C-Peptide Test
The C-peptide test is one of the most useful blood tests in all of diabetes and blood-sugar medicine, yet most people have never heard of it. Its quiet superpower is simple: it measures how much insulin your own body is making, and it does this even in someone who takes insulin by injection. That single fact makes C-peptide the go-to test for questions that ordinary insulin and glucose measurements cannot answer — is this type 1 or type 2 diabetes? Why is this person's blood sugar dropping dangerously low? How much insulin-making capacity is left in the pancreas? This page explains, in plain language, what C-peptide is, why a doctor orders it, how to read the results, and what can throw the number off.
Table of Contents
- What C-Peptide Is
- Why the Test Is Ordered
- Type 1 vs. Type 2 (and LADA, MODY)
- Investigating Low Blood Sugar
- Assessing Beta-Cell Reserve
- Reference Ranges & What Results Mean
- Factors That Affect the Result
- How the Test Is Done & How to Prepare
- Research Papers
- Connections
- Featured Videos
What C-Peptide Is
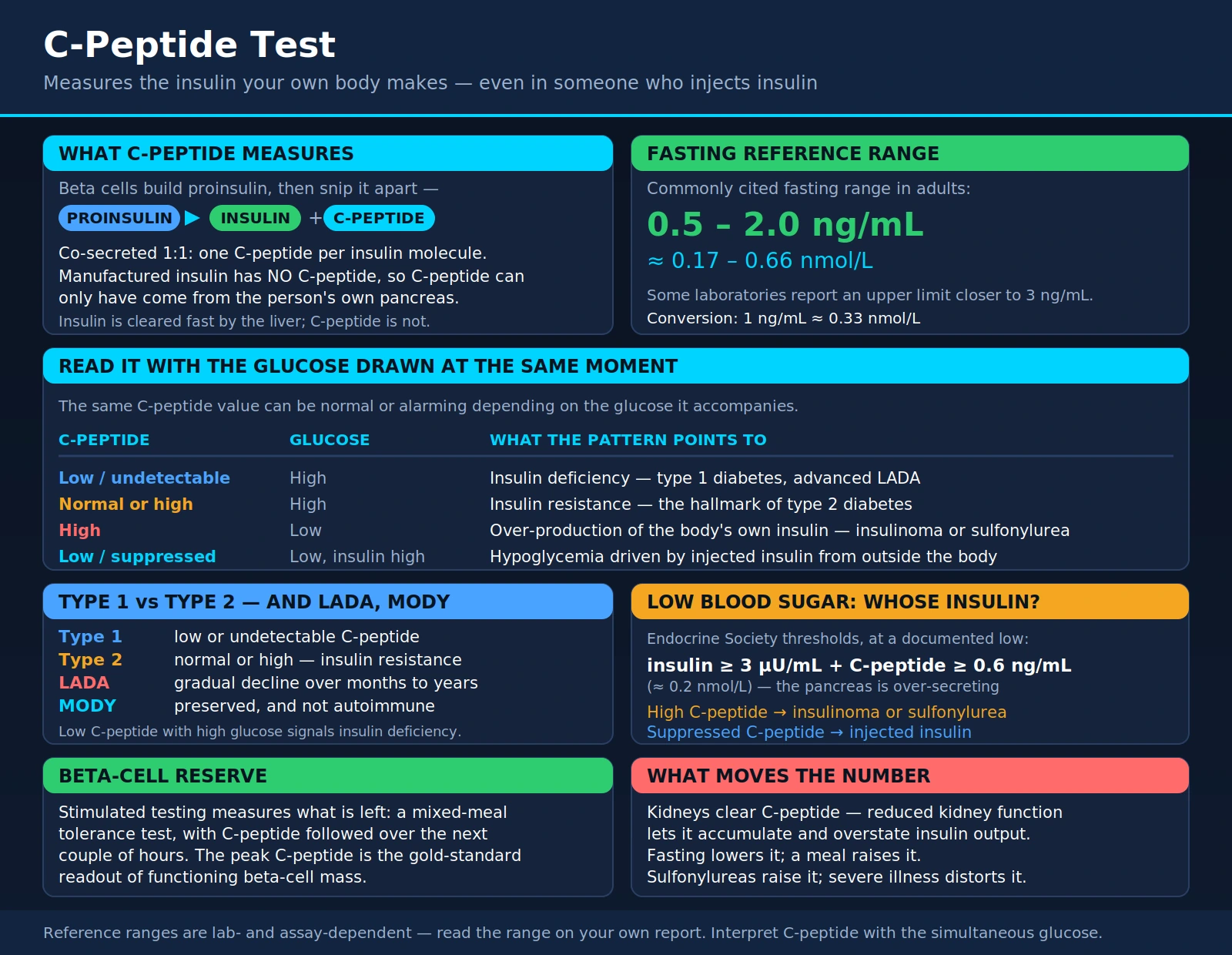
To understand C-peptide, picture how the pancreas actually builds insulin. The insulin-making beta cells first manufacture a larger, inactive precursor molecule called proinsulin. Think of proinsulin as a folded chain with a bridging segment in the middle. When the cell is ready to release insulin, an enzyme snips that chain apart. What comes out are two pieces: the finished insulin molecule, and the bridging segment that had been holding it together — the connecting peptide, or C-peptide.
Here is the crucial part. Because insulin and C-peptide start life joined in the same proinsulin molecule and are cut apart at the same moment, they are released into the bloodstream in equal amounts. For every insulin molecule the pancreas secretes, it also releases one C-peptide molecule. This is what scientists mean when they say the two are co-secreted in a 1:1 ratio. Measure the C-peptide and you have a faithful mirror of how much insulin the body itself produced.
Why not just measure the insulin directly? Two reasons make C-peptide the better witness:
