials. The realistic takeaway: meditation is unlikely to make chronic pain vanish, but it can change your relationship to pain — reducing the distress, fear, and tension that amplify it — and that shift is genuinely valuable for many people living with persistent pain.
Brain, Attention & Aging
You will often read that meditation “rewires your brain” or “grows gray matter.” There is some real science here, but it is the area most prone to hype, so it deserves careful wording. A widely cited 2011 study (Hölzel and colleagues) used MRI before and after an 8-week MBSR course and reported increases in gray-matter density in regions tied to learning, memory, and emotion regulation, including the hippocampus. Other studies have linked long-term meditation to differences in brain structure and to better-preserved attention with age.
Two honest caveats are essential. First, many of these neuroimaging studies are small, preliminary, and often correlational — long-term meditators may differ from non-meditators for many reasons, so “meditators’ brains look different” does not prove meditation caused the difference. Second, when it comes to everyday cognitive benefits, the well-controlled 2014 JAMA Internal Medicine review actually found low or insufficient evidence that meditation programs improve attention. So the careful statement is: there are intriguing, biologically plausible signals that meditation can affect brain structure and attention, but the evidence is early and far less settled than popular headlines suggest. It is a reasonable hope, not an established fact.
How to Start (No App Required)
You do not need an app, a subscription, a cushion, or any special equipment. Here is a complete beginner practice you can do right now:
- Sit comfortably in a chair, feet flat, back reasonably upright but not rigid. You can close your eyes or soften your gaze downward.
- Set a timer for 5–10 minutes. Short and regular beats long and rare.
- Bring your attention to your breath — the feeling of air at your nostrils, or your belly rising and falling. Don’t control it; just feel it.
- When your mind wanders (it will, constantly), simply notice “thinking,” and gently return to the breath. This returning is the exercise — you are not doing it wrong.
- When the timer ends, stop. Notice how you feel, without grading your performance.
The single most important principle is consistency over duration. Ten minutes a day, most days, will do far more than an occasional hour. Anchor it to an existing habit — right after you wake up, or before bed — so it becomes automatic.
For free, high-quality resources, look for guided practices from academic and nonprofit sources: the UCLA Mindful Awareness Research Center offers free guided meditations, the U.S. National Center for Complementary and Integrative Health (NCCIH) publishes plain-language guides, and many hospitals and libraries offer free or low-cost MBSR courses. Paid apps (Headspace, Calm, Insight Timer, and others) can be helpful for structure and reminders, but they are entirely optional — nothing in the research suggests you need to pay to get the benefit.
Cautions & Realistic Expectations
For most people, meditation is very safe — about as low-risk as a self-care practice gets. But “safe” is not the same as “harmless for everyone,” and the field has historically under-reported difficulties. A 2021 U.S. population-based study (Britton and colleagues) found that while unpleasant or challenging meditation experiences were common and usually transient, lasting negative effects occurred in roughly 6–14% of meditators, and were linked to signs of over-arousal or dissociation. These “meditation-related difficulties” — which can include increased anxiety, intrusive emotions, distressing memories, or feelings of detachment — appear more likely with intensive practice (long silent retreats), large amounts of meditation, and a history of trauma or childhood adversity.
Practical guidance:
- Start gently and modestly — short daily sessions, not multi-day intensive retreats, especially if you are new or have a trauma history.
- If meditation consistently makes you feel worse — more anxious, dissociated, or distressed — that is a signal to stop, switch techniques (e.g., open-eyed or movement-based practices), or work with a qualified, trauma-informed teacher or clinician.
- Meditation is not a substitute for treatment of serious mental illness. For significant depression, anxiety disorders, PTSD, bipolar disorder, psychosis, or active suicidal thoughts, it should be used — if at all — alongside professional care, never instead of it. Do not stop prescribed medication or therapy in favor of meditation without your clinician’s involvement.
Finally, set realistic expectations. Meditation is a skill that develops slowly, and the proven benefits for stress, anxiety, depression, and pain are modest, not miraculous. A thoughtful 2018 review titled “Mind the Hype” (Van Dam and colleagues) cautioned that overblown claims and weak studies can leave people “harmed, misled, and disappointed.” The healthiest mindset is curiosity without pressure: try it consistently for a few weeks, judge it by how you feel, and treat it as one useful tool among many — not a guaranteed fix.
Key Research Papers
- Goyal M, Singh S, Sibinga EMS, et al. (2014). Meditation Programs for Psychological Stress and Well-being: A Systematic Review and Meta-analysis. JAMA Internal Medicine, 174(3), 357–368. — The most rigorous review: moderate-quality evidence for anxiety, depression, and pain (effect sizes ~0.3–0.4); low or insufficient evidence for mood, attention, sleep, and weight; no proof of superiority over other active treatments.
- Kuyken W, Warren FC, Taylor RS, et al. (2016). Efficacy of Mindfulness-Based Cognitive Therapy in Prevention of Depressive Relapse: An Individual Patient Data Meta-analysis From Randomized Trials. JAMA Psychiatry, 73(6), 565–574. — In 9 trials (1,258 patients), MBCT cut depression-relapse risk (HR 0.69 vs. no MBCT) and was at least as effective as maintenance antidepressants (HR 0.79).
- Levine GN, Lange RA, Bairey-Merz CN, et al. (2017). Meditation and Cardiovascular Risk Reduction: A Scientific Statement From the American Heart Association. Journal of the American Heart Association, 6(10), e002218. — Meditation “may be considered as an adjunct” to guideline-directed cardiac care, with small blood-pressure benefits but modest-quality evidence.
- Hilton L, Hempel S, Ewing BA, et al. (2017). Mindfulness Meditation for Chronic Pain: Systematic Review and Meta-analysis. Annals of Behavioral Medicine, 51(2), 199–213. — Across 38 trials, mindfulness produced a small reduction in chronic pain and better quality of life, but the evidence was rated low-quality.
- Hofmann SG, Sawyer AT, Witt AA, Oh D (2010). The Effect of Mindfulness-Based Therapy on Anxiety and Depression: A Meta-Analytic Review. Journal of Consulting and Clinical Psychology, 78(2), 169–183. — Across 39 studies, mindfulness-based therapy showed robust effects on anxiety and mood, especially in clinical populations (though with less-controlled designs than the JAMA review).
- Hölzel BK, Carmody J, Vangel M, et al. (2011). Mindfulness Practice Leads to Increases in Regional Brain Gray Matter Density. Psychiatry Research: Neuroimaging, 191(1), 36–43. — An 8-week MBSR course was associated with MRI-detected gray-matter changes in the hippocampus and other regions — intriguing but small and preliminary.
- Van Dam NT, van Vugt MK, Vago DR, et al. (2018). Mind the Hype: A Critical Evaluation and Prescriptive Agenda for Research on Mindfulness and Meditation. Perspectives on Psychological Science, 13(1), 36–61. — A sober, expert caution that hype and weak methodology have outpaced the evidence, and that possible adverse effects deserve real attention.
Connections
- All Remedies
- The Stress Response & Cortisol — interactive animation
- Breathwork
- Natural Anxiety Relief
- Mediterranean Diet
- Fasting
- The Gut-Brain Axis
- Longevity Protocols