- Injected insulin does not contain C-peptide. Manufactured insulin used for injections is the insulin molecule alone — it has no connecting peptide attached. So in a person who takes insulin, a blood insulin measurement is a jumble of their own insulin plus the injected drug. C-peptide sidesteps this completely: it can only have come from the person's own pancreas. This is the single most important reason the test exists.
- C-peptide lasts longer and is steadier in the blood. The liver pulls a large, variable fraction of insulin out of circulation almost immediately after it is released. C-peptide is not cleared this way and lingers longer, so its level is a more stable, less "spiky" readout of average insulin secretion.
C-peptide itself was long thought to be simply biological packaging with no job of its own once it was cut loose. That view is being revisited — researchers are studying whether C-peptide has subtle effects of its own on nerves and small blood vessels — but for everyday medicine, its value is as a marker: a reliable stand-in for the body's own insulin output.
Why the Test Is Ordered
A doctor does not order a C-peptide test as part of a routine checkup. It is a targeted test, requested to answer a specific question about how much insulin someone is making. The common reasons fall into three groups, each explored in its own section below:
- Classifying diabetes. When it is unclear whether someone has type 1 diabetes (little or no insulin production) or type 2 diabetes (insulin resistance with preserved, often high, production), C-peptide helps sort it out — along with the less common LADA and MODY forms. See Type 1 vs. Type 2.
- Explaining unexplained low blood sugar. When someone has episodes of dangerously low blood sugar (hypoglycemia) without an obvious cause, C-peptide is central to figuring out whether their own pancreas is over-producing insulin (for example, a rare insulin-secreting tumor called an insulinoma) or whether insulin is coming from an injection. See Investigating Low Blood Sugar.
- Measuring remaining pancreas capacity. In people who already have diabetes, C-peptide gauges how much insulin-making "reserve" is left in the beta cells — useful for guiding treatment decisions and for research into therapies that try to preserve that reserve. See Assessing Beta-Cell Reserve.
Less commonly, C-peptide is used to check pancreas function after surgery to remove part of the pancreas, or to help evaluate why a person is not responding as expected to diabetes medication. In all of these situations, the test earns its place because it answers a question that glucose and A1c alone cannot.
Type 1 vs. Type 2 (and LADA, MODY)
Sorting out which kind of diabetes a person has is usually straightforward from the story — a thin child with rapid weight loss and ketones is almost certainly type 1; a middle-aged adult with obesity and gradual onset is usually type 2. But real patients are often ambiguous: adults can develop type 1, people with type 1 can also carry extra weight, and some inherited forms mimic both. When the diagnosis is genuinely uncertain, C-peptide is one of the best tests available to clarify it, because the two main types differ fundamentally in insulin production.
Type 1 diabetes: low or undetectable C-peptide
In type 1 diabetes, the immune system destroys the insulin-producing beta cells. Over time the pancreas can make little or no insulin, so the C-peptide level is low or undetectable — especially when the blood sugar is high at the same time, which should normally be driving insulin secretion up. A low C-peptide paired with a high glucose is a strong signal of insulin deficiency. Newly diagnosed type 1 patients often still have some measurable C-peptide during the "honeymoon" period, and sensitive assays show that a surprising number of people with long-standing type 1 diabetes retain a tiny but real amount of C-peptide production for years.
Type 2 diabetes: normal or high C-peptide
Type 2 diabetes is a problem of insulin resistance: the body's cells respond poorly to insulin, so the pancreas compensates by pumping out more. As a result, C-peptide in type 2 diabetes is typically normal or high, particularly earlier in the disease. A well-preserved or elevated C-peptide in someone with high blood sugar points toward type 2 rather than type 1. (Late in type 2 diabetes, after many years, beta cells can wear down and C-peptide may fall — which is one reason the test is most decisive when interpreted alongside the clinical picture.)
LADA: type 1 in slow motion
LADA stands for latent autoimmune diabetes in adults — sometimes called "type 1.5." It is a slowly progressing autoimmune diabetes that appears in adulthood and is frequently mislabeled as type 2 at first, because the person is an adult and does not need insulin right away. Over months to years, though, the autoimmune attack erodes insulin production. C-peptide, tracked over time, tends to show a gradual decline in LADA, and a falling or lower-than-expected C-peptide in an adult "type 2" who is thin or responding poorly to pills can be an important clue — usually confirmed by testing for diabetes-related autoantibodies.
MODY: an inherited form with preserved C-peptide
MODY (maturity-onset diabetes of the young) is a group of rare, single-gene forms of diabetes that run strongly in families and appear in adolescence or young adulthood. Unlike type 1, MODY is not autoimmune, and the beta cells keep working, so C-peptide is generally preserved (detectable and reasonably normal) even years after diagnosis — a pattern that helps distinguish MODY from type 1 diabetes. Recognizing MODY matters because some forms respond beautifully to low-dose sulfonylurea pills and do not need insulin at all. A persistent, measurable C-peptide in someone diagnosed young, with a strong family history and negative autoantibodies, is a reason to consider genetic testing for MODY.
For a hands-on interpretation, doctors often combine a random (non-fasting) C-peptide with a simultaneous glucose. Very low C-peptide with high glucose argues for type 1; a healthy C-peptide argues against it. Because the number varies with how recently a person ate and with kidney function, C-peptide is a piece of the puzzle rather than a stand-alone verdict.
Investigating Low Blood Sugar
One of C-peptide's most elegant uses is untangling why an adult is having spells of dangerously low blood sugar. When blood sugar falls, a healthy pancreas is supposed to switch insulin production off. So if someone is hypoglycemic and has high insulin at the same time, insulin is coming from somewhere it should not — and the key question is where. C-peptide answers it.
Insulinoma: high insulin and high C-peptide
An insulinoma is a rare tumor of the pancreas that secretes insulin without regard for the blood sugar level, causing repeated hypoglycemia. Because the tumor is part of the pancreas, it releases insulin the normal way — as proinsulin split into insulin and C-peptide. So in an insulinoma, when the blood sugar is low, both insulin and C-peptide are inappropriately high. The C-peptide confirms that the excess insulin is the body's own.
Injected insulin: high insulin but low C-peptide
Now consider hypoglycemia caused by injected (exogenous) insulin — whether an accidental overdose, a dosing error, or deliberate misuse. Manufactured insulin contains no C-peptide. So this person shows high insulin but low or suppressed C-peptide: the pancreas, sensing the low sugar, has correctly shut down its own production, dragging C-peptide down, even as the injected insulin keeps blood sugar low. This mismatch — high insulin, low C-peptide — is the classic fingerprint of insulin from outside the body, and it is exactly why C-peptide is indispensable here.
A third pattern rounds out the picture: hypoglycemia from sulfonylurea pills (medications that whip the pancreas into releasing more insulin) looks just like an insulinoma on paper — high insulin and high C-peptide — because the extra insulin is still endogenous. Doctors distinguish these by also screening the blood or urine for the drugs themselves. The Endocrine Society's guideline on hypoglycemia lays out the standard thresholds used during a supervised fast: when documented hypoglycemia occurs, an insulin level at or above roughly 3 µU/mL together with a C-peptide at or above about 0.6 ng/mL (0.2 nmol/L) indicates that the person's own pancreas is over-secreting insulin (as in an insulinoma or a sulfonylurea effect), whereas a suppressed C-peptide points to injected insulin.
Assessing Beta-Cell Reserve
"Beta-cell reserve" is a plain-language way of asking: how much insulin-making capacity does this pancreas have left? For someone with diabetes, that reserve shapes real decisions — whether pills are likely to keep working, how soon insulin might be needed, and how tightly the disease can be controlled. C-peptide is the practical way to gauge it.
Diabetes of most kinds is, over time, a story of declining beta-cell function. In type 2 diabetes, beta cells gradually falter after years of overwork; in type 1 and LADA, they are progressively destroyed. A C-peptide level captures a snapshot of what remains. A robust C-peptide says the pancreas still has meaningful capacity; a very low one says the tank is nearly empty and the person is dependent on the insulin they inject.
Sometimes a single resting measurement is not enough, because C-peptide naturally rises and falls with meals. To measure reserve more rigorously, clinicians and researchers use a stimulated test: they give a standardized challenge that should prompt the pancreas to release insulin, then measure the C-peptide response. The most common is the mixed-meal tolerance test, in which the person drinks a standardized nutritional shake and C-peptide is measured over the following couple of hours. A glucagon-stimulation test is an alternative. The peak C-peptide reached during stimulation is considered the gold-standard readout of functioning beta-cell mass, and it is the outcome measure used in clinical trials of therapies that aim to preserve insulin production in type 1 diabetes. For most everyday clinical questions, though, a simpler random C-peptide with a paired glucose is sufficient.
Reference Ranges & What Results Mean
A C-peptide result is reported as a concentration in the blood, usually in nanograms per milliliter (ng/mL) in the United States or nanomoles per liter (nmol/L) elsewhere. As a rough conversion, 1 ng/mL is about 0.33 nmol/L. The single most important rule for reading the number comes first:
A C-peptide result means little without the blood glucose measured at the same moment. The same value can be normal or alarming depending on the sugar it accompanies. A "normal-looking" C-peptide during an episode of low blood sugar is actually too high (the pancreas should have switched off), while a "normal-looking" C-peptide alongside very high glucose may be inappropriately low (the pancreas should have ramped up). Good labs and doctors always interpret the pair together.
Typical fasting range
Reference ranges vary from lab to lab depending on the assay, so always read the interpretation printed on your own report. As a broad orientation, a commonly cited fasting C-peptide reference range in adults is roughly 0.5 to 2.0 ng/mL (about 0.17 to 0.66 nmol/L), with some laboratories reporting an upper limit closer to 3 ng/mL. What matters is where your value sits relative to your lab's stated range and, again, what your glucose was doing.
Reading the result in context
- Low C-peptide with high glucose — suggests the pancreas is not making enough insulin (a pattern seen in type 1 diabetes, advanced LADA, or long-standing insulin-deficient diabetes).
- Normal or high C-peptide with high glucose — suggests the body is making insulin but not responding to it well (insulin resistance, the hallmark of type 2 diabetes).
- High C-peptide with low glucose — an inappropriate combination that raises concern for over-production of the body's own insulin (for example, an insulinoma or a sulfonylurea effect).
- Low or suppressed C-peptide with low glucose but high insulin — the signature of hypoglycemia driven by injected insulin from outside the body.
Because assays historically differed, laboratory scientists have worked to standardize C-peptide measurement so that a value means the same thing from one lab to another; this is part of why comparing a result to your own lab's current reference range — rather than a number you read online — is the reliable approach.
Factors That Affect the Result
Several things unrelated to beta-cell health can push a C-peptide value up or down. Knowing them prevents misreading a result.
- Kidney function. This is the big one. Unlike insulin, which the liver clears, C-peptide is removed from the blood mainly by the kidneys. When kidney function is reduced, C-peptide is cleared more slowly and accumulates, so the level in the blood rises. In someone with chronic kidney disease, a high C-peptide can therefore overstate how much insulin the pancreas is really making. Results in people with impaired kidneys have to be interpreted with this in mind.
- Whether you have eaten (fasting vs. fed). C-peptide is lower when fasting and rises after a meal as the pancreas responds to incoming carbohydrate. A fasting sample and a post-meal sample are not directly comparable, which is why the doctor specifies the conditions — and why a stimulated (post-meal) test is used when reserve needs to be measured carefully.
- Blood glucose at the time. As emphasized above, the prevailing glucose drives insulin (and therefore C-peptide) secretion. A high glucose normally raises C-peptide; a low glucose should suppress it. The value is only interpretable next to the simultaneous sugar.
- Certain medications. Drugs that stimulate insulin release — notably sulfonylureas and related pills — raise C-peptide, which is important context when investigating hypoglycemia. Some other medications and hormonal states can nudge the level as well.
- Severe liver disease and other illness. Because the metabolism of insulin and glucose is altered in serious illness, C-peptide can be affected indirectly; results during acute illness may not reflect the person's usual state.
None of these make the test unreliable — they simply mean the number is read in context. Kidney function in particular is worth asking your doctor about if your C-peptide comes back higher than expected.
How the Test Is Done & How to Prepare
The C-peptide test is a standard blood draw. A technician takes a sample from a vein in your arm, and it is sent to a lab. There is nothing about the procedure itself that differs from any other blood test.
Preparation depends entirely on why the test is being done, so follow your own doctor's instructions — they are not one-size-fits-all:
- Fasting. For many purposes, especially assessing baseline production, you may be asked to fast (nothing but water) for a number of hours beforehand, often overnight, so that the sample reflects your resting insulin output rather than a response to a recent meal.
- Random (non-fasting) with glucose. In other situations — such as classifying diabetes — a random C-peptide drawn together with a glucose is convenient and informative, and no fasting is required. The paired glucose is what makes the C-peptide interpretable.
- Stimulated testing. If beta-cell reserve is being measured, the test may be a mixed-meal or glucagon-stimulation protocol, where you drink a standardized shake (or receive an injection of glucagon) and blood is drawn at set intervals afterward. These take longer and are done under supervision.
- Supervised fast for hypoglycemia. When the question is unexplained low blood sugar, the definitive test is a monitored fast (sometimes up to 72 hours in a hospital) during which glucose, insulin, and C-peptide are measured together the moment symptoms or a low sugar occur.
Tell your care team about all medications and supplements you take, including any insulin or diabetes pills, and ask whether to adjust them before the test — do not stop prescribed medication on your own. Because the interpretation hinges on the paired glucose and on your kidney function and clinical story, the most valuable thing you can do is review the result with the doctor who ordered it rather than judging the raw number alone.
Research Papers
- Jones AG, Hattersley AT. The clinical utility of C-peptide measurement in the care of patients with diabetes. Diabetic Medicine. 2013;30(7):803–817. doi:10.1111/dme.12159 — A widely cited review of how and when C-peptide should be used in everyday diabetes care, including type classification and interpreting the result alongside glucose.
- Leighton E, Sainsbury CA, Jones GC. A practical review of C-peptide testing in diabetes. Diabetes Therapy. 2017;8(3):475–487. doi:10.1007/s13300-017-0265-4 — A clinician-friendly summary of practical thresholds and testing conditions for using C-peptide to guide treatment decisions.
- Cryer PE, Axelrod L, Grossman AB, Heller SR, Montori VM, Seaquist ER, et al. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism. 2009;94(3):709–728. doi:10.1210/jc.2008-1410 — The reference guideline defining the insulin and C-peptide thresholds used to work up hypoglycemia, including insulinoma versus injected insulin.
- Service FJ. Hypoglycemic disorders. New England Journal of Medicine. 1995;332(17):1144–1152. doi:10.1056/NEJM199504273321707 — A classic review explaining how C-peptide distinguishes endogenous hyperinsulinism (insulinoma) from factitious hypoglycemia caused by exogenous insulin.
- Buzzetti R, Zampetti S, Maddaloni E. Adult-onset autoimmune diabetes: current knowledge and implications for management. Nature Reviews Endocrinology. 2017;13(11):674–686. doi:10.1038/nrendo.2017.99 — A review of LADA ("type 1.5"), where a gradual decline in C-peptide helps separate slowly progressing autoimmune diabetes from type 2.
- Shields BM, McDonald TJ, Ellard S, Campbell MJ, Hyde C, Hattersley AT. The development and validation of a clinical prediction model to determine the probability of MODY in patients with young-onset diabetes. Diabetologia. 2012;55(5):1265–1272. doi:10.1007/s00125-011-2418-8 — Shows how preserved C-peptide (and other clinical features) helps flag inherited MODY, which is often misdiagnosed as type 1 or type 2.
- Palmer JP, Fleming GA, Greenbaum CJ, Herold KC, Jansa LD, Kolb H, et al. C-peptide is the appropriate outcome measure for type 1 diabetes clinical trials to preserve beta-cell function. Diabetes. 2004;53(1):250–264. doi:10.2337/diabetes.53.1.250 — An American Diabetes Association workshop report establishing C-peptide as the standard measure of surviving beta-cell function.
- Weir GC, Bonner-Weir S. Five stages of evolving beta-cell dysfunction during progression to diabetes. Diabetes. 2004;53(suppl 3):S16–S21. doi:10.2337/diabetes.53.suppl_3.s16 — A conceptual framework for how beta-cell capacity — the "reserve" that C-peptide reflects — declines as diabetes develops.
- Little RR, Rohlfing CL, Tennill AL, Madsen RW, Polonsky KS, Myers GL, et al. Standardization of C-peptide measurements. Clinical Chemistry. 2008;54(6):1023–1026. doi:10.1373/clinchem.2007.101287 — Documents efforts to harmonize C-peptide assays so a result means the same thing across laboratories — the basis for trusting reference ranges.
- Besser REJ, Shields BM, Casas R, Hattersley AT, Ludvigsson J. Lessons from the mixed-meal tolerance test. Diabetes Care. 2013;36(2):195–201. doi:10.2337/dc12-0836 — Examines the stimulated (mixed-meal) C-peptide test used to measure beta-cell reserve more rigorously than a resting sample.
Connections
- Fasting Insulin
- Hemoglobin A1C
- Continuous Glucose Monitoring
- Type 2 Diabetes
- Type 1 Diabetes
- Insulinoma
- All Lab Tests